

Abstract
Objective. Ankylosing spondylitis (AS) and psoriatic arthritis (PsA) often affect the hip and/or knee. If effective, treatments might reduce risk of total hip or total knee arthroplasty (THA/TKA). We evaluated risk of THA/TKA related to use of medical therapies in AS/PsA.
Methods. We conducted a nested case-control study using 1994–2018 data from the OptumLabs Data Warehouse, which includes deidentified medical and pharmacy claims, laboratory results, and enrollment records for commercial and Medicare Advantage enrollees. Among those with AS/PsA, THA/TKA cases were matched up to 4 controls by sex, age, AS/PsA diagnosis, diagnosis year, insurance type, obesity, and prior THA/TKA. We assessed AS/PsA treatment 6 months prior to THA/TKA, including disease-modifying antirheumatic drugs (DMARDs) and tumor necrosis factor inhibitors (TNFi), alone or in combination, stratified by nonsteroidal antiinflammatory drug (NSAID) use. We evaluated the relation of treatment to risk of THA/TKA using conditional logistical regression with adjustment for confounders.
Results. Among 16,748 adults with AS, there were 444 THA/TKA cases and 1613 matched controls. Among 34,512 adults with PsA, there were 1003 cases and 3793 controls. Adjusted ORs for treatment category and THA/TKA ranged from 0.60 to 1.92; however, none were statistically significant. Results were similarly null in several sensitivity analyses.
Conclusion. Odds of THA/TKA were not reduced with any combinations of NSAIDs, DMARDs, or TNFi among persons with AS or PsA. Given current utilization patterns in this population of US adults with AS and PsA, these medical therapies did not appear to be associated with less end-stage peripheral joint damage.
- ankylosing spondylitis
- psoriatic arthritis
- total hip arthroplasty
- total knee arthroplasty
- tumor necrosis factor inhibitors
Ankylosing spondylitis (AS) and psoriatic arthritis (PsA) are subtypes of spondyloarthritis (SpA) with similar genetics and shared clinical features, including peripheral arthritis.1,2,3 While peripheral arthritis may be ameliorated by medical therapy, some patients experience ongoing inflammation and joint destruction, even on treatment. Alternatively, therapies may be initiated after irreversible damage has already taken place. Either situation may result in the need for arthroplasty.
Total hip arthroplasty (THA) and total knee arthroplasty (TKA) are the most common joint replacement procedures, and their frequency is on the rise.4,5 THA and TKA may be complicated by infection, and, if hardware loosens or wears out, may require surgical revision.4 Moreover, peripheral joint involvement in SpA portends a poorer prognosis than those with axial disease alone.2 Therefore, it is essential to optimize medical management to prevent end-stage peripheral joint arthritis and improve overall prognosis.
There is a paucity of literature surrounding the use of certain medical therapies for joint replacement surgery among adults with AS and PsA. Nonsteroidal antiinflammatory drugs (NSAIDs) and disease-modifying antirheumatic drugs (DMARDs) can reduce joint inflammation and therefore lower the risk of end-stage joint damage requiring an arthroplasty. NSAIDs may have an effect on bone metabolism and preserve bone mineral density, which is relevant to osteoarthritis (OA) pathology.6,7 Tumor necrosis factor inhibitors (TNFi) have been shown to reduce radiographic progression and improve clinical manifestations of AS and PsA.1,3,8,9,10,11 TNFi inhibiting radiographic progression indicates these medical therapies have effects on bone mineralization, and it is not known if these effects on bone extend beyond the spine.
A recent study showed that TNFi were associated with a reduced rate of THA in older adults with rheumatoid arthritis (RA) compared to those on conventional synthetic DMARDs.12 While there are no studies to date assessing the effect of medications on joint replacements in SpA, a Norwegian study found that THA rates in 1988–2010 decreased over time among individuals with AS compared to those with OA.13 Authors speculated this reduced rate was due to the introduction of TNFi medications slowing peripheral arthritis. However, in another Norwegian study, a PsA diagnosis after 1999 was not associated with lower risk of orthopedic surgery relative to diagnosis in an earlier year, suggesting no effect of TNFi uptake.14 Studies in the United Kingdom and the United States found increasing rates of THA among AS patients over time.15,16 Further, a Danish cohort study from 1996 to 2012 found that patients with PsA were still twice as likely to require a joint replacement compared to the general population, highlighting the need for better treatment to prevent end-stage joint damage.17 These discrepancies in the literature highlight the need for additional studies.
