
Abstract
Objective. Magnetic resonance imaging (MRI) is considered the modality of choice for the diagnosis of spondyloarthropathy (SpA)-related spondylodiscitis, or discovertebral erosions (DE). Our aim was to analyze the prevalence and the clinical features of DE in patients with enteropathic SpA (EA) using MRI.
Methods. We evaluated 72 patients with EA and 43 controls for the study. All patients and controls underwent rheumatological and gastroenterological clinical examinations, and demographic features were recorded. For each patient, these factors were also recorded: duration of inflammatory bowel disease and arthritis from onset to enrollment, history of viral and bacterial infections, and occurrence of previous major trauma to the spine. These scores were taken: Bath Ankylosing Spondylitis Metrology Index (BASMI), Bath Ankylosing Spondylitis Functional Index (BASFI), Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), Harvey-Bradshaw Index, and the Simple Clinical Colitis Activity Index. All subjects had MRI of the spine.
Results. On the basis of inclusion criteria, 43 patients with EA were included in the study. Twenty-three had axial EA (axEA) and 20 had axial and peripheral subset EA (overlap subset or peripheral type 3; axphEA). Twenty-two patients with EA (15/7 axEA/axphEA) showed DE (30.55%; p < 0.001). DE was significantly more prevalent in axEA subjects than in the overlap subset (p < 0.001). In axEA, DE had a significant direct correlation with arthritis duration (r = 0.546, p = 0.007). Patients with DE showed BASDAI, BASMI, and BASFI scores significantly higher than patients without DE (p < 0.001).
Conclusion. We found a high prevalence of DE among patients with EA (30.55%), confirming that DE is an important characteristic aspect of SpA. We found a high prevalence in patients in the axphEA subset (31.82%), suggesting that DE could be a characterizing feature of the overlap subset.
- ENTEROPATHIC SPONDYLOARTHRITIS
- DISCOVERTEBRAL EROSIONS
- MAGNETIC RESONANCE IMAGING
- INFLAMMATORY BOWEL DISEASE
- SPONDYLOARTHROPATHIES
Rheumatic manifestations are the most frequent extraintestinal findings of inflammatory bowel disease (IBD), occurring in up to 62% of patients1,2. The arthritic manifestations of IBD (enteropathic spondyloarthropathy; EA) are divided into clinical subsets of peripheral and axial joint involvement (including sacroiliitis, with or without spondylitis). Two subtypes of peripheral arthritis were classified by Orchard, et al3: type 1, the pauciarticular form, and type 2, the polyarticular form. More recently, Smale, et al proposed another form of peripheral arthritis, type 3, which includes patients with both axial and peripheral joint involvement, or the overlap subset4. Axial involvement is more common in Crohn disease (CD; 5%–22%) than in ulcerative colitis (UC; 2%–6%); the prevalence of sacroiliitis (asymptomatic and symptomatic) is 12%–20%, and of spondylitis, 2%–16%1. Recently, some studies have shown that the prevalence of axial joint involvement is higher than previously reported, as described by Scarpa, et al5. Based on the European Spondylarthropathy Study Group (ESSG) criteria for spondyloarthropathy (SpA)6, these studies show a frequency ranging between 10% and 25% for spondylitis and 30%–36% for sacroiliitis2,7,8.
A spinal complication of spondylitis in patients with IBD is the development of erosive sclerotic lesions of vertebral body adjacent to disc9 or aseptic spondylodiscitis (discovertebral erosions; DE), also called the Andersson lesion10. Diagnosis is sometimes delayed, particularly in patients with an insidious onset and nonspecific symptoms11. In ankylosing spondylitis (AS), some studies report a frequency of DE of 1.5%–28%12,13,14,15,16,17,18. In psoriatic arthritis (PsA), Scarpa described a lower frequency of 12%19, while there are no data about the prevalence of these lesions in other SpA.
The diagnosis of DE is often difficult. It is based on clinical and radiological features. Magnetic resonance imaging (MRI), a technique used to evaluate the axial involvement of SpA20,21,22, is considered the modality of choice for the radiological diagnosis of discovertebral changes, such as spondylodiscitis18,23.
In our study we used MRI to characterize destructive lesions at discovertebral junctions in patients with EA. We then defined the prevalence and the clinical features.
MATERIALS AND METHODS
Patients and design
Seventy-two patients with EA (43 men, 29 women; mean age ± SD 39.68 ± 7.65 yrs; range 20–47 yrs), consecutively admitted to the Spondyloarthropathy Research Unit of University Federico II, Naples, Italy, between December 2010 and December 2011, were evaluated for inclusion in our study. The diagnosis of UC and/or CD was made by one author (FM and/or FC) based on clinical, endoscopic, and histological evaluation24. Because at present no gold standard is available, the diagnosis of EA was made according to the ESSG criteria6. Patients with EA were classified on the basis of articular involvement into peripheral (phEA) and axial (axEA) subsets. Patients in phEA were classified as type 1 or type 2, as proposed by Orchard, et al3.
