
Abstract
Objective. To explore the burden of skin, joint, and entheses manifestations in a representative psoriatic arthritis (PsA) outpatient cohort in the biologic treatment era.
Methods. This was a cross-sectional study of 141 PsA outpatients fulfilling the ClASsification for Psoriatic ARthritis (CASPAR) criteria and examined between January 2013 and May 2014. Selected disease activity measures were explored including Disease Activity index for PSoriatic Arthritis (DAPSA), Composite Psoriatic Disease Activity Index (CPDAI), Psoriatic Arthritis Disease Activity Score (PASDAS), Disease Activity Score for 28 joints (DAS28), Simplified Disease Activity Index (SDAI), and Psoriasis Area Severity Index (PASI). Dermatology Life Quality Index (DLQI), minimal disease activity (MDA), and remission criteria were assessed.
Results. Median (range) DAPSA was 14.5 (0.1–76.4), CPDAI 5 (1–11), PASDAS 3.1 (2.1–4.2), DAS28-erythrocyte sedimentation rate (ESR) 3.2 (0.6–6.4), SDAI 8.6 (0.1–39.5), PASI 1.2 (0.0–19.7), and DLQI 2.0 (0–17). The MDA criteria were fulfilled by 22.9% of the patients. DAPSA ≤ 4, CPDAI ≤ 2, PASDAS < 2.4, DAS28-ESR < 2.4, SDAI < 3.3, and Boolean’s remission criteria were fulfilled by 12.1, 9.3, 7.8, 26.2, 21.3, and 5.7% of patients, respectively. The number of satisfied patients was similar regardless of whether the group was treated with tumor necrosis factor inhibitors.
Conclusion. Our real-life data indicate that there is still a need for improvement in today’s treatment of PsA. Musculoskeletal inflammatory involvement was more prominent than psoriatic skin involvement. Only a few patients fulfilled the DAPSA, PASDAS, and CPDAI remission criteria, and about a quarter fulfilled the MDA criteria. Considerably fewer patients fulfilled PsA-specific remission criteria versus non-PsA specific remission criteria. Still, patient satisfaction was good and PASI and DLQI were low.
- PSORIATIC ARTHRITIS
- DISEASE BURDEN
- REMISSION
Psoriatic arthritis (PsA) is a heterogeneous and complex systemic disease that involves mainly the body surface (skin and nails) and the musculoskeletal system (e.g., joints, tendons, and entheses)1. In patients with PsA, quality of life has been found to be poorer than in patients with psoriasis alone2,3. In the literature there is a paucity of broad-based studies on the burden of skin and musculoskeletal manifestations in PsA outpatients, including recently developed composite scores for PsA4. During the last decade, the treatment possibilities in PsA have been vastly improved with the introduction of biologic disease-modifying antirheumatic drugs (bDMARD), which have led to far better disease outcomes5,6. The treat-to-target strategy, which has been demonstrated to improve clinical outcomes in rheumatoid arthritis (RA)7, has also been advocated for use in PsA8,9.
Over the years there has been an increased awareness of the potentially devastating nature of PsA3,10. We have previously reported data indicating that disease perception, i.e., pain, may be worse in PsA than in RA11.
In accordance with recommendations from the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA)12, PsA-specific composite scores reflecting the heterogenic nature of the disease have been developed. The Disease Activity Index for Psoriatic Arthritis (DAPSA)13 is joint-focused. The Psoriatic Arthritis Disease Activity Score (PASDAS)14 includes entheses and dactylitis, as well as joints. The Composite Psoriatic Disease Activity Index (CPDAI)15 is a 5-component score including joints, entheses, dactylitis, axial skeleton, and skin.
Composite scores initially developed for rheumatoid arthritis (RA) are also common in the evaluation of disease activity in PsA, i.e., the Simplified Disease Activity Index (SDAI)16, Clinical Disease Activity Index (CDAI)16, and Disease Activity Score for 28 joints (DAS28)17.
