

Abstract
Objective. To reach a consensus on the instruments to be used in clinical practice to evaluate the effectiveness of biological disease-modifying antirheumatic drug (bDMARD) treatment in patients with psoriatic arthritis (PsA) in the short to medium term (3–6 mos), and to establish the minimum health outcomes for treatment continuation.
Methods. A 2-round Delphi questionnaire was developed based on both the information gathered in the literature review and 4 discussion groups. The suitability and feasibility of the proposed sets of instruments were assessed on a 7-point Likert scale. Consensus was established when at least 75% of healthcare professionals (HCP) reached agreement. To define a minimum health outcome to continue treatment, a combination of 4 disease activity states and 3 health-related quality of life states were defined for 3 hypothetical patient profiles. HCP were given a dichotomous choice (yes/no) to respond to whether they would continue treatment in each case.
Results. The second round was completed by 106 HCP. Consensus was reached on the use of (1) Disease Activity in Psoriatic Arthritis + Psoriatic Arthritis Impact of Disease (PsAID12) or minimal disease activity + PsAID12 + C-reactive protein, in peripheral PsA; and (2) Ankylosing Spondylitis Disease Activity Score + PsAID12, in axial PsA. Health outcomes considered sufficient to continue treatment were stricter for bDMARD-naive patients than for patients who failed several bDMARD.
Conclusion. To the best of our knowledge, this is the first multidisciplinary consensus on a set of outcomes for the evaluation of bDMARD effectiveness in PsA, in routine clinical practice.
- antirheumatic agents
- consensus
- Delphi technique
- patient-reported outcome measures
- psoriatic arthritis
- treatment outcome
Psoriatic arthritis (PsA) is a chronic musculoskeletal disease characterized by heterogeneous manifestations such as arthritis, spondylitis, dactylitis, enthesitis, and/or psoriasis. Nearly 70% of patients with PsA develop skin lesions prior to the onset of arthritis, 15% develop musculoskeletal symptoms first, and both symptoms coexist in the other 15%1. Symptom burden reduces work productivity and increases healthcare costs, particularly in patients with severe PsA2,3,4,5,6. Therefore, health-related quality of life (HRQOL) is commonly impaired in these patients. The most frequent presentations of PsA are peripheral oligoarticular and symmetrical polyarticular arthritis. However, both axial and peripheral involvement may coexist7.
Current therapies aim to prevent the progression of structural damage, maintain functional status, and improve HRQOL8. Development of new biological disease-modifying antirheumatic drugs (bDMARD) has improved disease management and provided better patient care. However, complete disease control has not yet been achieved7,9.
Given the complexity of PsA, a holistic approach is required to assess the effectiveness of treatment10. The combined use of clinical outcomes and patient-reported outcomes (PRO) in clinical practice is a pragmatic way of gaining a comprehensive view of patient well-being11. The Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA) and the group for Outcome Measures in Rheumatology (OMERACT) have jointly developed a core domain to be measured in randomized controlled trials (including both clinical outcomes and PRO). Eight mandatory domains (“inner core”: musculoskeletal disease activity, skin disease activity, pain, patient global, physical function, HRQOL, fatigue, and systemic inflammation) and 4 strongly recommended but nonmandatory domains (“middle circle”: participation, economic costs, structural damage, and emotional well-being) were established10,12. In addition, 4 domains (“outer circle”) were suggested to be further considered in the future.
The GRAPPA-OMERACT effort has defined remission or alternatively low disease activity/minimal disease activity (MDA) as the treatment target13. Nevertheless, no consensus was reached on which measures are more appropriate to assess the disease activity. This lack of consensus is of particular importance given the great heterogeneity of existing instruments13,14, which hinders the holistic and standardized evaluation of treatment effectiveness15,16.
The MERECES group (in Spanish: MEdir Resultados. Consenso de Evaluación en Salud para artritis psoriásica) aims to reach a consensus on the instruments to be used in clinical practice to evaluate the effectiveness of bDMARD treatment in patients with PsA in the short to medium term (3–6 mos) and to establish the minimum health outcomes for treatment continuation.
