
To the Editor:
Rituximab (RTX) is a chimeric B cell-depleting monoclonal antibody used in the treatment of non-Hodgkin’s lymphoma and rheumatoid arthritis (RA), and with an emerging role in connective tissue disease therapy. Its use has rarely been associated with skin reactions, in particular psoriasiform skin lesions. We report a case of atypical psoriasis reactivation in a patient with RA following RTX, and we review the literature.
A 49-year-old woman presented in 1999 with a seronegative polyarthritis affecting the hands, elbows, feet, hips, and knees. At the time she gave no history of psoriasis. Over the next 10 years she received several disease-modifying antirheumatic drugs (DMARD) sequentially and in combination including sulfasalazine, hydroxychloroquine, methotrexate, azathioprine, gold, and leflunomide. Disease activity persisted, although radiographs remained nonerosive. Her 28-joint Disease Activity Score (DAS28) in September 2010 was 6.45 despite triple DMARD therapy, and she was assessed for a biologic. RTX was chosen in preference to anti-tumor necrosis factor (TNF) treatment because of recurrent shingles and a previous positive Heaf test (chest radiograph normal, quantiferon test negative).
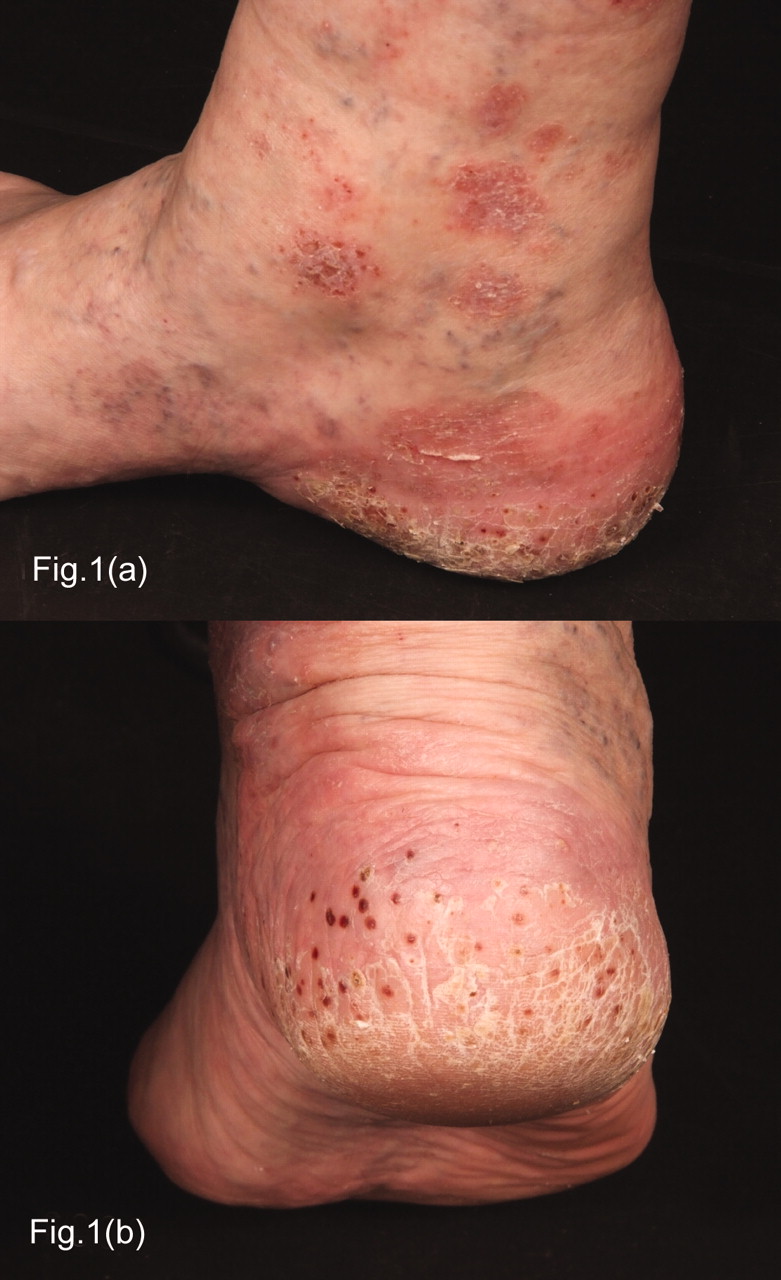
In November 2010 she received 2 intravenous infusions of 1 g RTX 2 weeks apart with paracetamol, chlorpheniramine, and methylprednisolone premedications. Ten weeks posttreatment her DAS28 score was 4.32, but she had developed skin lesions (present for 6 weeks) on the sole of her right foot plus some nail changes suggestive of psoriasis. Two months later, further red, itchy, scaly patches around the ankles and heels were seen, including some well-defined plaques (Figure 1). She was given methylprednisolone acetate intramuscular injection 120 mg and assessed by a dermatologist (SG) who confirmed the clinical diagnosis of acral psoriasis. Onset of the rash 1 month post-RTX treatment suggested causation. Topical treatments containing steroid, salicylic acid, and coal tar proved effective, with improvement over several weeks. On reviewing the notes it was established that she had had a single episode of guttate psoriasis in her teens; however, she had never developed extraarticular manifestations suggestive of psoriatic arthropathy; her pattern of joint disease (predominantly metacarpophalangeal, proximal interphalangeal joints, and knees) was more in keeping with RA. The patient’s brother has psoriasis.

{kind=link}
A. Right medial ankle showing well-defined patches of scaly erythema, in keeping with psoriasis. B. Right heel with erythema, scaling, and resolving pustular changes, more in keeping with plantar pustular psoriasis.
