
Abstract
Objective. The objective of these posthoc analyses was to evaluate short-term clinical outcomes as predictors of poor response after 1 year of treatment with combination etanercept/methotrexate (ETN/MTX) therapy versus MTX monotherapy in patients with early rheumatoid arthritis (RA).
Methods. Participants with moderate to severe RA [28-joint Disease Activity Score-Erythrocyte Sedimentation Rate (DAS28-ESR) ≥ 3.2] of 3–24 months’ duration received ETN 50 mg weekly plus MTX or MTX monotherapy for 52 weeks. Regression analyses were performed to evaluate the likelihood of remission (DAS28-ESR < 2.6) after 1 year despite poor clinical short-term treatment effects (e.g., absolute or changes from baseline in DAS28-ESR after 4, 8, 12, 20, and 24 weeks of therapy).
Results. The magnitude of disease activity and its improvement and timing influenced remission probability in both treatment groups; remission rate was diminished with higher disease activity levels and lower response levels over time from weeks 4 to 24. The rate of DAS28-ESR remission at 1 year was generally greater with ETN/MTX than with MTX alone at most timepoints from weeks 4 to 24. Despite persistent high disease activity (DAS28-ESR > 5.1) after 4, 8, 12, and 24 weeks of therapy, 35%, 27%, 25%, and 22% of patients, respectively, in the ETN/MTX group achieved DAS28-ESR remission after 1 year of continuous treatment; the respective proportions were 33%, 27%, 8%, and 13% in the MTX group.
Conclusion. High disease activity and less improvement with treatment over time in the initial 24 weeks of treatment, particularly after 12 weeks, were predictive of a lower remission rate after 1 year.
- EARLY RHEUMATOID ARTHRITIS
- TREATMENT
- BIOLOGIC AGENTS
- ETANERCEPT
- METHOTREXATE
- REMISSION
Sustained active inflammation in patients with rheumatoid arthritis (RA) may result in irreversible joint damage, even early in the disease course1,2. As a result, to prevent structural deterioration and minimize disability, the essential goal of RA treatment is prompt achievement of clinical remission or, alternatively, low disease activity in patients with longstanding disease3. Current European League Against Rheumatism (EULAR) guidelines4 support an early start of treatment with synthetic disease-modifying antirheumatic drugs (DMARD) in patients diagnosed with RA, which will provide remission or very low disease activity in a substantial proportion of patients, and with the addition of biologic agents if the treatment target is not initially achieved. First-line use of biologic agents combined with a DMARD may be considered in DMARD-naive patients who have symptoms of very aggressive disease, such as high disease activity or early joint damage. EULAR recommendations also suggest that clinicians closely monitor patient response and consider a change in the therapeutic regimen if disease activity persists after 3 to 6 months of treatment. Adjustment of treatment that has not adequately controlled active disease in that time frame may help reduce the risk of permanent joint damage, although the potential exists for premature discontinuation of treatment that may ultimately provide clinical benefit.
Prompt identification of patients who are unlikely to achieve longterm response to RA treatment based on short-term control of disease activity is a clinically relevant strategy that may facilitate early adjustment of treatment regimens to achieve the desired treatment target. However, relatively little is known about factors (measured when treatment is initiated or early in the treatment course) that reliably predict subsequent outcomes. Such information is crucial to the patient’s and/or clinician’s ability to make decisions regarding the benefits and risks of modifying therapy early in the treatment course.
In COMET (COmbination of Methotrexate and ETanercept in Active Early Rheumatoid Arthritis; Clinicaltrials.gov number NCT00195494), a double-blind, randomized, multicenter study, Emery, et al5 demonstrated that patients with active early RA who received combination etanercept/methotrexate (ETN/MTX) therapy for 1 year had greater reduction of disease activity and higher rates of clinical remission than did their counterparts who received MTX alone. In the posthoc analyses reported here, findings from the COMET study were used to assess whether and which short-term clinical outcomes were predictive of a poor clinical response after 1 year of treatment with either ETN combination therapy or MTX monotherapy in patients with early, aggressive RA.
MATERIALS AND METHODS
A detailed description of the participants, study design, and primary results of the COMET study has been published5. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki. All patients signed an approved informed consent form prior to participation.
Patients
In brief, eligible patients were aged at least 18 years and had adult-onset RA diagnosed according to the American College of Rheumatology 1987 revised criteria6. Participants had moderate to severe disease activity of 3 to 24 months’ duration at baseline, as defined by Disease Activity Score (DAS) based on 28-joint count and erythrocyte sedimentation rate (ESR), i.e., DAS28-ESR ≥ 3.2, and Westergren ESR ≥ 28 mm/h or C-reactive protein (CRP) ≥ 20 mg/l. All patients were MTX-naive and biologic-naive.
Study design
During the first year of the study, patients were randomly assigned to receive combination therapy of ETN 50 mg once weekly (QW) plus MTX or MTX alone. In both groups, all patients received an initial MTX dose of 7.5 mg QW, which, in patients with tender or swollen joints, was titrated over 8 weeks up to a maximum of 20 mg QW.