MATERIALS AND METHODS
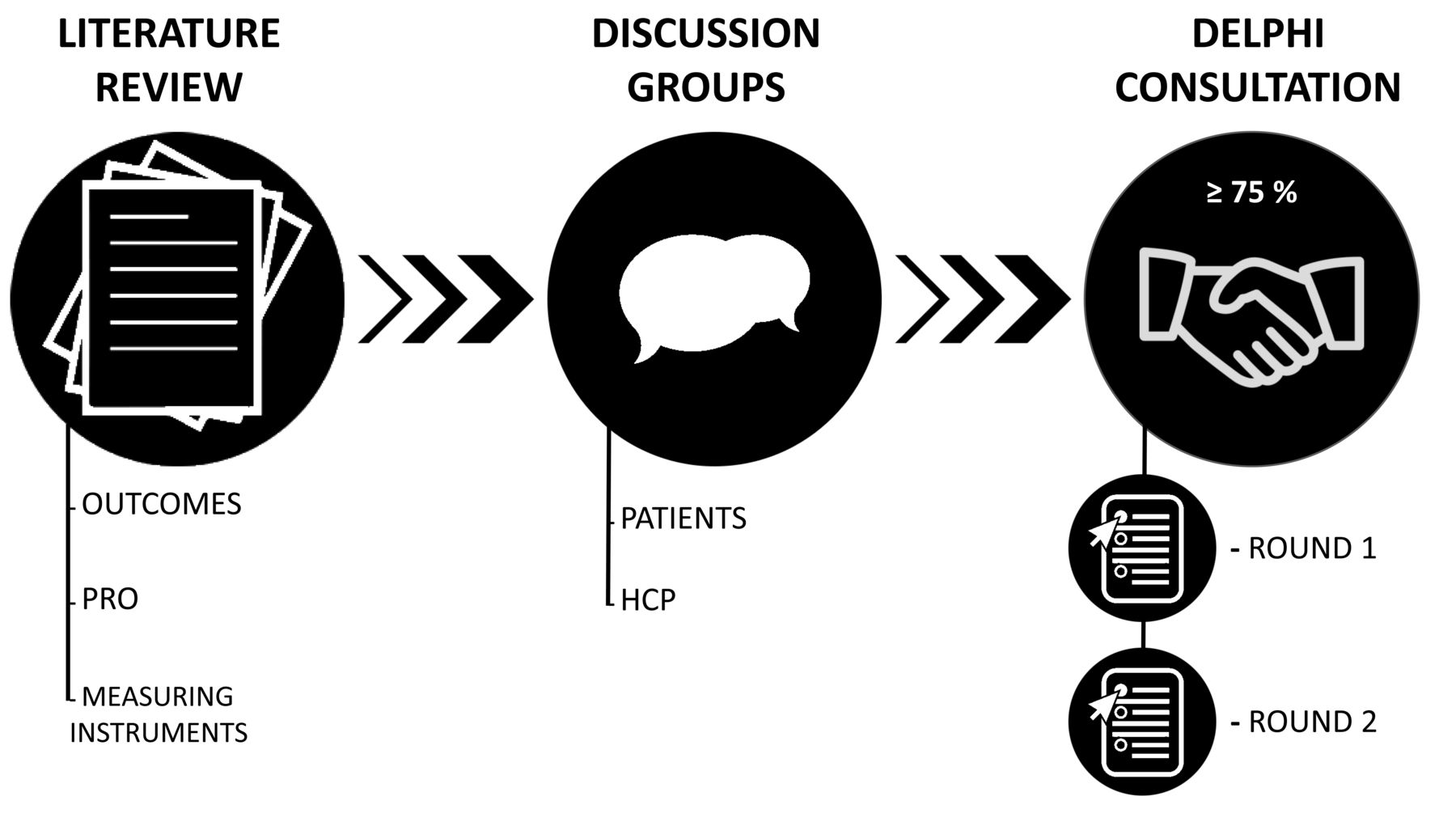
The study comprised 3 phases: (1) literature review, June 2017; (2) discussion groups with patients and healthcare professionals (HCP), January and February 2018; and (3) Delphi consultation, May and July 2018 (Figure 1).