For assessment of skin disease, the Psoriasis Area Severity Index (PASI)18 is the best-validated and most frequently used score in PsA, although it is mainly used in trials19. The Dermatology Life Quality Index (DLQI)20 is used for a number of dermatological conditions including PsA to measure disability related to skin disease.
Criteria for minimal disease activity (MDA) in PsA have been established21, and recently DAPSA remission criteria were defined, although they are debated22,23. CPDAI and PASDAS remission criteria have been proposed, but not yet validated4,24.
In our present study we aimed to explore the burden of skin, joint, and entheses manifestations, as well as patient-reported outcome measures (PRO) in a representative PsA outpatient cohort in the biologic treatment era.
MATERIALS AND METHODS
Patients
In total, there were 581 patients with PsA registered in the outpatient clinic of the Hospital of Southern Norway Trust, Norway, during the study period from January 2013 to May 2014, of whom 471 fulfilled the ClASsification for Psoriatic ARthritis criteria (CASPAR)25. Of these 471 patients, 141 were included in the study in a random manner at consecutive clinic visits. All the included patients had to be 18 years or older and have a history of peripheral inflammatory involvement clinically (peripheral arthritis and/or enthesitis). Patients diagnosed as having only axial spondyloarthritis were excluded. The study was approved by the Norwegian Regional Committees for Medical and Health Research Ethics (Regional komité for Medisinsk og helsefaglig forskningsetikk Midt-Norge 2012/101), and written informed consent was obtained from each patient.
Assessment of disease activity
Main clinical assessments were previously reported26. Patients registered demographics and PRO in the computer system, GoTreatIT Rheuma27, including Modified Health Assessment Questionnaire (MHAQ)28 (range 0–3), Bath Ankylosing Spondylitis Disease Activity Index (BASDAI, range 0–10)29, Bath Ankylosing Spondylitis Functional Index (BASFI, range 0–10)30, DLQI (range 0–30), Rheumatoid Arthritis Impact of Disease (RAID, range 0–10)31, and Patient Acceptable Symptom State (PASS)32. C-reactive protein (CRP, mg/l) and erythrocyte sedimentation rate (ESR, mm/h) were assessed. Two specially trained nurses performed 66/68 tender/swollen joint count (TJC/SJC), dactylitis count, Maastricht Ankylosing Spondylitis Enthesitis Score33 (MASES, range 0–13, including first and seventh costosternal joints, anterior superior iliac spine, iliac crest, fifth lumbar spinous process, posterior superior iliac spine, and Achilles), as well as 16 other entheses (lateral and medial epicondyle, triceps, great trochanter, quadriceps, proximal and distal patellar tendons, plantar fasciae), and PASI (range 0–72). The presence of enthesitis was defined as tenderness on firm palpation. Visual analog scales for evaluator’s global assessment of disease activity (EGA) and patient’s global assessment of disease activity (PtGA), pain, joint pain, fatigue, morning stiffness, and back pain were recorded (range 0–100 mm, 100 mm worst assessment).
SDAI, DAS28-ESR, DAS28-CRP, and DAPSA scores were calculated. Modified versions of PASDAS (including EGA, PtGA, MHAQ, SJC66, TJC68, MASES, dactylitis count, and CRP) and CPDAI (including 66/68 joint count, MHAQ, PASI, DLQI, MASES, dactylitis count, BASDAI, and RAID) as well as CPDAI joint, entheses, and dactylitis domains (CPDAI-JED) were calculated (Supplementary Table 1, available with the online version of this article). In the PASDAS and CPDAI calculations we used MHAQ instead of HAQ34/SF-36 PCS (physical component summary score of the Medical Outcomes Study Short Form-36)35, RAID instead of ASQoL (Ankylosing Spondylitis Quality of Life)36, and MASES instead of Leeds enthesitis index37, because MHAQ, RAID, and MASES but not HAQ, SF-36 PCS, ASQoL, or Leeds enthesitis index were assessed in our study. The presence of erosions on radiographs of hands and feet was assessed by a radiologist as part of general care.