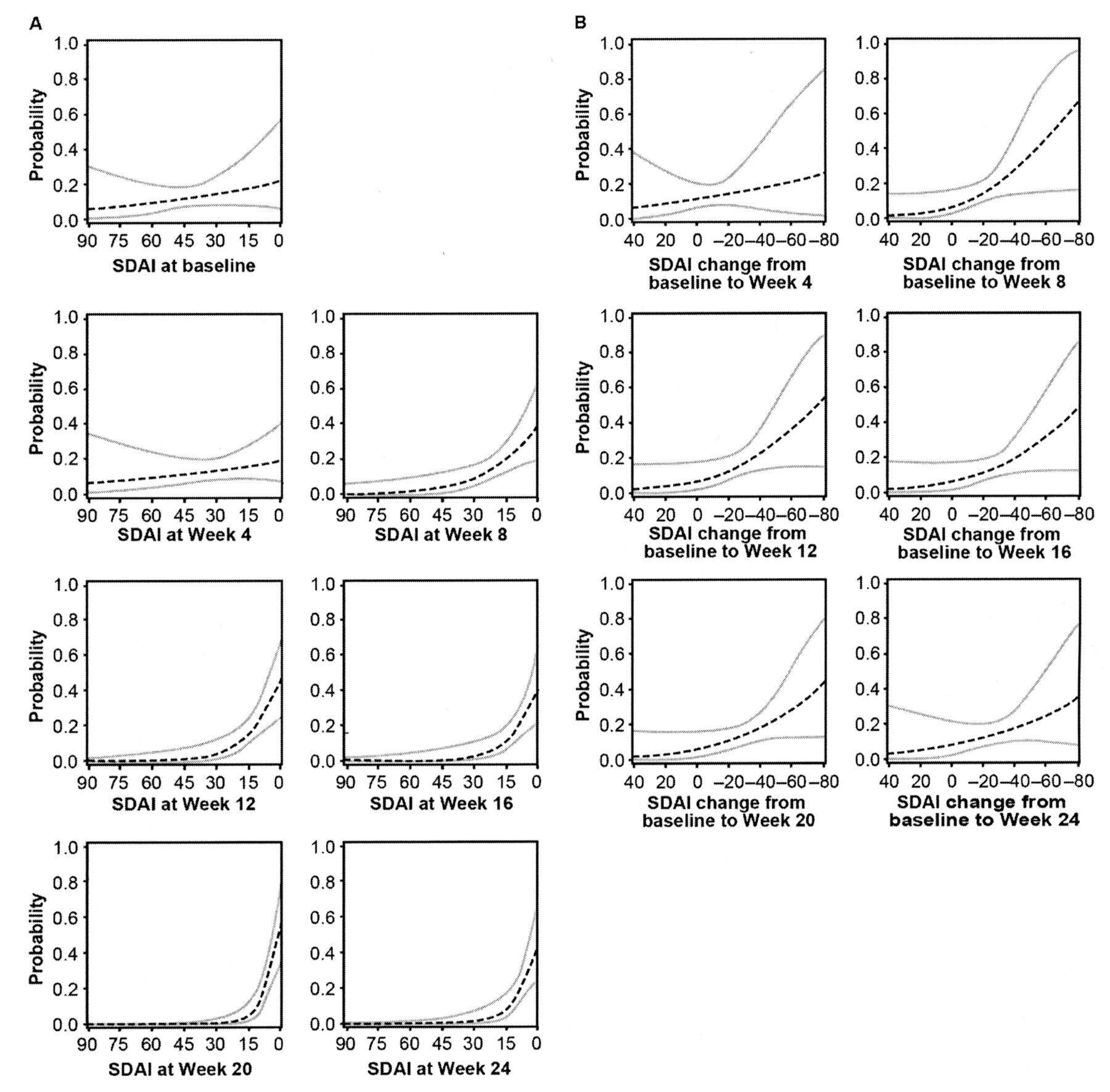
Posthoc analyses were conducted using observed data from patients who had 1 year of followup to assess the relationship between short-term disease activity and treatment response and the longterm rate of remission. The proportion of patients in each treatment group who achieved DAS28-ESR remission (< 2.6)7 at 1 year was calculated in the subpopulation of patients having predefined levels of (1) absolute DAS28-ESR values at baseline and weeks 4, 8, 12, 16, 20, and 24; and (2) changes in DAS28-ESR from baseline to weeks 4, 8, 12, 16, 20, and 24. A similar sensitivity analysis was conducted using remission based on the Simplified Disease Activity Index (SDAI ≤ 3.3) at 1 year, with the absolute SDAI values and changes in SDAI at weeks 4, 8, 12, 16, 20, and 24 used to predict such remission (Appendices 1–5).
Statistical analysis
Separate logistic regression analyses were conducted by considering remission at 1 year (DAS28-ESR < 2.6 or SDAI ≤ 3.3) as the dependent variable and 2 definitions of independent variables (either absolute values or changes from baseline in DAS28-ESR or SDAI) at Week 0 for the absolute values and weeks 4, 8, 12, 20, and 24 for both the absolute values and changes from baseline. These logistic regressions allowed calculation (and plotting) of the predictive probability of patients’ achieving remission at 1 year based on absolute DAS28-ESR/SDAI values or changes in DAS28-ESR/SDAI from baseline at earlier timepoints. The rate of remission at 1 year was also calculated for specific cutoffs of absolute values (based on accepted categories of disease activity status, i.e., DAS28-ESR < 2.6, 2.6 ≤ DAS28-ESR ≤ 3.2, 3.2 < DAS28-ESR ≤ 5.1, and DAS28-ESR > 5.1; SDAI ≤ 3.3, 3.3 < SDAI ≤ 11, 11 < SDAI ≤ 26, and SDAI > 26) and for changes from baseline [based on clinical relevance, i.e., reductions of DAS28: ≤ 0.6 (measurement error), > 0.6 to ≤ 1.2 (not clinically relevant), and > 1.2 (clinically relevant); reductions of SDAI: ≤ 50%, > 50% to ≤ 70%, > 70% to ≤ 85%, and > 85%] at the designated timepoints. Finally, the rate of remission at 1 year was determined by combining both the predefined absolute values (DAS28-ESR > 3.2 or > 5.1; SDAI > 11 or > 26) and the DAS28-ESR changes from baseline (DAS28-ESR reduction ≤ 0.6 or ≤ 1.2) or SDAI response (SDAI70 or SDAI85) at given times. Because of the differences observed between combination therapy and MTX monotherapy in the magnitude and timing of efficacy5, these analyses were conducted in each study treatment group.
RESULTS
Patient disposition and characteristics
A total of 542 patients were enrolled in the COMET study. The population of patients with at least 1 year of followup numbered 391 (ETN/MTX, n = 213; MTX, n = 178). Demographics and baseline disease characteristics of patients with DAS28-ESR data available at 1 year were generally similar in the 2 treatment groups (Table 1).