The inclusion criteria were the presence of axial involvement with back pain for at least 3 months and with an insidious onset, morning stiffness that improves with exercise, and age < 45 years. Control subjects, matched with cases for age and sex, were recruited from the hospital staff.
Both patients and controls underwent rheumatological and gastroenterological clinical examinations, and demographic features were recorded. For each patient we also recorded the following data: IBD and arthritis duration from onset to enrollment; history of tuberculosis; staphylococci, streptococci, and gram-negative bacterial infections; and major trauma to the spine.
EA clinical disease activity was assessed using the Bath Ankylosing Spondylitis Metrology Index (BASMI) for the measurement of spinal mobility25, the Bath Ankylosing Functional Index (BASFI)26, and the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI)27. Other measures taken were the Harvey-Bradshaw Index (HBI)28 and the Simple Clinical Colitis Activity Index (SCCAI)29 for CD and UC. The SCCAI includes bowel frequency during the day and night, urgency of defecation, blood in stool, general well-being, and extracolonic features. The HBI includes general well-being, abdominal pain, number of liquid stools per day, abdominal mass condition, and complications. These 2 indices were chosen because they are based entirely on symptoms and do not require any invasive procedures, yet they correlate very well with more complex indices28,29.
Venous blood samples were collected from each subject to evaluate the inflammatory markers C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR).
Informed consent was obtained from all subjects and the study protocol was approved by the ethics committee.
Imaging procedures
MRI studies were performed at 1.5 Tesla (Achieva; Philips) along sagittal planes covering the whole spine with 3 partially overlapping slabs. MRI sequence included a TSE T1 [slice thickness 3 mm, TR 650 msec, TE 9.3 msec, field of view (FOV) 319 mm, matrix 288 × 384 pixel), T2 (slice thickness 3 mm, TR 3500 msec, TE 99 msec, FOV 280 mm, matrix 288 × 384 pixel), and short-tau inversion recovery (STIR; slice thickness 3 mm, TR 4000 msec, TE 267 msec, TI 160 msec, FOV 320 mm, matrix 448 × 405 pixel) on the sagittal plane and with T2 (slice thickness 3 mm, TR 7090 msec, TE 106 msec, FOV 240 mm, matrix 272 × 320 pixel) on the axial plane centered on the intervertebral disk. Each study lasted about 35 min, including patient positioning.
Image evaluation
MRI images were evaluated independently and in random order on an electronic work station by 2 observers: a radiologist (ES) and a rheumatologist (RP) who were blinded to the status of each subject. The κ value of interreader concordance for the presence of DE was 0.97.
We developed standardized definitions of active and structural DE detected by MRI. These focused on bone marrow edema seen on STIR images: erosion (peripheral, irregular with ill-defined margin) of the discovertebral junction and marrow fat infiltration on T1SE images.
Bone marrow edema was defined as bright subchondral bone marrow signal on STIR images. Erosion was defined as a full-thickness defect of discovertebral endplate cortical bone combined with an altered bone marrow signal on T1SE images. Fat infiltration was defined as focal bright subcortical bone marrow signal on T1SE images.
We defined destructive erosion of the discovertebral junction as disc-related signal-intensity abnormalities of one or both vertebral halves of a discovertebral unit, associated with bone marrow edema and fat replacement or sclerosis. They appear hyperintense on STIR images and hypointense on T1SE images.
DE were assessed at each endplate at all 23 spinal levels from C2-C3 to L5-S1. The 2 readers used the second cervical vertebrae as primary points of reference for the assignment of spinal levels, and the fifth lumbar vertebra as the last point of reference.
We excluded the lesions that did not fulfill the DE definition: underlying fracture, malignancy, infectious spondylitis, hemangioma, and Schmorl node.
Statistical analysis
Statistical analysis was performed with the SPSS 16 system (SPSS Inc.). Continuous data were expressed as mean ± SD, and categorical variables were expressed as percentage. To compare continuous variables, we used independent sample t-test or the ANOVA analysis with the Bonferroni posthoc test. Correlation was assessed using Pearson’s linear correlation coefficients (r). To analyze categorical data, the chi-square test was performed. When the minimum expected value was < 5, Fisher’s exact test was used to evaluate differences according to different DE sites. To make predictions, a linear regression (stepwise) model was adopted, with the number of DE as the dependent variable and the following as independent variables: ESR, CRP, sex, age, IBD type (CD or UC), arthritis subset, IBD onset, arthritis onset, IBD duration, arthritis duration, BASDAI, BASFI, and BASMI.