There are no published studies to date assessing the effects of NSAIDs, DMARDs, or TNFi on joint replacement risk in AS or PsA. These are important to include because NSAIDs are still first-line therapy for patients with AS, and both AS and PsA subjects are prescribed DMARDs. Evaluating these classes of medications, in addition to TNFi, is helpful because the findings could support future guidelines on medical therapies for these patients. We therefore assessed whether specific medical treatments were associated with risk of THA or TKA in AS and PsA, using one of the largest samples to date of adults in the US.
METHODS
We conducted a nested case-control study using data from the OptumLabs Data Warehouse (OLDW), which includes deidentified medical and pharmacy claims, laboratory results, and enrollment records for commercial and Medicare Advantage enrollees. The database contains longitudinal health information on enrollees and patients, representing a diverse mixture of ages, ethnicities, and geographical regions across the US. Members in the database had full insurance coverage for physician, hospital, and prescription drug services.18 A nested case-control study design was selected to maximize power, given the relatively low number of outcomes (knee and hip replacements).
Study sample. Cases were defined as subjects with AS or PsA with THA or TKA, and controls were defined as subjects with AS or PsA without such procedures. International Classification of Diseases, 9th and 10th revisions (ICD9 and ICD10) codes were used to identify adults with AS and PsA aged 18 years or older from January 1, 1994, to December 31, 2018. These codes (Supplementary Table 1, available with the online version of this article) have been validated in AS and PsA in prior studies.19,20 Subjects were required to have medical and pharmacy coverage at least 6 months prior to AS or PsA diagnosis, and were eligible for inclusion on the date of their second AS or PsA diagnosis claim. If a subject had both AS and PsA diagnoses, we categorized them by the first diagnosis listed. THA/TKAs were defined by ICD 9/10 procedure codes and current procedural terminology (CPT) codes, and the date of first THA/TKA during the study period was defined as the index date. We made the assumption that subjects were undergoing THA/TKA for end-stage joint damage due to their AS or PsA. We did not include arthroplasty revisions in this outcome. We did not exclude subjects who had had a single hip/knee replacement, to allow for THA/TKA on both left and right sides within each subject. Additional exclusion criteria were (1) history of 2 THAs or 2 TKAs prior to AS/PsA diagnosis, and (2) a diagnosis of inflammatory bowel disease any time prior to AS/PsA diagnosis. Subjects with inflammatory bowel disease were excluded because they may have different treatment patterns than AS and PsA subjects. We excluded hip and knee fractures 30 days prior to the outcome because this is the time frame that we would expect that any THA or TKA would be related to the fracture. As part of our internal validation study, we reviewed 100 random subject profiles, and all claims listed 6 months prior to study entry to 6 months after exit of the study. We obtained claim records with the codes of interest from the OLDW through SAS (SAS Institute); the data were then exported to Excel for review. We were able to confirm appropriate identification of diseases of interest (AS or PsA), exposures (NSAID, DMARD, and/or TNFi), and outcomes (THA or TKA).
Study design. The outcome of interest was THA or TKA, as defined by procedure codes. THA or TKA cases were each matched to up to 4 controls by sex, age (± 3 yrs), SpA subtype (AS/PsA), AS/PsA diagnosis year (± 1), insurance type (commercial or Medicare Advantage), obesity (defined as BMI ≥ 30 kg/m2), and any hip or knee replacement prior to study entry. Subjects were matched using risk-set sampling. Thus, subjects could be included as controls before they became a case. We assessed AS/PsA treatment in the 6-month period prior to THA or TKA. We assessed for use of DMARDs or TNFi stratified by NSAID use. This is because those taking NSAIDs in the 6 months prior to arthroplasty may have done so due to pain from end-stage joint disease rather than as a treatment for their AS or PsA (confounding by indication). Medical therapies were identified according to records of filled prescriptions. DMARDs included apremilast, auranofin, azathioprine, baricitinib, chloroquine, cyclophosphamide, cyclosporine, hydroxychloroquine (HCQ), leflunomide, methotrexate (MTX), mycophenolate mofetil, sulfasalazine (SSZ), thiomalate, and tofacitinib. While still a subject of controversy, we included apremilast and tofacitinib in this DMARD category because they are oral small molecules, and the low frequency of use did not allow us to analyze them separately. Janus kinase inhibitors and non-TNFi biologics were not included in this study, as there was an insufficient number of subjects on these medications.