Demographics and baseline disease characteristics by treatment-group completer population in patients with DAS28-ESR or SDAI data available at 1 year.
According to this completer analysis, in the ETN/MTX therapy group, 119 of 212 patients (56%) achieved DAS28-ESR remission (DAS28-ESR < 2.6) at 1 year, compared with 64 of 176 patients (36%) in the MTX monotherapy group. SDAI remission (SDAI ≤ 3.3) was achieved by 47 of 181 patients (26%) who received combination therapy versus 19 of 145 patients (13%) who received MTX monotherapy.
Short-term predictors of remission at 1 year
Patient probability of achieving DAS28-ESR remission at 1 year based on respective absolute DAS28-ESR and the DAS28-ESR changes from baseline at weeks 4 through 24 is shown for both treatment groups in Figures 1–4. Persistent high disease activity indicated by high absolute DAS28-ESR values decreased the probability of achieving remission at 1 year while patients continued the same treatment regimen, regardless of study treatment. In patients receiving combination therapy who had high disease activity (i.e., DAS28-ESR > 5.1) at baseline, the proportion of patients achieving DAS28-ESR remission after 1 year of therapy was 54.7% (n/N = 105/192); with the persistence of such high disease activity after 8 and 12 weeks of therapy, respectively, the proportion of patients achieving remission decreased to 27.3% (n/N = 9/33) and 25.0% (n/N = 6/24). In patients receiving MTX monotherapy who had high disease activity, the corresponding decreases were from 34.8% (n/N = 56/161) at baseline to 27.0% (n/N = 20/74) and 7.5% (n/N = 4/53) after 8 and 12 weeks of treatment, respectively. Similar results were observed in the analysis using SDAI as outcome measure (Appendices 1–4).
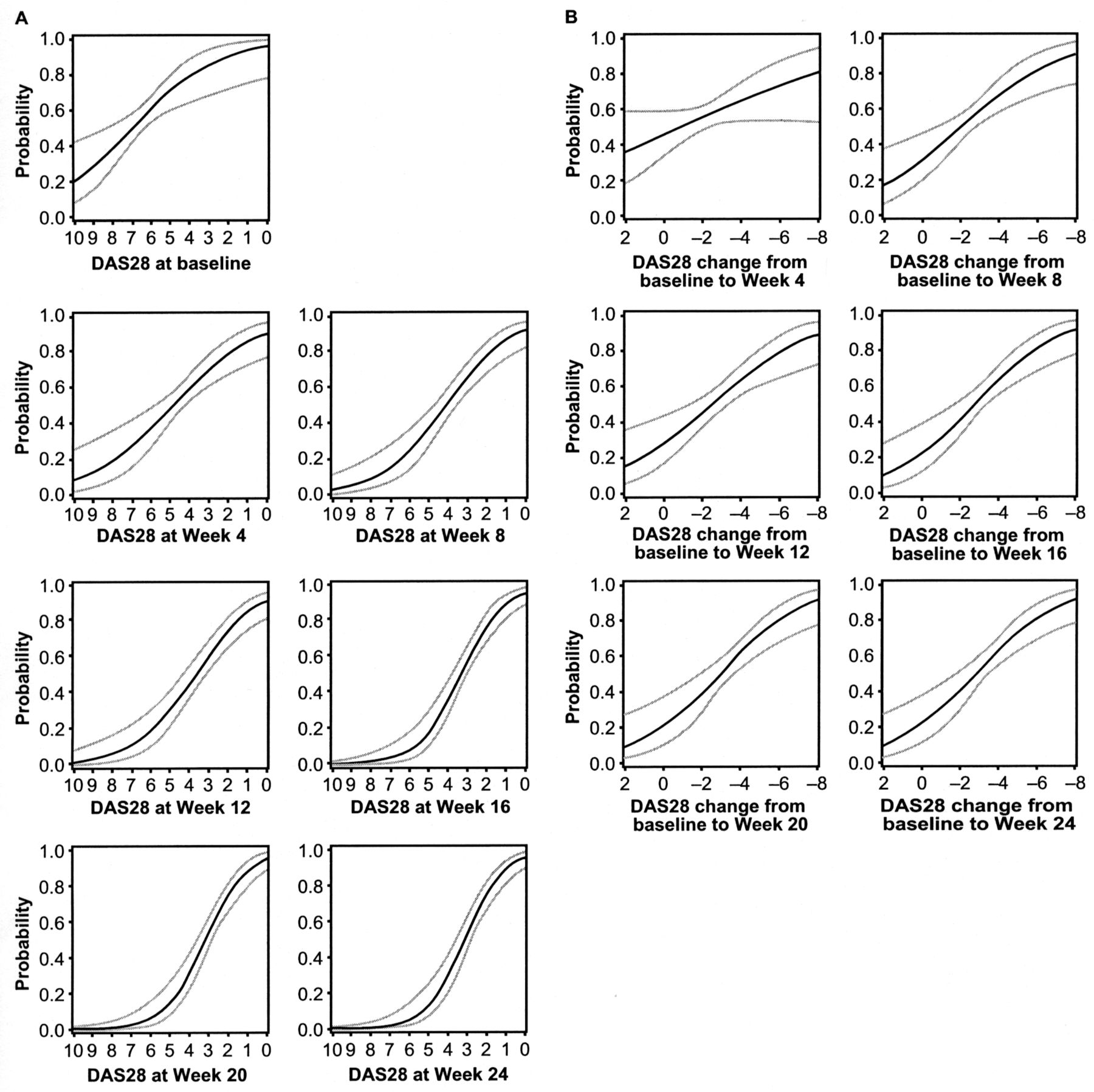
Predictive probability of DAS28-ESR remission at 1 year (solid black) and 95% CI (grey) by (A) absolute DAS28-ESR scores and (B) changes in DAS28-ESR scores among patients treated with combination etanercept/methotrexate. DAS remission was defined as DAS28-ESR < 2.6. DAS28-ESR: 28-joint Disease Activity Score calculated by erythrocyte sedimentation rate.