All the results are presented as 2-tailed values with statistical significance for p values < 0.05.
RESULTS
Among the 72 patients with EA, 43 (29 men and 14 women; mean age ± SD 34.72 ± 6.88 yrs; range 21–45 yrs) fulfilled the inclusion criteria for the study. Twenty-nine were excluded: 26 were in the phEA subset and 3 were in the axEA subset but did not satisfy the inclusion criteria.
Control subjects (n = 43) matched for age and sex were enrolled from the hospital staff. Clinical and demographic characteristics of patients and controls are reported in Table 1.
Characteristics of the study population.
All 43 patients were in the axEA subset, on the basis of ESSG classification criteria6. In particular, 23 patients (53.50%) had axEA alone, and 20 (46.50%) had both axEA and phEA involvement (overlap subset; axphEA). The mean duration of IBD was 5.30 ± 2.54 years (range 1–9 yrs) and the mean duration of arthritis was 3.14 ± 1.63 years (range 1–6 yrs; Table 1).
While only 2 of the controls (4.65%) had DE, 22 patients (30.55%) with EA showed MRI changes consistent with the diagnosis (p < 0.001). Specifically, the MRI evidence of DE was found in 7 out of 20 subjects (31.82%) with the axphEA and in 15 out of 23 subjects (68.18%) with the axEA (p = 0.047). The prevalence of lesions was not significantly different between men and women [10 (45.45%) vs 12 (54.55%); p = 1.000] and between patients with CD and patients with UC [6 (27.27%) vs 16 (72.73%); p = 0.124].
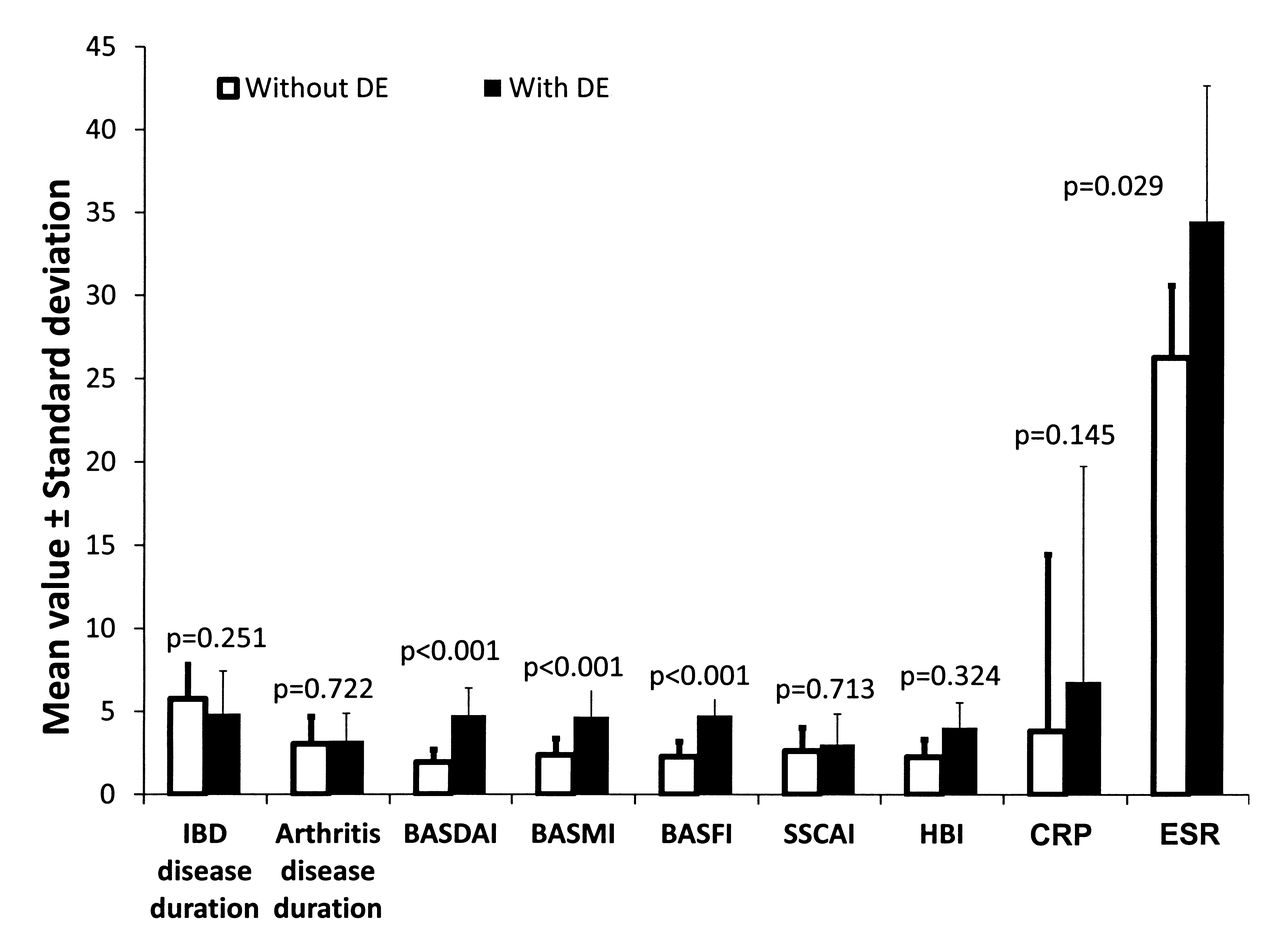
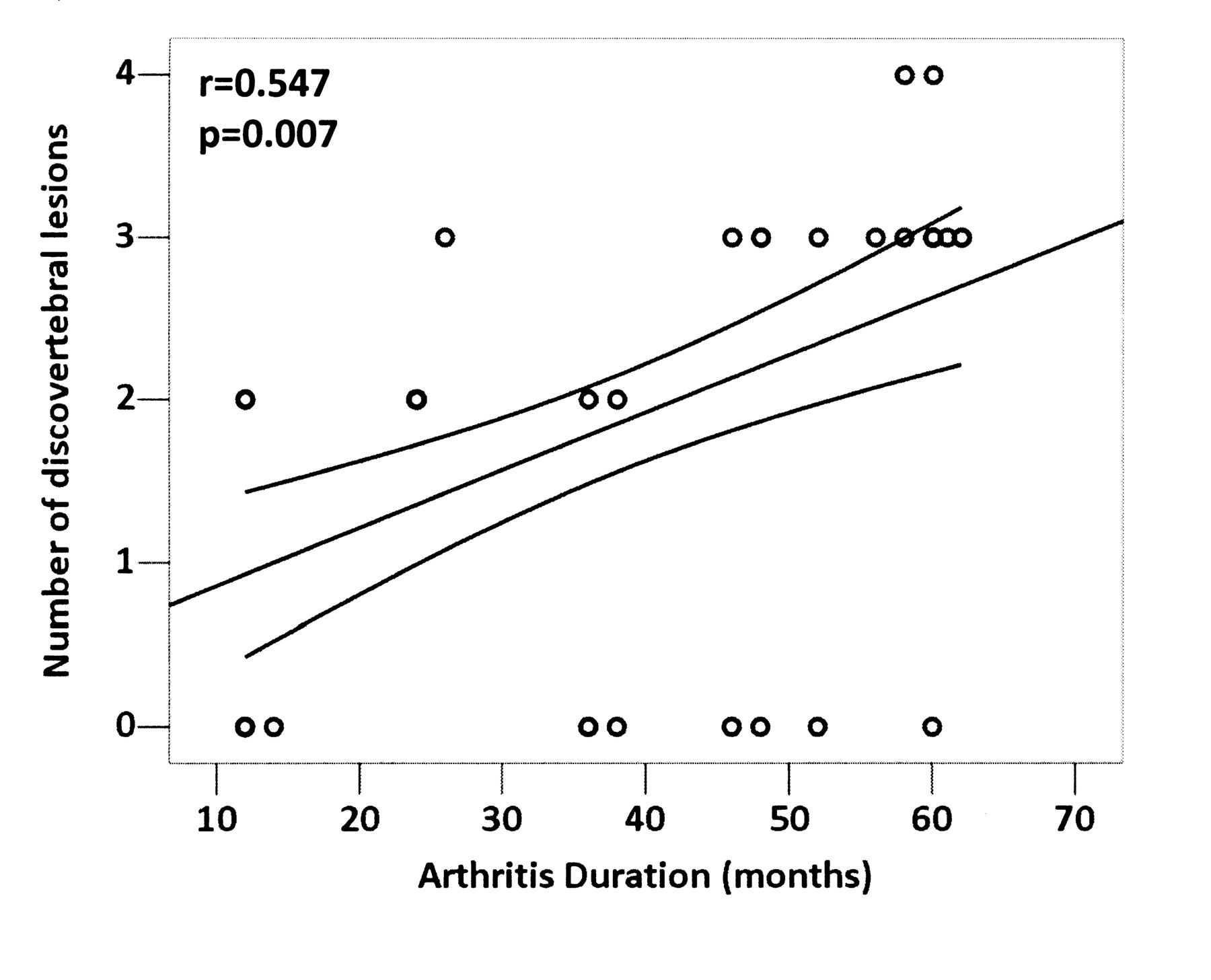
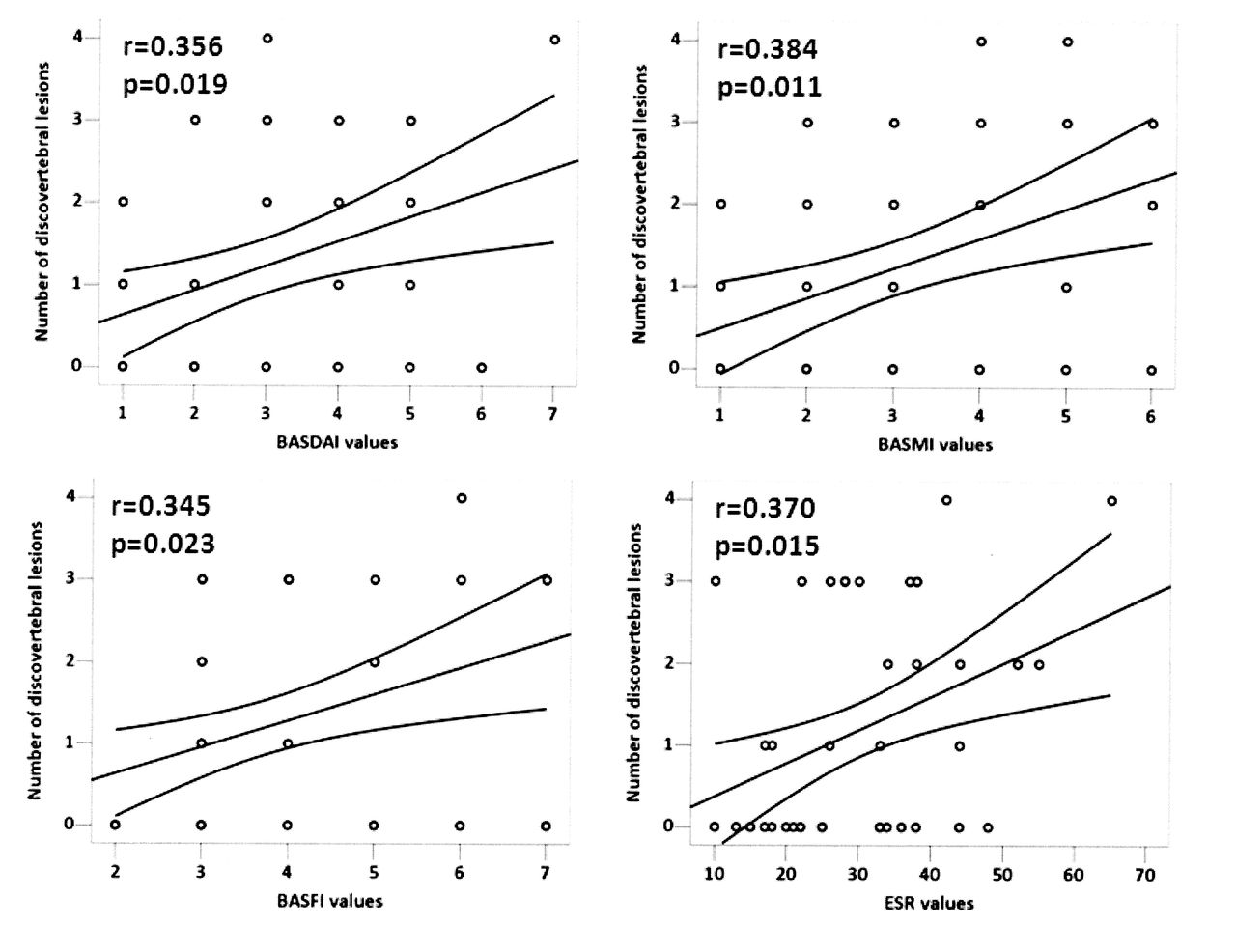