The patients were classified as achieving MDA when meeting 5 of the 7 following criteria21: (1) TJC ≤ 1, SJC ≤ 1, PASI ≤ 1, pain ≤ 15 (0–100 scale), PtGA ≤ 20 (0-100 scale), MHAQ ≤ 0.5, and MASES ≤ 1; (2) DAPSA ≤ 4.022; (3) CPDAI ≤ 2 and CPDAI-JED = 024; (4) PASDAS < 2.44; (5) a Boolean’s definition of remission modified for PsA, meeting all of the following: TJC ≤ 1, SJC ≤ 1, MASES ≤ 1, dactylitis count ≤ 1, EGA ≤ 1 (0–10 scale), PtGA ≤ 1 (0–10 scale), CRP ≤ 1 mg/dl; (6) DAS28 < 2.44; and (7) SDAI < 3.34.
PRO, disease activity measures, and medication data from the last visit during the study period were compared between the included patients (n = 141) and the rest of the PsA cohort fulfilling the inclusion criteria (n = 330). The data included demographics, 28 TJC and SJC, MHAQ, ESR, CRP, EGA, PtGA, joint pain, fatigue, morning stiffness, body mass index (BMI), CDAI, DAS28, and current use of conventional synthetic DMARD (csDMARD), tumor necrosis factor inhibitors (TNFi), and steroids.
Statistical analyses
Statistical analyses were performed using IBM SPSS Statistics version 21.0.0.2 as well as STATA statistical software version 14 (Fisher’s exact test). Descriptive statistics were used to calculate patients’ demographic variables. The median and range were calculated for nonparametric data and the mean and SD for parametric data. Proportions were analyzed using the chi-square test or Fisher’s exact test as appropriate. Quantitative results were compared using the Mann-Whitney U test (nonparametric distribution of the data). Correlation analyses were performed by Spearman’s rank correlation test (nonparametric distribution of the data).
RESULTS
Clinical findings
The 141 included patients had a mean (SD) age of 52.4 (10.2) years, disease duration 9.5 (6.6) years, education duration 13.0 (3.3) years, BMI 28.3 (4.3) kg/m2. In addition, 50.4% were women, 17.0% current smokers, 51.8% previous smokers, 53.2% currently had paid work, and 26.6% had erosive disease.
At inclusion, 15 patients (10.6%) were using glucocorticoid, 53 (37.6%) csDMARD monotherapy, 18 (12.8%) bDMARD monotherapy, and 28 (19.9%) both csDMARD and bDMARD treatment.
A comparison of the characteristics of the 141 included and 330 excluded patients with PsA (for whom less extensive data were available) at their last visit at the outpatient clinic is displayed in Supplementary Table 2, available with the online version of this article. No statistically significant differences were found between the included and excluded patients, apart from age, 28 TJC, DAS28, CDAI, and current use of steroids.
Composite scores
PRO, inflammatory markers, and composite scores of disease activity are listed in Table 1. CPDAI categories are displayed in Table 2. Active arthritis was found in 128 patients (90.8%), active skin disease in 127 (90.0%; 1 missing), enthesitis in 95 (67.4%), dactylitis in 1 (0.7%), and active spondylitis in 11 (7.8%). On the 66/68 joint count, 126 patients (89.4%) had ≥ 1 TJ and 52 (36.9%) ≥ 1 SJ. On MASES count, 95 patients (67.4%) presented ≥ 1 painful entheseal site. Median (range) DAPSA was 14.5 (0.1–76.4), CPDAI 5.0 (1.0–11.0), CPDAI-JED 4 (0–6), and PASDAS 3.1 (2.1–4.2).
Patient-reported outcome measures, inflammatory markers, and composite scores of disease activity (n = 141).
Modified Composite Psoriatic Disease Activity Index (CPDAI) categories. All data are n (%).