Non-clinically relevant changes from baseline were also associated with a reduction in the rate of remission at 1 year in both study treatment groups. In patients receiving combination treatment who had a reduction from baseline in DAS28-ESR ≤ 0.6, the rate of remission decreased from 32.1% (n/N = 9/28), 38.5% (n/N = 5/13), and 33.3% (n/N = 2/6) at weeks 4, 8, and 12, respectively, to 14.3% (n/N = 1/7) at Week 16. In patients treated with MTX monotherapy, the corresponding decreases were from 37.0% (n/N = 27/73), 25.0% (n/N = 10/40), and 19.2% (n/N = 5/26) at weeks 4, 8, and 12 to 11.8% (n/N = 2/17) at Week 16.
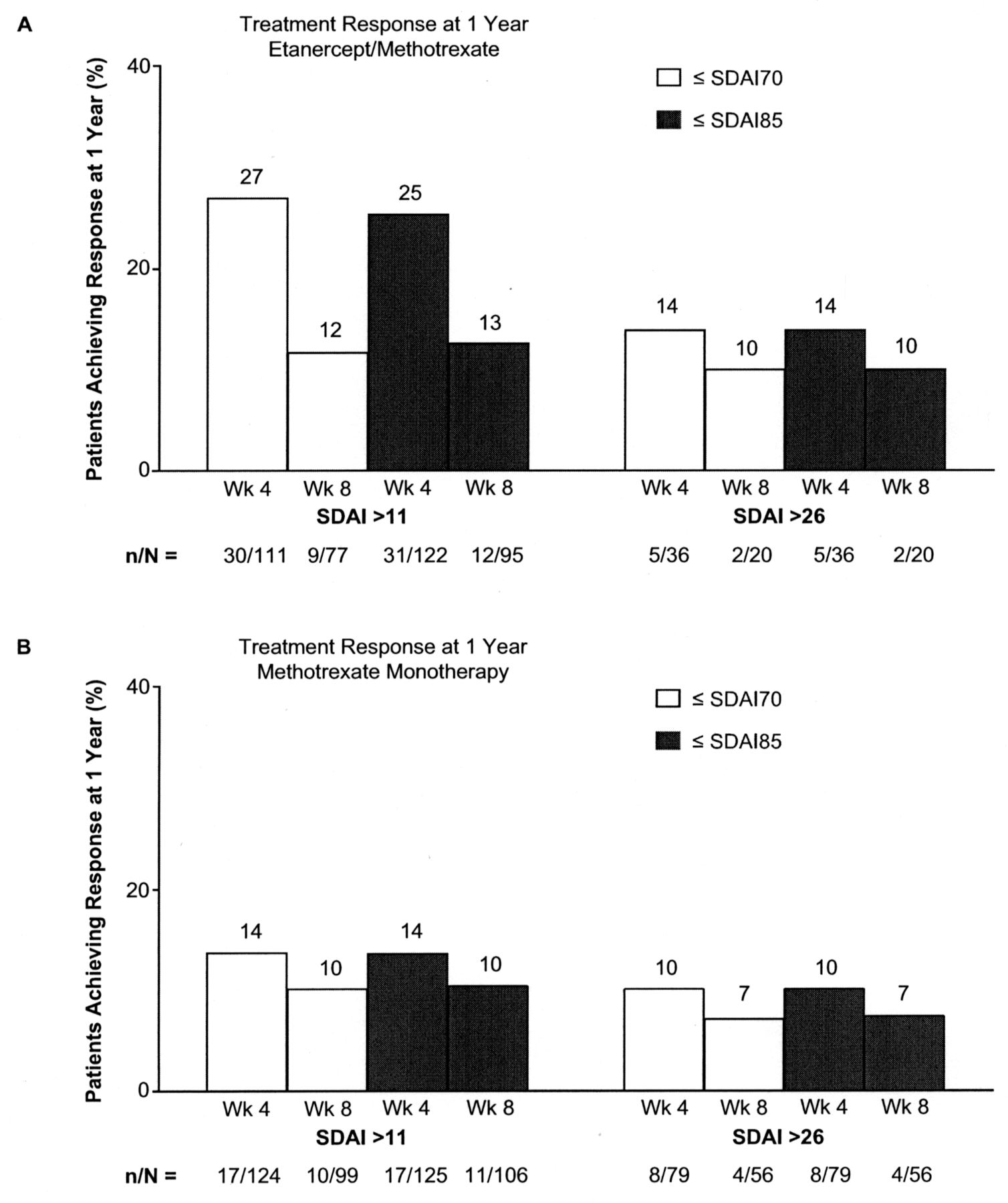
The rate of remission at 1 year was greater with ETN/MTX therapy than with MTX monotherapy regardless of disease activity level at most timepoints (Figures 3 and 4). Small numbers of patients in both treatment groups had active disease and non-clinically relevant changes in DAS28-ESR or SDAI at 4 and 8 weeks, particularly those administered ETN/MTX (Figure 5; Appendix 5). However, these analyses indicate that a substantial proportion of patients who did not achieve low disease activity or clinically relevant improvement from baseline did achieve remission at 1 year.

Predictive probability of DAS28-ESR remission at 1 year (dashed black) and 95% CI (grey) by (A) absolute DAS28-ESR scores and (B) changes in DAS28-ESR scores among patients treated with methotrexate alone. DAS remission was defined as DAS28-ESR < 2.6. DAS28-ESR: 28-joint Disease Activity Score calculated by erythrocyte sedimentation rate.

DAS28-ESR remission (DAS28-ESR < 2.6) at 1 year among patients treated with ETN/methotrexate (n = 213), by short-term clinical outcomes. n = no. patients in this clinical situation at this time of the study who achieved DAS28-ESR remission after 1 year of this treatment regimen; N = number of patients in this clinical situation at this time of the study. Total N varies between timepoints because of the omission of patients with missing data required for calculation of the DAS28-ESR score. DAS28-ESR: 28-joint Disease Activity Score calculated by erythrocyte sedimentation rate; ETN: etanercept.