The cervical segment was affected in 3 patients (13.64%), the thoracic in 10 (45.45%), and the lumbar in 21 (95.45%). Whereas none of the patients showed an isolated lesion of the cervical and thoracic segment, 12 patients (54.55%) had a DE only in the lumbar segment. In addition, whereas none of the patients showed concomitant involvement of cervical and lumbar segments, 6 showed simultaneous lesions at thoracic and lumbar segments (27.27%; Figure 1 and 2) and 2 at cervical, thoracic, and lumbar segments (9.09%). DE were localized at one level in 12 patients (54.55%) and at multiple levels in the remaining 10 (45.45%; in 8 cases at 2 levels and in 2 cases at 3 levels). The number of lesions was significantly higher in subjects with axEA than in those with axphEA (27 vs 8; p < 0.001; Table 2). Interestingly, it was shown that the number of lesions had a significant direct correlation with arthritis duration (r = 0.546, p = 0.007) in the axEA subset (Figure 3). The axial localization was limited to the lumbar segment in 12 subjects, and involved additional areas in 10 subjects. We found that IBD and arthritis duration were significantly lower in those with isolated lumbar lesions than in those with multiple levels of involvement [3.38 ± 2.82 vs 5.71 ± 2.09, respectively (p = 0.038) and 2.13 ± 1.55 vs 3.86 ± 1.40 (p = 0.021)]. Moreover, the isolated lumbar lesions were found to be more common in subjects with axphEA than in those with axEA (p < 0.001). Further, the number of lesions was similar in patients with CD and patients with UC (p = 0.138) and was positively correlated with BASDAI (r = 0.356, p = 0.019), BASMI (r = 0.384, p = 0.011), BASFI (r = 0.345, p = 