Statistical analysis. We evaluated the relation of each type of treatment (DMARDs, TNFi stratified by NSAID use) to risk of THA or TKA using conditional logistical regression. The outcome of THA or TKA was binary (yes/no) and defined as the first THA/TKA code during follow-up. Arthroplasty codes excluded revisions. After matching subjects by age, sex, disease, diagnosis year, and insurance type, we then performed adjustment for potential confounders. These included age (after matching ± 3 years for more precision, as some subjects were not perfect matches) and history of chronic kidney disease, diabetes, liver disease, peptic ulcer disease, psoriasis (for subjects with PsA only), and RA. We also adjusted for a record of erythrocyte sedimentation rate (ESR) or C-reactive protein (CRP) testing having been performed within 1 year prior to AS/PsA diagnosis, as well as at least 1 rheumatology visit in the year prior to AS/PsA diagnosis (vs no visits). These variables were used as surrogates for disease activity. Among the strata of NSAID users, NSAID use alone was the referent group, and for NSAID nonusers, the absence of any medication of interest was the referent group. Controls were not excluded on the basis of comorbidities. As a way to assess for effect modification by how much risk a subject would incur with a knee/hip arthroplasty surgery, we considered variables that may deem a subject a poor candidate for joint replacement: BMI ≥ 40 kg/m2, history of joint infection, any high-risk cancer, end-stage renal disease (ESRD) requiring dialysis, and severe pulmonary disease requiring supplemental oxygen. We looked at the prevalence of these across cases and controls to identify any patterns for descriptive purposes but did not incorporate these variables into the analysis.
Sensitivity analyses. To assess the robustness of our primary results, we performed several sensitivity analyses for AS and PsA individually: models assessing age stratification (< 55 vs ≥ 55 years), THA and TKA separately, history of joint replacement prior to the study period (yes/no), 14-month exposure assessment (rather than our standard 6-month period), and ≥ 2 prescriptions during the exposure assessment (instead of 1). Last, we performed a conditional logistic regression model analysis considering each drug category as a binary variable and assessed the effect of each category after adjustment for other confounders.
Ethical approval. Since this study involved analysis of preexisting, deidentified data, it was exempt from Institutional Review Board approval.
RESULTS
Among 16,748 adults with AS meeting eligibility criteria, we identified 444 cases of THA or TKA. There were 1613 matched controls with AS for these cases. For cases, the mean age was 58.4 (SD 11.9) years, and 206 (46.4%) were female (see Table 1). Cases had an increased prevalence of peptic ulcer disease (29.1%) versus controls (24.7%). Other characteristics among AS cases and controls include the prevalence of chronic kidney disease (3.4% vs 3.8%), diabetes (20.7% vs 20.7%), liver disease (3.2% vs 4.2%), psoriasis (20.0% vs 20.6%), RA (24.5% vs 19.1%), BMI ≥ 30 kg/m2 (15.8% vs 12.3%), rheumatology visit in the year prior to diagnosis (53.8% vs 51.5%), and ESR/CRP ordered in the year prior to diagnosis (57.4% vs 57.3%). Very few subjects (< 11 cases and < 11 controls) had a joint replacement prior to entering the study. We were unable to report these numbers, as low frequencies were not permitted to be published per OptumLabs data policy.
Characteristics of cases and controls.
Among 34,512 adults with PsA meeting eligibility criteria, we identified 1003 cases with THA/TKA (Table 1). There were 3793 matched controls with PsA for these cases. For cases, the mean age was 59.7 (SD ± 9.8) years, and 592 (59.0%) were female. The remaining characteristics appeared similar across cases and controls, including chronic kidney disease (3.3% vs 3.9%), diabetes (22.7% vs 23.7%), prior joint replacement (3.3% vs 1.3%), liver disease (6.7% vs 6.0%), peptic ulcer disease (24.6% vs 23.9%), psoriasis (74.8% vs 76.4%), RA (22.7% vs 22.4%), BMI ≥ 30 kg/m2 (19.7% vs 18.9%), rheumatology visit in the year prior to diagnosis (67.1% vs 66.3%), and ESR/CRP ordered in the year prior to diagnosis (65.0% vs 65.6%).