DAS28-ESR remission (DAS28-ESR < 2.6) at 1 year among patients treated with methotrexate monotherapy (n = 178), by short-term clinical outcomes. n = no. patients in this clinical situation at this time of the study who achieved DAS28-ESR remission after 1 year of this treatment regimen; N = no. patients in this clinical situation at this time of the study. Total N varies between timepoints because of the omission of patients with missing data required for calculation of the DAS28-ESR score. DAS28-ESR: 28-joint Disease Activity Score calculated by erythrocyte sedimentation rate.

Percentages of patients achieving DAS28-ESR treatment response (DAS28-ESR < 2.6) at 1 year, by short-term clinical outcomes. Each percentage corresponds to the rate of remission at 1 year with regard to both the absolute DAS28-ESR value (> 3.2 or > 5.1) and the change from baseline (reduction ≤ 0.6 or ≤ 1.2) at a given study timepoint (weeks 4 and 8). DAS28-ESR: 28-joint Disease Activity Score calculated by erythrocyte sedimentation rate.
DISCUSSION
Findings of these posthoc analyses may help answer this critical question: When should clinicians consider an adjustment in biologic and/or DMARD regimens after treatment initiation in patients with RA? The results suggest that the level of disease activity and treatment response during the first 6 months of treatment are predictive of a poor clinical response at 1 year with both combination ETN/MTX therapy and MTX monotherapy. Non-clinically relevant changes from baseline over the initial 3 to 4 months of treatment were associated with a reduced likelihood of later remission. Among patients treated with combination ETN/MTX, weeks 16 to 24 were critical for the assessment of disease activity state and response, with < 10% of patients with high disease activity at 16 weeks achieving DAS28-ESR remission at 1 year. However, the small numbers of patients with high DAS28-ESR levels (i.e., > 5.1) from weeks 16 to 24 should be considered when analyzing these findings. The critical timepoint for assessment appeared to occur earlier in patients treated with MTX monotherapy because a similarly small proportion of patients with DAS28-ESR > 5.1 at Week 12 achieved the treatment target at Year 1. Although treatment response after 4 weeks of MTX monotherapy was not predictive of remission at 1 year, responses after 8 to 12 weeks were strongly predictive. The latter findings are supported by larger numbers of MTX-treated patients in subgroups with high disease activity at these timepoints. The present findings suggest that if high disease activity persists after 2 to 3 months of MTX therapy or 4 to 6 months of ETN/MTX therapy in patients with early active RA, alternative treatments should be considered. The observations from these analyses that patients with persistent disease activity and inadequate therapeutic response early in the treatment course (e.g., at weeks 12 to 16) are more likely to have poor longterm clinical outcomes are consistent with those from previously published reports8,9,10,11,12. Moreover, the optimal window for assessment suggested by these data coincides with current EULAR RA treatment guidelines, which propose that clinicians consider modification of treatment regimens after 3 to 6 months if treatment targets are not achieved4.
Several features of these posthoc analyses differentiate them from previous research. In our analyses, because the COMET population comprised patients with early RA, remission was selected as the treatment target. At a later stage of the disease, as recommended by EULAR and the T2T (Treat to Target) Expert Committee (Smolen, et al) guidelines3,4, a status of low disease activity would be acceptable. Remission was defined as DAS28-ESR < 2.6 because the DAS28 is the most commonly used assessment tool and was used to validate interest in a treat-to-target approach3. Nevertheless, some scientific arguments suggest that other tools, such as the SDAI, are more accurate. For this reason, a sensitivity analysis was conducted using the SDAI as the outcome measure. The findings of the analyses using the DAS28-ESR and SDAI approaches were similar. In addition to definition of the treatment target itself (i.e., DAS28-ESR < 2.6), the time to achieve that target, specified as 1 year after treatment initiation, was determined. Finally, clinical cutoffs were also selected that would identify unacceptable outcomes in terms of disease activity state and treatment response to help prevent continuation of potentially non-beneficial/deleterious and costly treatments.
These analyses have both strengths and weaknesses. The COMET study design, which required fixed treatment during Year 1, allowed for evaluation of the predictive probability of 1-year remission based on a given status of clinical activity at a given timepoint in patients receiving the same treatment regimen for the entire year. However, this design does not reflect current clinical practice because, for example, patients with very active disease at baseline who were randomized to receive MTX monotherapy would likely have received a short course of corticosteroid therapy in a “real-world” setting. Similarly, after 8 to 12 weeks of therapy, practicing rheumatologists would likely consider administering an intraarticular injection of corticosteroid in patients who may have started to improve but have persistent monoarthritis or oligoarthritis. Moreover, the MTX regimen used in the COMET study (i.e., a starting dose of 7.5 mg QW with titration up to a maximum of 20 mg QW over 8 weeks) does not reflect current practice, in which MTX is administered in a higher initial dose and is more rapidly escalated to the maximum dose. The relatively small numbers of patients included in the subsets analyzed are also considered a study limitation.
The most challenging decision related to these analyses is defining the threshold for probability of remission that would warrant an adjustment to or substitution of treatment. Such a definition clearly depends on several factors, including the disease duration (e.g., early vs late), the patient’s treatment history (e.g., biologic-naive vs refractory), and possible comorbidities. Nevertheless, the information provided by these posthoc analyses will likely facilitate the clinical decision. Additional studies conducted in patient populations receiving different treatment are required to improve clinician knowledge.
Acknowledgment
We thank all patients who participated in the COMET study as well as all investigators and medical staff at all of the participating centers.
APPENDIX 1.