Study design. PRO: patient reported outcomes; HCP: healthcare professionals.
The project was led by a multidisciplinary steering committee consisting of 3 rheumatologists with experience in PsA management, 1 methodologist, and 1 healthcare manager.
Literature review
A literature review was conducted using the international databases (MedLine/PubMed, Google Scholar, Cochrane Library, and ISI Web of Knowledge) to identify clinical outcomes and PRO, and their measuring instruments, for the followup of patients with PsA. It included clinical trials, PsA-related observational studies, and literature reviews published in English or Spanish until June 2017.
Measurement properties of PRO measures
Prior to the HCP discussion group, PRO measures (PROM) identified in the literature review were preselected based on the availability of a validated transcultural adaptation for Spanish patients (if required), number of core domains covered, feasibility of use in clinical practice (≤ 25 items), and psychometric properties (consistency reliability, test-retest reliability, responsiveness, and minimal importance difference). No preselection of clinical instruments was undertaken.
Discussion groups
Four discussion groups were conducted according to the information extracted in the literature review: 2 with PsA patients (n = 15) and 2 with HCP (including rheumatologists, hospital pharmacists, nurses, clinical psychologists, and healthcare managers; n = 19).
Patients with PsA (diagnosed more than 6 mos earlier) taking biological treatment (for at least 3 mos) were invited to participate by the national patient advocacy group Acción Psoriasis. To obtain representatives of the different PsA phenotypes, patients were selected based on their sociodemographic (age and sex) and clinical characteristics (joint disease and skin manifestations, time since diagnosis, time since treatment onset). The main objective of discussion groups was to examine and identify the most relevant health outcomes and their measuring instruments based on the patient’s perspective. In addition, a second objective was to study patients’ willingness to complete questionnaires to assess PROM.
HCP were selected according to their professional experience and interest in the project. The objective of HCP discussion groups was to identify the most appropriate outcomes and the corresponding measuring instruments, to evaluate the effectiveness of bDMARD in routine clinical practice. HCP were asked to define several sets of instruments to take clinical outcome measures and PROM to be included in Delphi questionnaire.
Delphi consultation
The Delphi technique is widely used to achieve a consensus, and allows anonymity between participants and controlled feedback17,18. To obtain agreement on the assessment of treatment effectiveness, 2 Delphi rounds were planned.
A Delphi questionnaire was developed based on both the information gathered in the literature review and discussion groups. The first-round questionnaire consisted of 3 sections:
Sociodemographic and occupational characteristics of participants.
Instrument suitability. It was assessed on a 7-point Likert scale (from 1 = completely disagree, to 7 = in total agreement).
Suitability and feasibility of using the instrument sets proposed for patients, with axial or peripheral involvement in routine clinical practice. The suitability and feasibility of the sets were assessed on a 7-point Likert scale (from 1 = completely disagree, to 7 = in total agreement).
Consensus was established when at least 75% of respondents reached agreement (1–3) or disagreement (5–7).
The second round of the questionnaire was composed of 2 sections: (1) prioritization of agreed instrument sets in the first round, and (2) definition of a minimum health outcome to be achieved in a short to medium term (3–6 mos) to continue treatment. In this section, we defined a combination of 4 disease activity states [remission, low activity, and moderate/high activity with and without clinically important improvement (CII)] and 3 HRQOL states (optimal HRQOL and suboptimal HRQOL with and without CII) for 3 hypothetical patient profiles: (A) a bDMARD-naive patient with PsA; (B) a patient with PsA without structural damage, and functional disability and/or mild-moderate psoriasis, and failure to respond to 1 bDMARD; (C) a PsA patient with structural damage, serious sequelae, and failure to respond to several bDMARD. Panelists were given a dichotomous choice (yes/no) in response to whether they would continue treatment in each case.