History of joint infection, high-risk cancer, ESRD, and severe pulmonary disease occurred in 2.5% or fewer of cases and controls. These low frequencies were not permitted to be published per OptumLabs data policy; however, frequencies were similar between cases and controls for each condition.
Among those with AS, the unadjusted odds of THA/TKA was higher for those on TNFi only (OR 1.71, 95% CI 1.02–2.88) and for those on DMARD/TNFi combination therapy (OR 2.12, 95% CI 1.07–4.23; Table 2); however, once adjusted for confounders, these associations were no longer statistically significant (adjusted OR 1.58, 95% CI 0.88–2.82; and adjusted OR 1.92, 95% CI 0.91–4.08, respectively). Among subjects with PsA, those on NSAIDs and DMARDs had lower unadjusted odds of THA/TKA (OR 0.77, 95% CI 0.61–0.98), which also lost significance when adjusted for confounders (adjusted OR 0.78, 95% CI 0.61–1.00).
Primary outcome: odds of DMARD and/or TNFi use stratified by NSAID use within 6 months of THA or TKA among adults with AS or PsA.
Sensitivity analyses. No combination of medical therapies showed a significant association with THA/TKA once adjusted for confounding factors, as highlighted in Table 3 and Table 4. Table 3 includes the adjusted OR for TNFi use in these analyses. These include age < 55 vs ≥ 55, THA and TKA separately, prior joint replacement (yes/no), and 14-month exposure assessment. Table 4 shows the analysis performed with 2 or more prescriptions during the exposure assessment period. The median number of prescriptions for each drug category with IQRs are listed in Supplementary Table 3 (available with the online version of this article). Table 5 reveals each drug category as a binary variable. TNFi use among AS was associated with increased odds of THA/TKA at 1.83 (1.11–3.00). All other results were null.
Adjusted ORa of TNFi use among adults with AS or PsA stratified by NSAID use within 6 months of THA or TKA (secondary outcome).
Adjusted ORa of 2 or more prescriptions among adults with AS or PsA stratified by NSAID use within 6 months of THA or TKA (secondary outcome).
Adjusted oddsa of each drug exposure category as binary variables among adults with AS or PsA stratified by NSAID use within 6 months of THA or TKA (secondary outcome).