0.023), and ESR (r = 0.370, p = 0.015; Figure 4). Patients with DE showed BASDAI, BASMI, and BASFI results that were significantly higher than those of patients without these lesions [4.82 ± 1.63, 4.55 ± 1.89, 4.77 ± 1.34 vs 1.95 ± 0.74, 2.38 ± 0.97, 2.29 ± 0.90 (p < 0.001); Figure 5]. Among these, patients with axEA with lesions showed BASDAI, BASMI, and BASFI results that were significantly higher than those of axphEA patients with lesions [5.67 ± 1.05 vs 2.86 ± 0.69 (p < 0.05); 5.73 ± 1.16 vs 2.43 ± 0.79 (p < 0.05); 5.33 ± 1.18 vs 3.57 ± 0.79 (p < 0.001); Table 2]. In patients with axphEA, a direct correlation was found between number of DE and BASFI (r = 0.362, p = 0.022) and ESR (r = 0.412, p = 0.008). After adjustment for age, sex, IBD type, rheumatologic and gastrointestinal disease duration, a linear regression analysis was done; it showed that axphEA was a negative predictor of number of lesions (ß = −0.546, p < 0.001) and BASMI was a positive predictor (ß = 0.384, p = 0.011). Stratifying the population according to disease subset, arthritis duration directly predicted the number of lesions (ß = 0.431, p = 0.040) in the patients with axEA, whereas ESR was the only predictor in patients with axphEA (ß = 0.427, p = 0.036). In addition, the mean duration of arthritis in EA patients with DE was 3.14 ± 1.63 years. In detail, patients with axphEA showed a shorter duration of arthritis (1.86 ± 1.46 yrs) than patients with axEA (3.87 ± 1.36 yrs; p = 0.005).

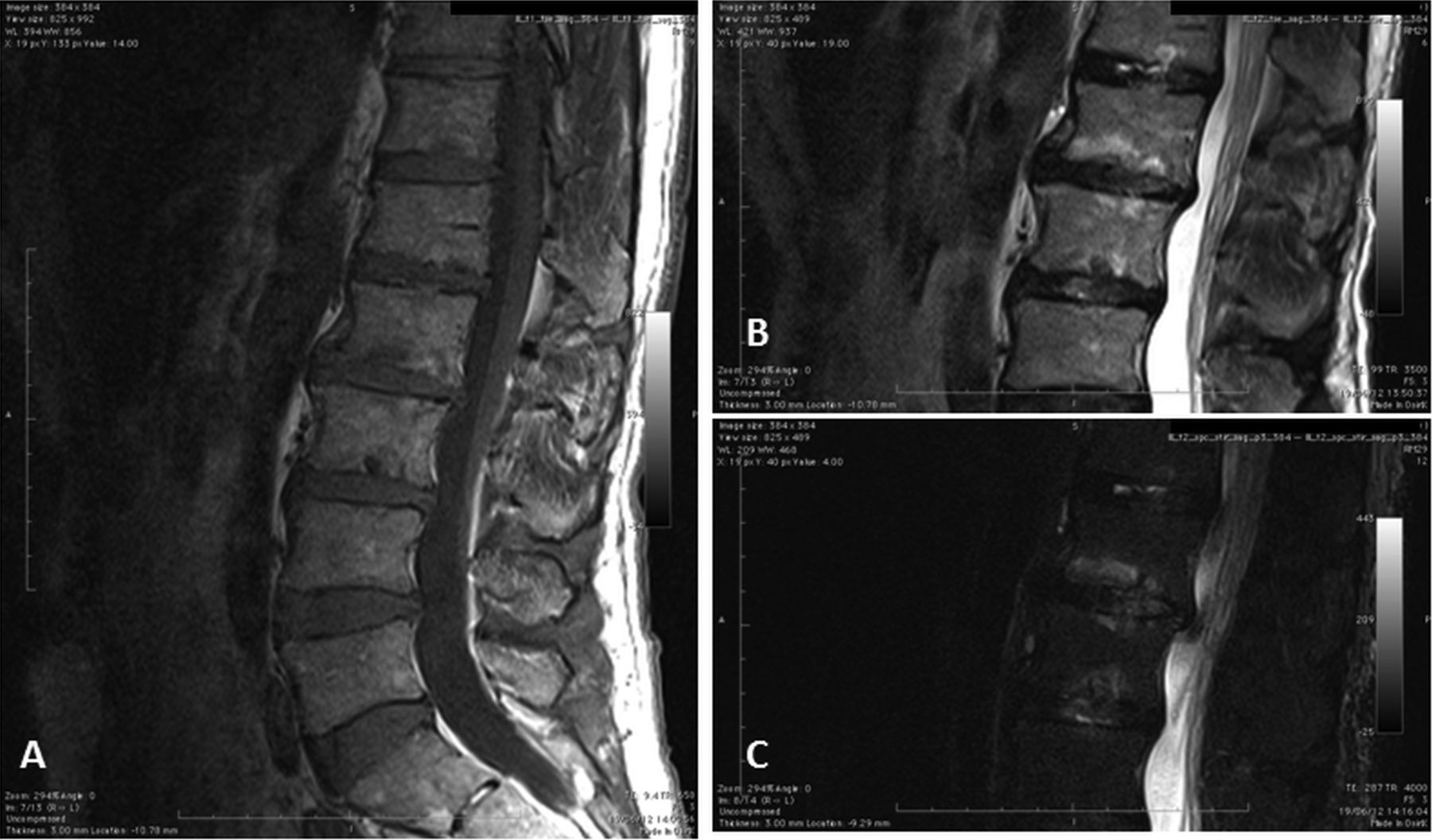