The different PsA-specific composite scores were moderately to highly correlated (p < 0.001): CPDAI and DAPSA (ρ= 0.77), CPDAI and PASDAS (ρ= 0.63), and DAPSA and PASDAS (ρ= 0.54). Respectively, DAPSA, CPDAI, and PASDAS were highly to moderately correlated to DAS28-CRP (ρ= 0.85, 0.65, 0.46), SDAI (ρ= 0.89, 0.70, 0.46), and MHAQ (ρ= 0.61, 0.77, 0.56), all with p < 0.001.
PASI < 3, the lower limit for reliability of the score, was found in 105 (74.3%) patients.
DLQI ≤ 1, indicating no effect at all on patient’s life, was reported by 59 patients (41.8%), and DLQI ≤ 5, indicating no or small effect on a patient’s life, by 109 patients (77.3%). DLQI and PASI were moderately correlated (ρ= 0.55, p < 0.001).
MHAQ ≤ 0.5 was found in 94 (66.7%), MHAQ ≤ 1 in 134 (95%), and RAID ≤ 2 in 39 patients (27.9%). RAID was strongly correlated to MHAQ (ρ= 0.71) and moderately to DLQI (ρ= 0.32, p < 0.001).
PASS was reported as acceptable by 76.3% of the patients. Patient-reported change of condition compared to the previous visit at the outpatient clinic was reported as worse, the same, better, or much better by 6.3%, 73.4%, 16.1%, and 1.4% of the patients, respectively. No difference in the number of patients considering the status actually acceptable was found when comparing patients currently treated with or without bDMARD (73.9% vs 77.4%, p = 0.648) and csDMARD (79.7% vs 71.7%, p = 0.267).
Patients finding the status acceptable showed significantly lower DAPSA (−12.7), CPDAI (−2.0), PASDAS (−0.3), Boolean’s (−7.6), DAS28-ESR (−0.9), DAS28-CRP (−0.9), and SDAI (−6.9) compared to patients who did not report the status as acceptable (p ≤ 0.002).
MDA and remission criteria
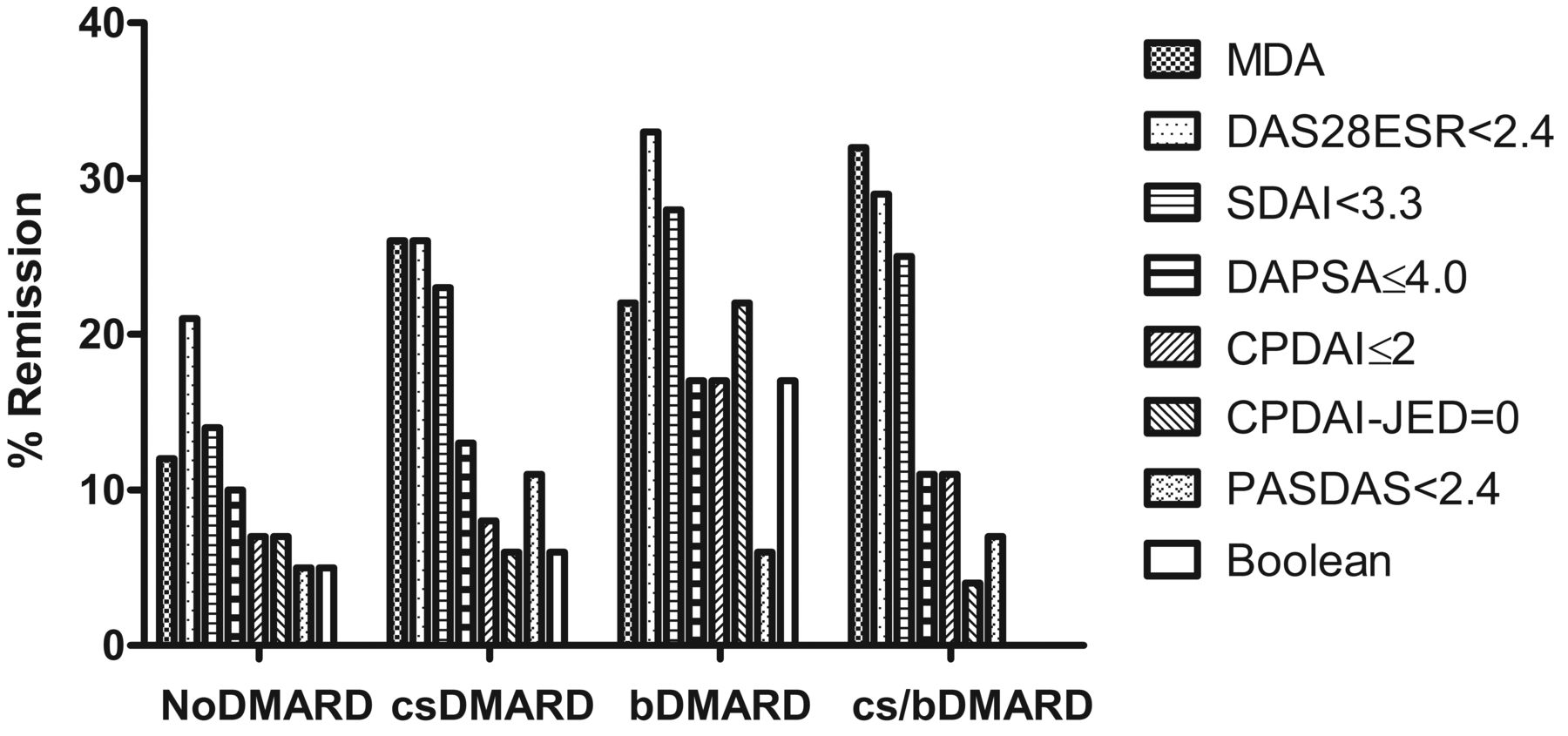
The percentages of patients fulfilling the remission criteria and the MDA criteria are displayed in Table 3. According to the composite scores specifically developed for PsA, about 1 in 10 patients were in remission, while a considerably higher proportion of the patients were in remission according to the composite scores initially developed for RA. The percentages of patients