
Systemic sclerosis (SSc) is characterized by excess collagen deposition in multiple organs, resulting in dilatation of intestine, delayed transit, chronic intestinal pseudoobstruction (CIPO), and bacterial overgrowth.1
A 58-year-old woman with a 2-year history of SSc presented with alternating diarrhea and constipation. On examination, the abdomen was distended, tympanitic, and nontender, with decreased bowel sounds. Abdominal supine radiograph showed the distended small intestine (Supplementary Figure 1, available with the online version of this article). Computed tomography disclosed marked dilatation of the small intestine with narrow separation between the valvulae conniventes (Kerkring folds), presenting the “hide-bound” bowel sign (Figure 1 and Figure 2). The patient was diagnosed with CIPO associated with SSc and was treated conservatively with mosapride, a serotonin 5-hydroxytryptamine4 receptor agonist.

A scout view of computed tomography showed marked dilatation of the small intestine with narrow separation between valvulae conniventes, presenting the “hide-bound” bowel sign (arrows).
{kind=link}
{kind=link}
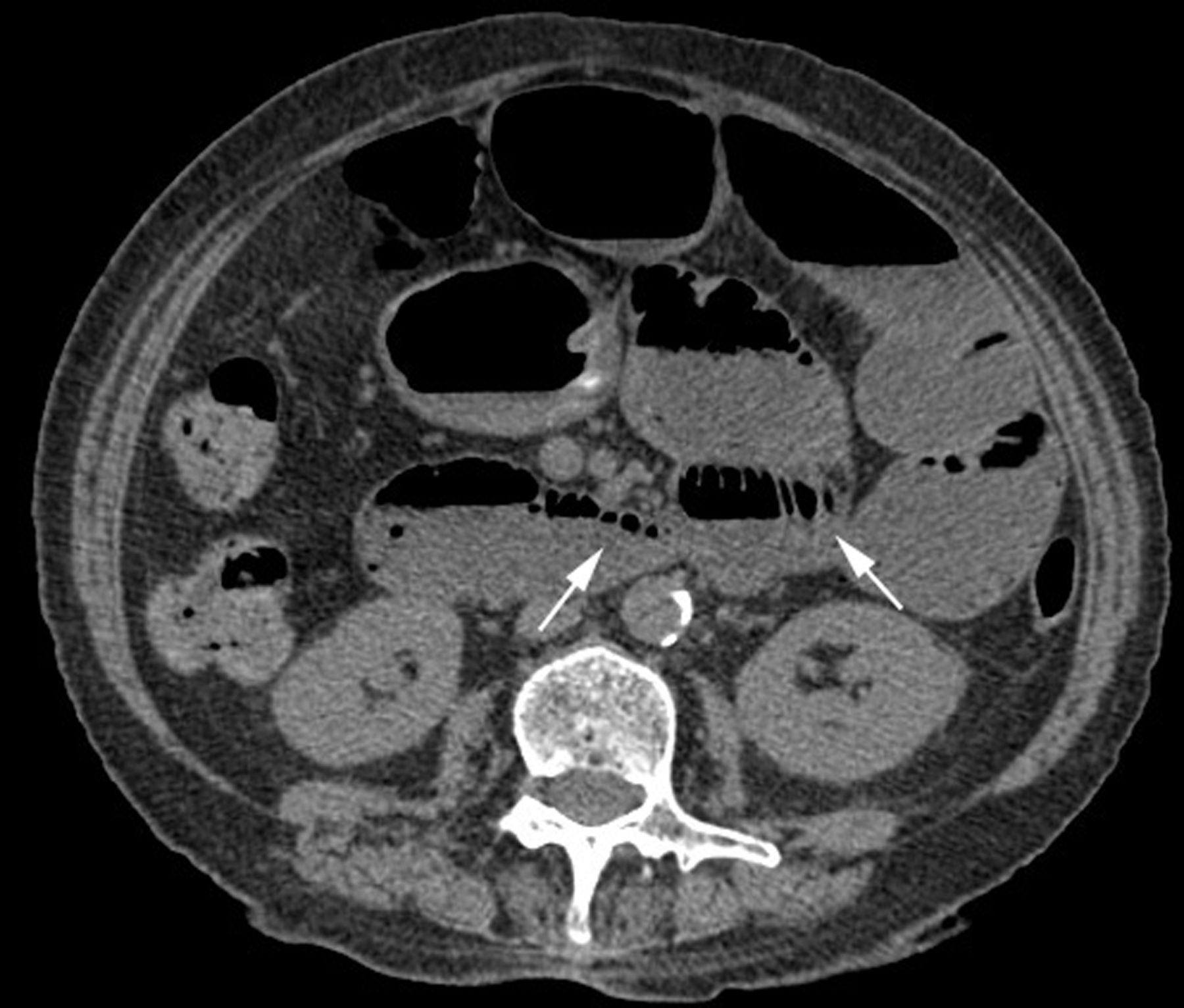
An axial computed tomography scan showed dilatated small intestine with air-fluid levels and the “hide-bound” bowel sign (arrows).
Although the etiology of the hide-bound bowel sign remains unclear, reasonably preserved function of the outer longitudinal layer relative to the inner circular layer may illustrate narrow separation between valvulae conniventes despite bowel dilation. One hypothesis is the predominant muscular atrophy and collagenous replacement of the longitudinal layer relative to the circular layer.2 The term hide-bound was originally used to describe a cutaneous manifestation of SSc that give the appearance similar to the skin of lean cattle. Although SSc-related CIPO is often refractory, octreotide—a somatostatin analog—has provided some beneficial effects for intestinal dysmotility in SSc.1,3
Footnotes
Ethics board approval was not required because this is a single case report and no intervention had been made for research. The patient’s written informed consent to publish the report was obtained.
- Copyright © 2022 by the Journal of Rheumatology
REFERENCES
- 1.
- 2.
- 3.