Magnetic resonance images of a 64-year-old man with enteropathic spondyloarthritis associated with Crohn disease. Sagittal sections through the thoracic spine show height reduction of intervertebral disc space, sclerosis of the endplates at D5-D6, and erosion of the inferior endplate of D5 and superior endplate of D6 (structural lesion). A. T1-weighted sequence. B and C. T2-weighted sequence. At D12 there is a Schmorl node (focal and regular small round defect with peripheral sclerotic reaction; usually localized in the center of the somatic articular profile associated with marrow edema).

Magnetic resonance images of a 64-year-old man with enteropathic spondyloarthritis associated with Crohn disease. Sagittal sections through the lumbar spine show erosion of vertebral body endplates surrounded by areas of bone marrow edema at L2-L3. A. T1-weighted sequence. B and C. T2-weighted sequence.

Pearson correlations between arthritis duration (years) and number of discovertebral erosions in subjects in the axial subset of enteropathic arthritis.

Pearson correlations between BASDAI (Bath Ankylosing Spondylitis Disease Activity Index), BASMI (Bath Ankylosing Spondylitis Metrology Index), BASFI (Bath Ankylosing Spondylitis Functional Index), erythrocyte sedimentation rate (ESR), and number of discovertebral erosions in subjects in the axial subset of enteropathic arthritis.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mean values of clinical and laboratory variables in the study population compared to the presence of discovertebral erosions (DE). P values by sample t-test. IBD: inflammatory bowel disease; BASDAI: Bath Ankylosing Spondylitis Disease Activity Index; BASMI: Bath Ankylosing Spondylitis Metrology Index; BASFI: Bath Ankylosing Spondylitis Functional Index; SSCAI: Simple Clinical Colitis Activity Index; HBI: Harvey-Bradshaw Index; CRP: C-reactive protein; ESR: erythrocyte sedimentation rate.