fulfilling the remission criteria and the MDA criteria according to different treatment regimens are displayed in Figure 1. The percentages of patients in remission were similar in the bDMARD group compared with the cs/bDMARD group. A trend was seen toward higher percentages of patients in remission among patients treated with bDMARD compared with csDMARD and without DMARD.
{kind=link}
Percentage of patients fulfilling the remission criteria and the minimal disease activity (MDA) criteria according to different treatment regimens. DAS28-ESR: 28-joint Disease Activity Score with erythrocyte sedimentation rate; SDAI: Simplified Disease Activity Index; DAPSA: Disease Activity index for Psoriatic Arthritis; CPDAI: Composite Psoriatic Disease Activity Index; CPDAI-JED: CPDAI joint, entheses, and dactylitis domains; PASDAS: Psoriatic Arthritis Disease Activity Score; DMARD: disease-modifying antirheumatic drugs; csDMARD: conventional synthetic DMARD; bDMARD: biologic DMARD.
Patients fulfilling minimal disease activity and remission criteria according to type of treatment (n = 141). Chi-squared or Fisher’s exact test were used, as appropriate. Except for p values, data are n (% of DMARD category).
DISCUSSION
Remission is the main goal in modern treatment of inflammatory joint disorders including PsA9,38. Still, only a few of the PsA patients fulfilled the DAPSA, CPDAI, CPDAI-JED, PASDAS, and Boolean’s remission criteria, and only about one-quarter met MDA criteria.
CPDAI is the only PsA-specific composite score covering all the main disease entities, giving a detailed overview of disease activity. Although DAPSA is primarily joint-focused and PASDAS covers joints, dactylitis, and entheses but not skin and axial disease, the number of patients in remission was similar according to CPDAI, CPDAI-JED, DAPSA, and PASDAS.
In contrast, DAS28 and SDAI remission criteria were fulfilled by considerably more patients. This could partly be attributed to DAS28 and SDAI including 28 and not a 66/68 joint count, in contrast to CPDAI, DAPSA, and PASDAS, which all include the 66/68 joint count.