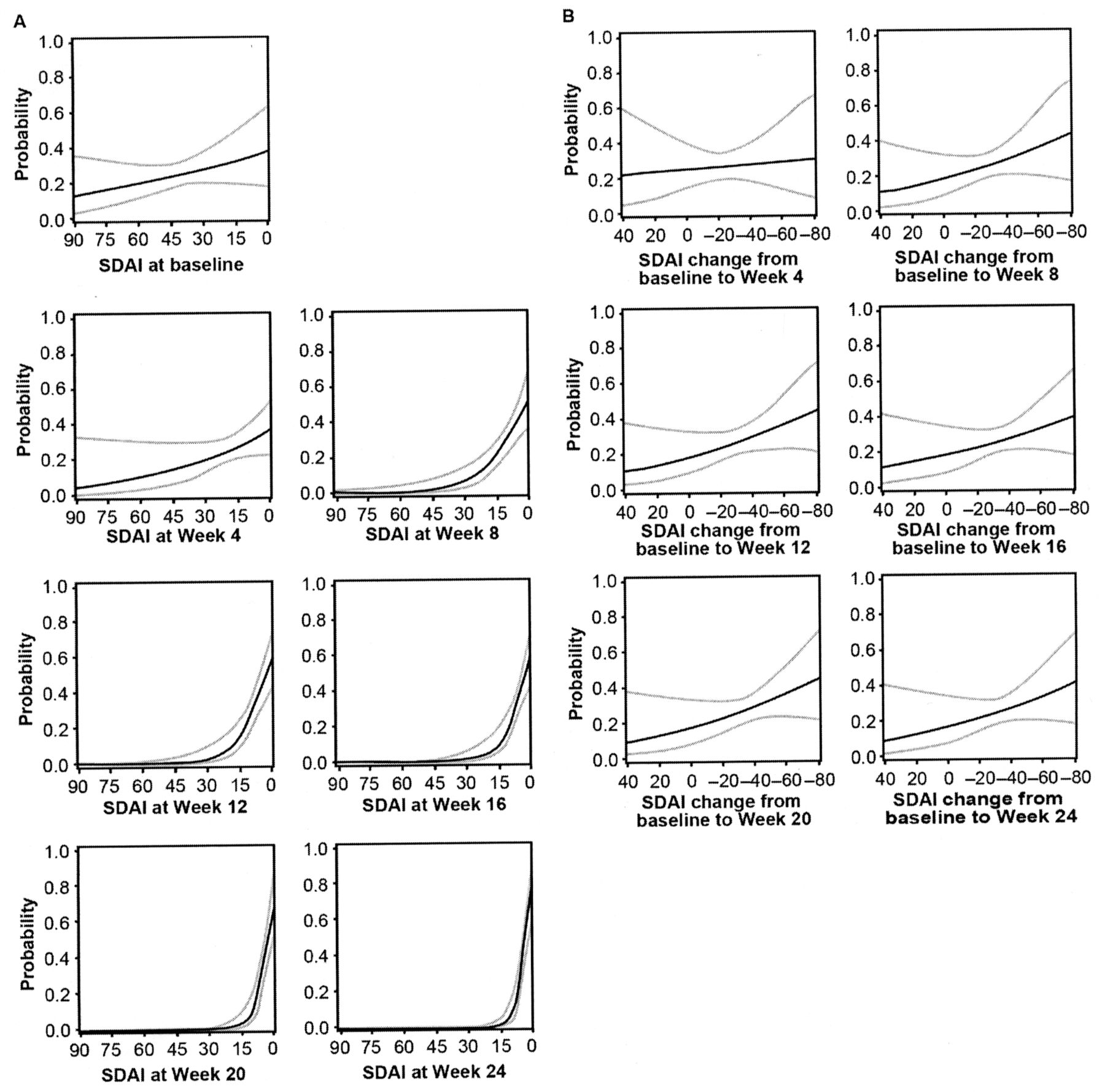
Predictive probability of SDAI remission at 1 year (solid black) and 95% CI (grey) by absolute SDAI scores (A) and changes in SDAI scores (B) among patients treated with etanercept/methotrexate. SDAI remission was defined as SDAI ≤ 3.3. SDAI: Simplified Disease Activity Index.
APPENDIX 2.

Predictive probability of SDAI remission at 1 year (dashed black) and 95% CI (grey) by (A) absolute SDAI scores and (B) changes in SDAI scores, among patients treated with methotrexate monotherapy. SDAI remission was defined as SDAI ≤ 3.3. SDAI: Simplified Disease Activity Index.
APPENDIX 3.

SDAI remission (SDAI ≤ 3.3) at 1 year among patients treated with etanercept/methotrexate (n = 213), by short-term clinical outcomes. n = no. patients in this clinical situation at this time of the study who achieved SDAI remission (SDAI ≤ 3.3) after 1 year of this treatment regimen; N = number of patients in this clinical situation at this time of the study. Total N varies between timepoints because of the omission of patients with missing data required for calculation of the SDAI score. SDAI: Simplified Disease Activity Index.
APPENDIX 4.