Clinical, functional, and laboratory data of the enteropathic arthritis patients with discovertebral erosion (DE). Data are mean ± SD unless otherwise indicated.
Age at enrollment and at IBD and arthritis onset, duration of IBD, and IBD activity (SCCAI and HBI) were similar regardless of DE status (p > 0.05).
DISCUSSION
DE is a well-known manifestation of AS. It was first described by Andersson in 1937 as a destruction and sclerosis of the disc bone border in the lumbar and thoracic spine10. Kabasakal, et al reported a DE occurrence of 8% in patients with early-onset AS; it was found in patients with a long disease duration and was mainly considered a late complication of AS15. Langlois, et al described DE in 18% of patients with severe AS, with a predominant involvement of thoracic and lumbar segments17. More recently, de Vries, et al, using MRI, recorded a low prevalence of DE in patients with severe AS with a relatively short disease duration and young age30. Scarpa reported a prevalence of 12% in PsA subjects with a longer disease duration19. In that study, moreover, the lesions were found not only in PsA patients in the axial disease subset but also in those in the polyarthritis subset (without spinal involvement), suggesting that DE are also a characteristic aspect of PsA19. In patients with IBD, these lesions occur in a range between 3% and 6%, as reported by Urlep, et al, even if the literature lacks studies with a larger number of patients31.