Our findings are supported by a study exploring the discriminative capacity of composite scores in PsA also reporting DAPSA, CPDAI, and PASDAS, to show more stringent definitions of remission compared to DAS28 and SDAI in PsA4. Interestingly, the MDA criteria were fulfilled by a percentage of patients similar to those who fulfilled the DAS28 and SDAI remission criteria. It is important to be aware that while the MDA criterion is validated for PsA21, the recent validation of the DAPSA remission criterion (≤ 4) for PsA is being debated22,23, while the cutoff values for PASDAS (< 2.4), CPDAI (≤ 2), CPDAI-JED (0), DAS28 (< 2.4), and SDAI (< 3.3) remission are proposed but not validated for PsA4,24. There was a trend toward higher percentages of patients in remission among the bDMARD-treated patients compared with the patients without DMARD treatment or with csDMARD monotherapy (Figure 1).
In contrast to the low number of patients who fulfilled the remission criteria, the 66 SJC was low. SJC is easy to perform and valuable for impartial evaluation of arthritis. Patient global assessment and TJC are included in all the mentioned composite scores and are often considerably higher than evaluator’s global assessment and SJC, respectively39. PRO may be influenced by psychosocial factors and may pose error sources in the evaluation of disease activity through composite scores40. Nevertheless, PRO are of unquestionable importance in the evaluation of the total disease burden in inflammatory arthritides41.
According to DLQI, psoriatic skin disease had little or no effect on quality of life for a majority of patients. This is in accordance with the low scoring of PASI in this cohort, with a majority of the patients having PASI lower than the reliability limit set for this score. Health-related quality of life (HRQOL) according to MHAQ and RAID was also good in our population.
Only about half of the patients had paid work at the time of the study. This is consistent with previous studies in PsA42.
A limitation of our study is the cross-sectional design, allowing evaluation of disease burden in only 1 visit. On the other hand, the strength of our study is the evaluation of the total disease burden in a real-life cohort of patients with PsA from the outpatient clinic, including recently developed PsA-specific composite scores.
In a recent study we showed that the proportion of patients in remission in our RA outpatient clinic cohort was as high as 55.5% for DAS28-ESR remission, 31.7% for SDAI remission, and 17.7% for Boolean remission27. These figures are considerably higher than the remission figures seen in PsA in this study. This may be explained by higher perceptions of pain and patient global assessment in PsA compared to RA, as previously reported11. However, it is questionable whether the use of DAS28 and SDAI remission criteria is justified in PsA because of the clinical complexity and heterogeneity seen in this disease, as well as the exclusion of the feet in the 28-joint count included in these composite scores.
The treatment options in PsA have been revolutionized in the last decade with the introduction of TNFi. Yet, a substantial proportion of patients do not receive satisfactory results from TNFi. In recent years, several other new and promising treatment options have been developed43. In our study, about a third of the patients were currently under TNFi treatment.
PASS was reported as acceptable by a majority of the patients, and a vast majority reported change in condition since the last visit as the same, better, or much better. A previous study has reported cutpoints for PASS to correspond to an HRQOL far from perfect health44. The number of satisfied patients was similar in the groups receiving and not receiving TNFi treatment.
PsA is a heterogeneous disease and evaluation of disease activity remains challenging. Whether the available composite scores sufficiently reflect disease activity in PsA remains to be explored in future studies. Further, there is a need for validated remission criteria in PsA.
Our real-life data indicate a continuing need for improvement in today’s treatment of PsA. Musculoskeletal inflammatory involvement was more prominent than psoriatic skin involvement. Only a few patients fulfilled the DAPSA, PASDAS, and CPDAI remission criteria and about a quarter the MDA criteria. Considerably fewer patients fulfilled PsA-specific versus non–PsA-specific remission criteria. Still, patient satisfaction was good and PASI and DLQI were low.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
Acknowledgment
The authors thank the patients for participating in our study and the local rheumatology staff for data collection.
Footnotes
Funded by an unrestricted grant from Pfizer (GH). Clinical research fellowship from the Hospital of Southern Norway Trust (BM).
- Accepted for publication December 5, 2016.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.