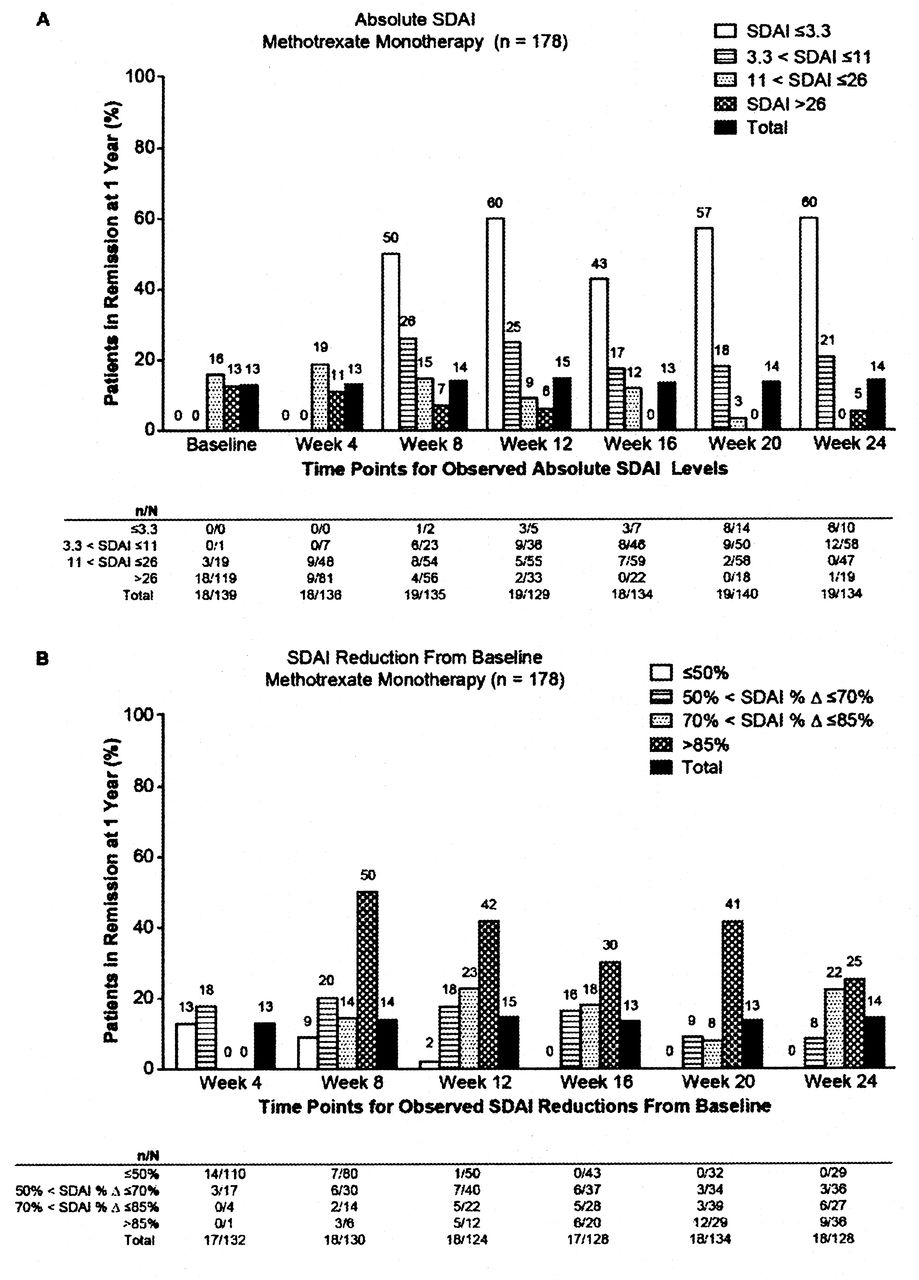
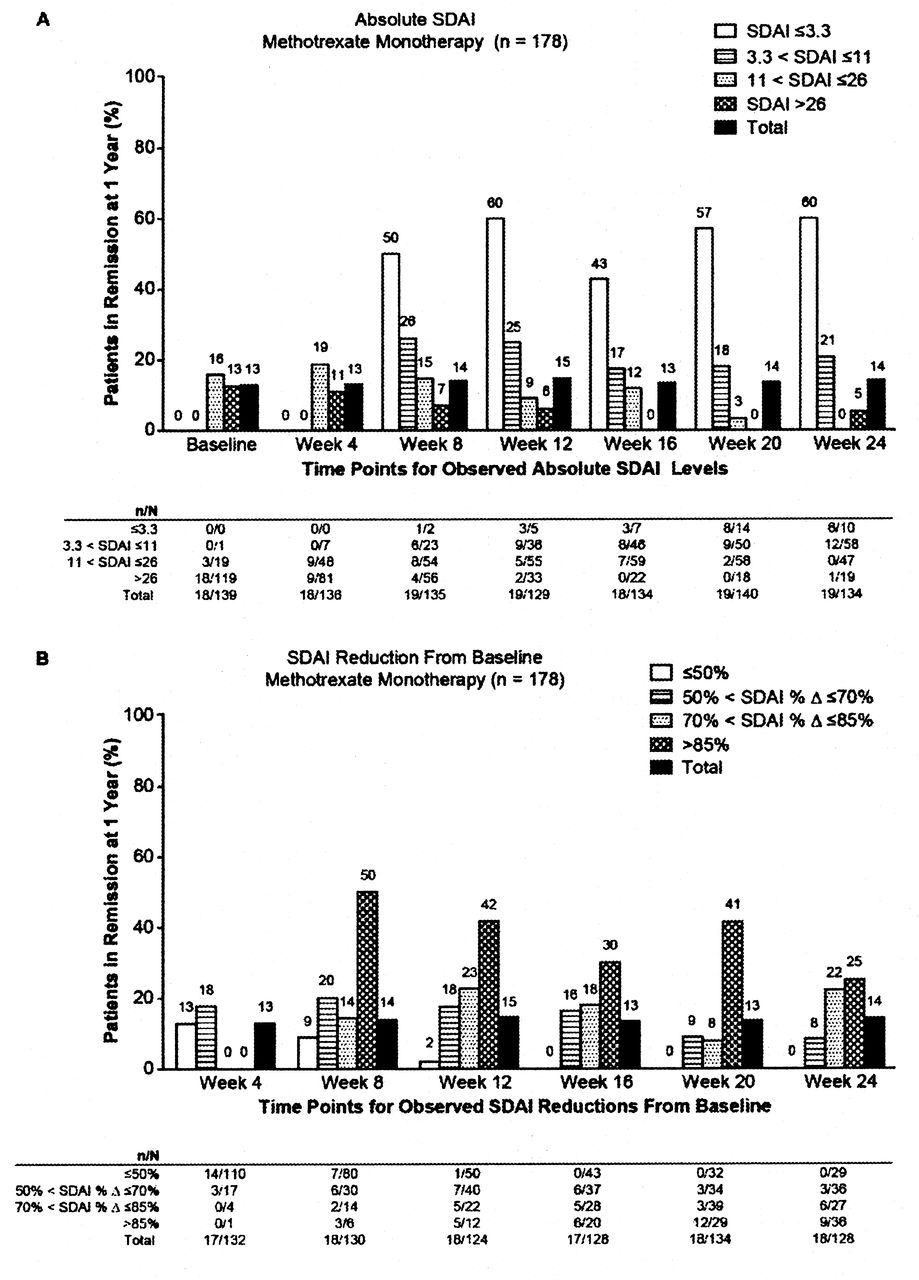
SDAI remission (SDAI ≤ 3.3) at 1 year among patients treated with methotrexate monotherapy (n = 178), by short-term clinical outcomes. n = no. patients in this clinical situation at this time of the study who achieved SDAI remission (SDAI ≤ 3.3) after 1 year of this treatment regimen; N = no. patients in this clinical situation at this time of the study. Total N varies between timepoints because of the omission of patients with missing data required for calculation of the SDAI score. SDAI: Simplified Disease Activity Index.