There are conflicting reports about the relationship between psoriasis and RTX therapy. In oncology, Mielke, et al reported a case of a patient with non-Hodgkin’s lymphoma treated with RTX and cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP) who developed psoriasis and arthritis within 6–8 weeks of exposure1. In the rheumatology setting, Markatseli, et al2 reported a patient with seropositive RA developing de novo psoriatic skin lesions of the arms and thighs 10 days after a second course of RTX treatment. Dass, et al3 published a case series of 3 patients with inflammatory arthritis (1 seronegative, 1 seropositive, and 1 with systemic lupus erythematosus) developing skin psoriasis following RTX treatment, but the interval between treatment and the development of the psoriatic skin lesions was longer in each case (4–6 months) than in our case. There has been 1 case of RTX used specifically to treat skin psoriasis4 because R-CHOP chemotherapy had previously improved psoriasis in the same patient: this resulted in worsening of the skin psoriasis within weeks. However, Cohen5 reported a patient with psoriatic arthritis and a history of skin psoriasis 15 years previously who received RTX for his joint disease, with no adverse skin effects.
The particularly noteworthy features of our case are the atypical distribution of the skin lesions (confined to the legs and feet, asymmetrically) and their quality, which around the ankles resembled chronic plaque psoriasis and on the soles plantar pustular psoriasis. The interval between RTX treatment and psoriasis development was relatively short (1 month). Although in our patient there was a history of psoriasis and rheumatoid factor and anticitrullinated protein antibodies were negative (raising the possibility of underlying psoriatic arthropathy), this problem has also been seen in seropositive RA and those with no prior history of psoriasis2,3. As our patient had an initial good clinical response to RTX, we do not consider this event to be an absolute contraindication to retreatment in the future.
The mechanism by which RTX may cause or worsen skin disease is unclear, as psoriasis is thought of as a T cell-mediated disease. Potential mechanisms proposed by other authors include disruption of regulatory actions of B cells on T cells2,3, increased susceptibility to infections, which may trigger plaque development2,3, and T cell reactivity against the murine component of the chimeric molecule1,2. Interestingly, there have also been several case reports of the induction of psoriasis following anti-TNF treatment6, especially infliximab7, despite the fact that anti-TNF is an established treatment for psoriatic arthritis.
Clinicians should be aware of the possible link between B cell depletion with RTX and development or worsening of psoriasis. This is a consideration when planning treatment, in the same way as with hydroxychloroquine, corticosteroids, and anti-TNF agents, which can exacerbate or unmask psoriasis in an unpredictable way. As use of biologic agents becomes more widespread in rheumatology it is likely that further such phenomena will emerge.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.