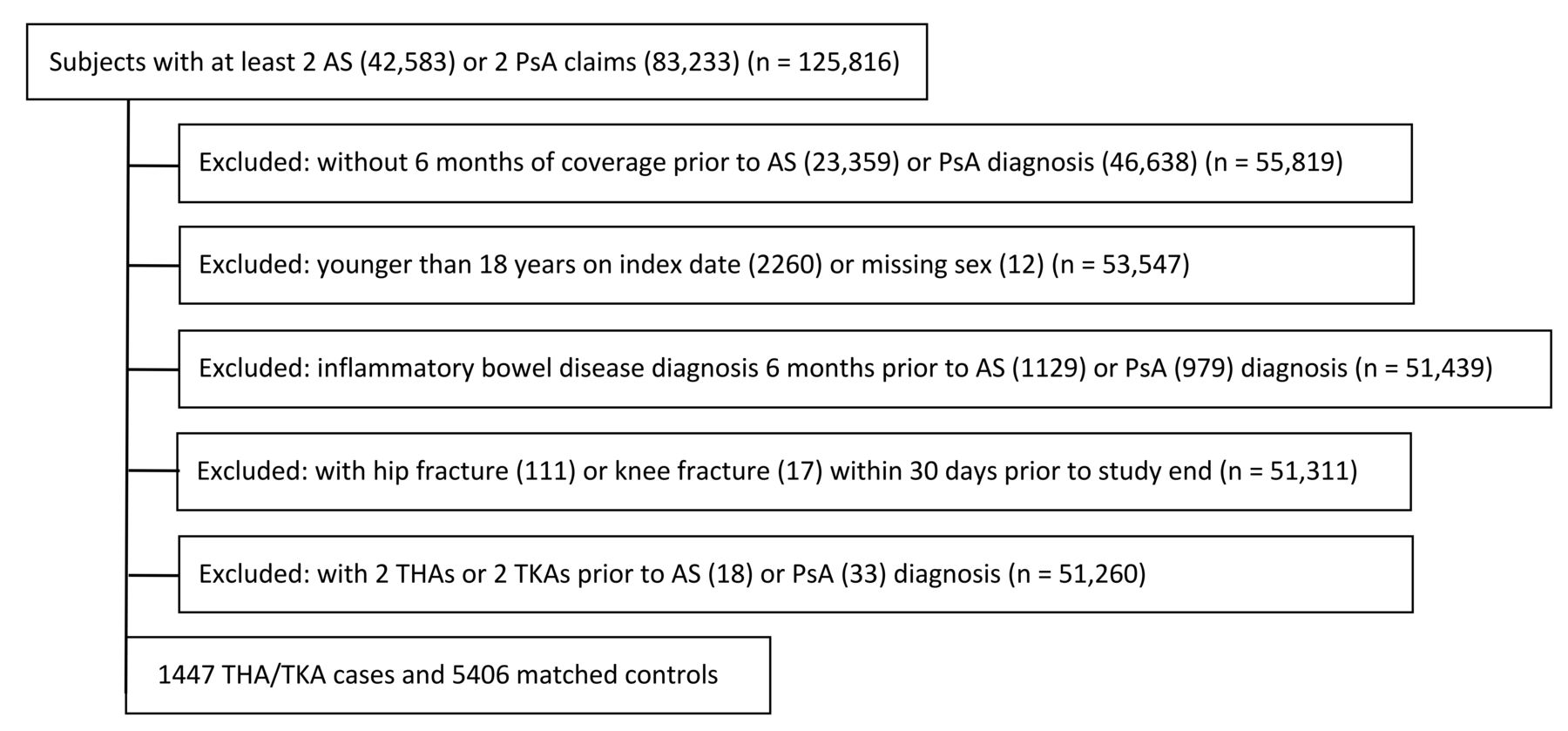
Selection criteria. AS: ankylosing spondylitis; PsA: psoriatic arthritis; THA: total hip arthroplasty; TKA: total knee arthroplasty.
DISCUSSION
In this large, US-based study of adults with AS and PsA, we did not find any protective effects of DMARDs or TNFi for THA/TKA. These null findings were confirmed in several sensitivity analyses assessing subgroups based on SpA subtype, joint (hip vs knee), and age. The only instance TNFi was associated with a higher risk of arthroplasty was during the binary analysis, and this is likely due to confounding by indication. In all other scenarios of TNFi use, the OR was not significantly different from 1, and this could be an indication of effect, as one would expect those using TNFi to be the most severely affected and thus have a higher risk of joint replacement surgery compared to those on DMARDs. Subjects with AS on DMARD/TNFi therapies and no NSAID use had an adjusted OR 1.92, 95% CI 0.91–4.08 for THA/TKA, while those on DMARD/TNFi with NSAID use had an adjusted OR 0.60, 95% CI 0.32–1.14. Because the CIs for both estimates included 1.0, we cannot conclude there is any increased or decreased risk with either treatment category. While subjects with PsA had similar findings, the adjusted ORs were closer to 1 and remained statistically insignificant. Nonetheless, while a statistically significant association of TNFi and lower rates of THA was previously shown in RA, our findings do not support such an association in AS or PsA.12
There are several potential explanations for our findings. These findings may suggest that TNFi have a protective effect on the axial skeleton21 but not on peripheral joints. It is also possible that TNFi do not prevent need for THA/TKA because they are given too late in the disease course, when irreversible damage from inflammatory peripheral arthritis has already taken place. This is a particular concern in axial SpA (axSpA), in which the diagnosis remains delayed by 5–10 years from symptom onset.22,23 Last, they may suggest residual confounding by indication despite our attempts to adjust for disease severity and comorbidities.