APPENDIX 5.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
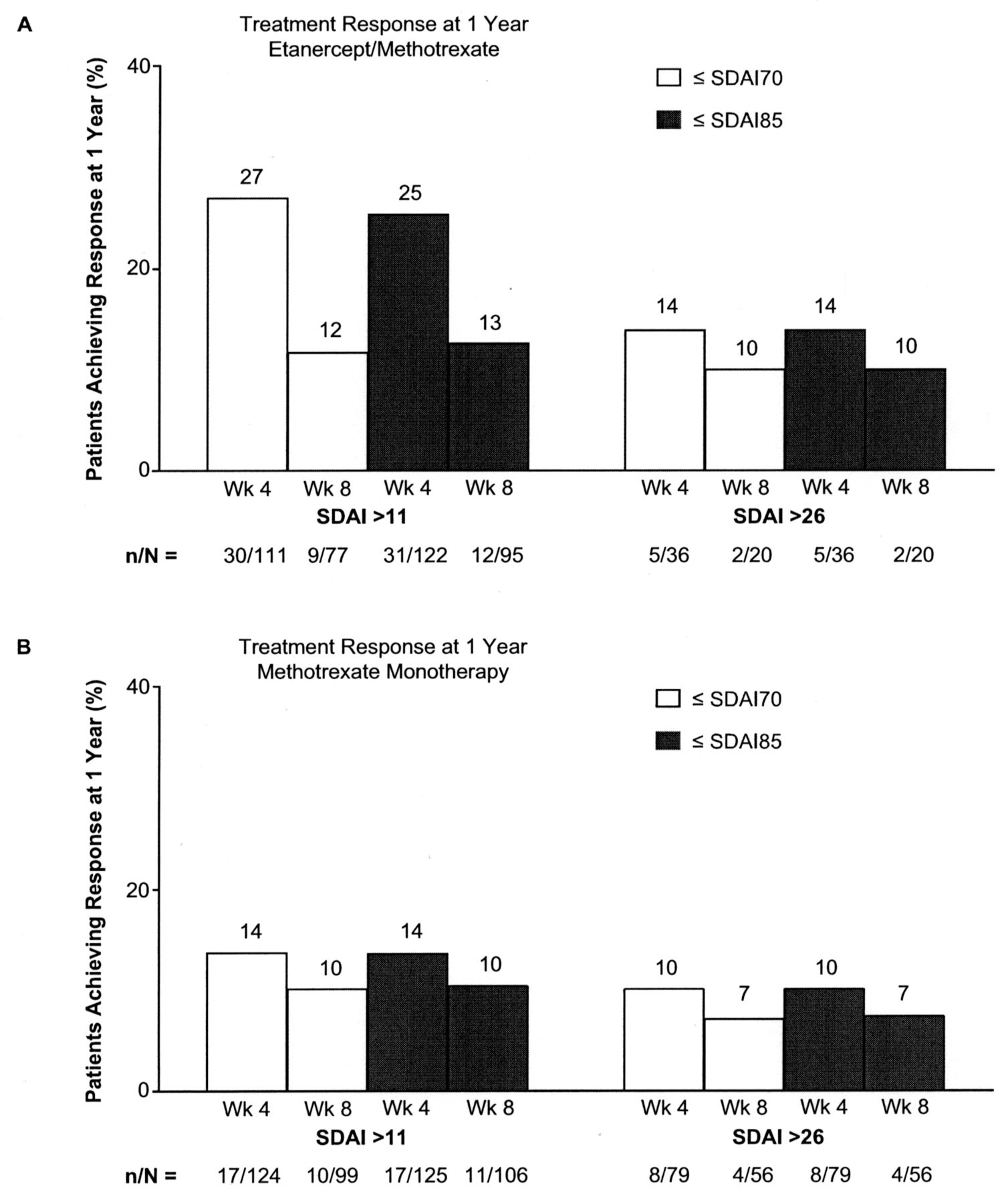
Percentages of patients achieving SDAI treatment response (SDAI ≤ 3.3) at 1 year, by short-term clinical outcomes. Each percentage corresponds to the rate of remission at 1 year with regard to both the absolute SDAI value (> 11 or > 26) and the percent change from baseline (≤ 70% or ≤ 85%) at a given study timepoint (weeks 4 and 8). SDAI: Simplified Disease Activity Index.
Footnotes
-
The COMET study was sponsored by Wyeth Research, which was acquired by Pfizer Inc. in October 2009. Editorial/medical writing support was provided by Donna McGuire of Engage Scientific Solutions and was funded by Pfizer Inc. M.R. Dougados has participated in advisory boards and symposia organized by Pfizer, Abbott, UCB, Roche, and Bristol-Myers Squibb; his department has received research grants from Pfizer, Abbott, UCB, Roche, Bristol-Myers Squibb, Sanofi, Lilly, and Novartis. D.M. van der Heijde has received consulting fees and/or research grants from AbbVie, Amgen, AstraZeneca, Bristol-Myers Squibb, Centocor, Chugai, Daiichi, Eli-Lilly, GlaxoSmithKline, Janssen Biologics, Merck, Novartis, Novo-Nordisk, Otsuka, Pfizer, Roche, Sanofi-Aventis, Schering-Plough, UCB, Vertex, and Imaging Rheumatology bv. Y. Brault, A.S. Koenig, and I.S. Logeart are Pfizer employees.
- Accepted for publication April 3, 2014.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.