In the other SpA, DE are not uncommon and are often asymptomatic11, so the diagnosis is sometimes delayed.
In our study we used MRI (a sensitive method to detect DE17) to evaluate the prevalence and the clinical features of these lesions in patients with EA. MRI is considered the modality of choice for the radiological diagnosis of discovertebral changes, such as spondylodiscitis18,23. Hermann, et al compared MRI and conventional radiography of spinal changes in patients with SpA22. They concluded that the best way to detect syndesmophytes was radiography; ankylosis was detected equally well by both radiography and MRI, but for all other lesions, MRI was the preferred method. A limitation of radiography of the spine is the difficult analysis of vertebrae of the thoracic segment because of the overimposed lung tissue32, while most disorders of the discovertebral junction occur in the lower part of the thoracic and upper parts of the lumbar spine33,34.
MRI is important for early detection of discovertebral lesions. In a study using MRI in patients with AS, de Vries, et al recorded features of severe degenerative disc disease at lumbosacral segments30. The MRI features of these degenerative abnormalities were sometimes difficult to distinguish from DE, as described by Jevtic, who showed that the appearance of DE can resemble Modic type III degenerative lesion35. One difference between DE and degenerative disc disease is that DE occurs as a result of inflammation in combination with the mechanical stress of the ankylosed spine. Another difference is the location, because most DE occur at the level of the cervical, thoracic, and lumbar segments, whereas the degenerative disc disease predominates at the lumbosacral level18. The debate about the prevalence of DE is hampered by the lack of uniformity in the nomenclature of these lesions. For example, the term DE has been used for severe destructive discovertebral lesions, but also for minor abnormalities such as degenerative changes and local inflammation around the discovertebral junction18,36.
The prevalence of DE in our population was 30.55%, a high frequency compared with that of other SpA. This high prevalence confirms that DE is an important aspect of axial involvement in SpA and may be due to the persistent inflammation in the gut of patients with IBD, possibly by causing an increased antigenic load across the inflamed gut mucosa.
The DE may start as enthesitis at the insertion of the outer fibers of the annulus fibrosus, which are attached to the vertebral body adjacent to the anterior and/or lateral parts of the vertebral rim. “Romanus lesions” are marginal erosions of the anterior vertebral corners related to inflammation of the annulus fibrosus, and appear as small lesions rapidly enclosed by a rim of sclerosis. They can be viewed as mild forms of spondylodiscitis17. In our study the “Romanus lesions” were found in all patients with axEA alone and in 4 patients with axphEA (57.14%). In contrast, erosions of the posterior vertebral corners (posterior spondylitic lesions) were found in only 13.33% of patients in the axial disease subset.
While many studies reported that the presence of DE is associated with longstanding disease in AS15 and PsA19, in our study the mean duration of arthritis was only 3.14 ± 1.63 years. These results suggest that such lesions may occur earlier in the EA than in other SpA; then, DE could be considered an early manifestation of axial involvement of EA11. In addition, among patients with EA, those in the overlap subset (axphEA) showed a shorter duration of arthritis (1.86 ± 1.46 yrs) than patients with axial involvement alone (axEA; 3.87 ± 1.36 yrs; p < 0.05), suggesting that DE could be an early feature of axial involvement in patients who develop the overlap subset. In addition, even if the number of lesions showed a significant direct correlation with disease duration and activity in axEA, we found that disease duration was significantly shorter in patients with isolated lumbar lesion than in those with multiple levels of involvement. This finding suggests that lumbar lesion was the first level of involvement in those patients. Isolated lumbar lesion was found to be more common in subjects with axphEA (85.71%) than in those with axEA. Subsequently, with increasing disease duration and persistence of the inflammatory process, lesions can also extend to the thoracic and cervical segments. Indeed, in contrast with studies that showed AS as a predominant involvement of thoracolumbar levels17, in our patients we also found involvement of the cervical segment (18.18%). Scarpa showed this for patients with PsA19, always in association with thoracic and/or lumbar segments.
Patients with DE showed a higher disease activity and a worse functional status of the spine than did patients without lesions. The axEA patients with these lesions showed BASDAI, BASMI, and BASFI scores that were significantly higher than those in patients in the overlap subset with lesions, confirming that in these patients the occurrence of DE seems paucisymptomatic.
The occurrence of DE in patients with EA is probably underestimated because of the use of simple diagnostic imaging (conventional radiography), which often is not sufficient for an exact diagnosis of these lesions. Moreover, the symptoms are often mild and nonspecific, with an insidious onset that delays the timing of diagnosis. The occurrence of DE in axphEA patients with low axial disease activity and with recent onset of articular disease could be an early feature of axial involvement in patients with phEA, who are likely to develop an overlap with axial subset involvement.
- Accepted for publication August 31, 2012.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.