According to the most recent guidelines by both the American College of Rheumatology (ACR) and the European League Against Rheumatism (EULAR), NSAIDs are the first line of treatment for axSpA followed by TNFi.24,25 TNFi have been shown to improve disease activity in AS and PsA, making it plausible that this class of medications could reduce the rates of THA and TKA, but this was not observed in our study.1,2 In the most recent guidelines, TNFi were recommended as an option for first-line therapy in PsA.24,25,26 DMARDs are also conditionally recommended for treatment of PsA in some scenarios, but are not recommended for those with axSpA alone due to lack of efficacy.24,25
There were a substantial number of adults in our study on DMARDs, either alone or in combination with other therapies. The most common DMARDs used by subjects in this study were MTX (58.3%), SSZ (11.5%), and HCQ (11.0%; Supplementary Table 2, available with the online version of this article). Some subjects may have used DMARDs specifically to treat peripheral arthritis symptoms, but others may have used them due to their lower cost and safety profile, or due to contraindications to other therapies or intolerance of other medications.
As shown in Table 1, approximately 20% of subjects had a diagnosis of RA in addition to AS or PsA. Patients with PsA are often mistaken to have RA initially, which may be why they have both diagnoses in their claims. Additionally, as suggested here, those with an RA diagnosis in their claims history would be more likely to have peripheral arthritis and therefore may be more likely to receive a THA or TKA.
Limitations. There are limitations to this study. First, this is an observational study, and while we attempted to control for confounding through matching and adjustment for potential confounders, residual confounding remains possible. Subjects with more severe AS or PsA would be more likely to be prescribed TNFi, and their severe disease would put them at risk for THA/TKA. However, this confounding by indication would result in an increased OR for TNFi, whereas we found no significant increase. Alternatively, a healthy user effect may explain our results, in that only the healthiest AS/PsA patients may have been prescribed TNFi, thereby reducing the observed effect of TNFi on THA/TKA. Because we used filled prescriptions to capture medication use, those taking over-the-counter NSAIDs would not be captured. Methotrexate, sulfasalazine, and hydroxychloroquine use in these patients could have been prescribed for conditions other than peripheral arthritis, such as treating psoriatic dermatitis. While the most recent guidelines do not recommend use of MTX, SSZ, or HCQ in axial disease, earlier versions of treatment guidelines did not recommend against MTX and SSZ.25 Therefore, there was a period of time in which these medications were used with the thought that they may prevent antidrug antibody formation among biologic users. We only had 6 months of follow-up for some subjects, and we were unable to capture a large enough sample to perform analysis over a longer period of time. While we adjusted for rheumatology appointments and inflammatory marker testing as a proxy for disease severity, results of standard disease activity instruments were not available. Data on AS/PsA duration were also not available. Another limitation is that we cannot fully exclude the possibility of misclassification of the cases or outcomes; however, our internal validation confirmed the exposure and outcome in all 100 subjects, and procedure codes have high validity in administrative data.27 Last, some of our subjects could have undergone THA or TKA for OA rather than their primary inflammatory arthritis, as diagnostic codes do not distinguish between AS/PsA and OA manifestations of the hip and knee. This is likely not a large issue, as the mean age of cases is relatively younger than those who typically receive arthroplasty for OA.
Strengths of this study include its large sample size, inclusion of adults of all ages, and our ability to ascertain patients’ medication use through prescription fill records. While previous studies have evaluated THA and TKA among subjects with AS, those studies did not ascertain medication use. Further, previous studies were primarily in older adults with Medicare, whereas our study included both commercial and Medicare Advantage beneficiaries, and our analysis stratified by age showed consistent results.28 Additionally, our findings were consistent across a series of other sensitivity analyses.
In this large sample of US adults with AS and PsA, no combination of NSAIDs, DMARDs, or TNFi therapy was associated with fewer THAs or TKAs. Further study should investigate strategies to mitigate end-stage peripheral arthritis in AS and PsA.
Footnotes
M. Dubreuil was supported by the National Institutes of Health (NIH) K23 AR09127, NIH/National Institute of Arthritis and Musculoskeletal and Skin Diseases R03 AR076495, and the Spondylitis Association of America. T. Neogi was supported by NIH K24 AR070892. This work and C. Peloquin, D. Felson, T. Neogi, and M. Dubreuil were supported by the NIH center grant P30 AR072571. Funding sources had no role in the study design, collection, analysis and interpretation of the data, or the decision to submit the manuscript for publication.
The authors declare no conflicts of interest.
- Accepted for publication January 5, 2021.
- Copyright © 2021 by the Journal of Rheumatology








{kind=link}