Patients with PsA who are achieving remission and optimal HRQOL should continue treatment. This scenario was considered as a test to identify panelists who did not understand the second part of the questionnaire. Therefore, panelists who considered that patients should not continue treatment on achieving remission with optimal HRQOL were excluded from the analysis.
Delphi panelists
There is no agreement in the literature on the appropriate number of panelists for the Delphi method, although a sample of 23 experts has been suggested as sufficient19. We planned to obtain a sample size of 80 panelists. Assuming a potential loss of 50%, a total of 162 panelists were invited to participate in the consultation. They were selected by the promoter and the scientific committee based on their professional experience in PsA management and interest in the project. A minimum of 2 years’ professional experience was required. Panelists received by e-mail the link to the questionnaire, username, and password (unique for each participant). HCP who participated in the discussion groups (n = 19) as well as other rheumatologists and dermatologists (n = 143) were invited. Owing to the nature of the questionnaire, which required specialized clinical knowledge of the disease, patients were not invited to participate as Delphi panelists.
Data analysis
Frequencies and percentile distributions were calculated for each option using Stata statistical software, version 14 (StataCorp.).
Ethics
The study was approved by the Research Ethic Committee of Asturias (nº229/17). All participants received adequate information on the study and agreed to participate by signing an informed consent. To ensure data confidentiality, all documents were duly encoded.
RESULTS
Literature review
A total of 138 publications were reviewed. These publications described 87 instruments used for PsA patient followup (43 PROM, 32 clinical instruments, and 12 composite indices). None of the identified instruments assessed all 8 core domains established by the GRAPPA-OMERACT group.
The composite indices that assess the most core domains are Assessment of SpondyloArthritis international Society criteria (5 domains), MDA (5 domains), American College of Rheumatology criteria (4 domains), Ankylosing Spondylitis Disease Activity Score (ASDAS; 4 domains), Disease Activity in Psoriatic Arthritis (DAPSA; 4 domains) and Psoriatic Arthritis Disease Activity Score (PASDAS; 4 domains).
The psychometric properties of preselected PROM presented to HCP are showed in Supplementary Table 1 (available with the online version of this article).
Patient discussion groups
A heterogeneous group of 15 patients with PsA participated in 2 discussion groups. The sociodemographic and clinical characteristics are presented in Table 1.
Sociodemographic and clinical characteristics of patients.
Patients considered impairment of physical, as well as emotional well-being, to be the most important aspects. In fact, most of them requested psychological support because of the impact of both arthritis and psoriasis. Nonetheless, different opinions were observed according to the severity of arthritis and psoriasis-related symptoms.
The use of PROM in clinical practice was found valuable for PsA management. However, according to the patient’s experience, its use was limited and determined by the particular hospital and Spanish region where the patient received treatment. Participants indicated their willingness to complete PROM not exceeding 15 items at every medical checkup.
HCP discussion groups
A multidisciplinary group of 19 HCP (5 rheumatologists, 4 hospital pharmacists, 2 dermatologists, 2 psychologists, 2 nurses, and 4 healthcare managers) participated in 2 discussion groups.
Participants considered the 8 core domains defined by GRAPPA-OMERACT for the evaluation of patients with PsA to be essential. Regarding the 4 middle circle domains, participants considered participation and emotional well-being relevant but discarded structural damage and economic cost. Structural damage was dismissed because it is irreversible, and its progression is unmeasurable in the short term. Economic cost was not selected because it was considered unsuitable for evaluating treatment effectiveness. The 4 outer circle domains were not considered because they have not been sufficiently established. Therefore, participants agreed to assess 10 out of 16 domains by combining validated composite indices and PROM. Considering the different manifestations of axial and peripheral involvement, specific composite indices were proposed for each one.
Instruments to evaluate disease activity in patients with PsA
Participants selected ASDAS to evaluate axial involvement because it allows for direct measurement, which is easily implemented in clinical practice. The reasons for selecting DAPSA for the peripheral PsA evaluation included its responsiveness, simplicity of calculation and usage, and ability to evaluate 66/68 joints. Further, DAPSA correlated with function and radiographic progression20. It was argued that the 28 joint counts do not necessarily identify commonly affected joints in PsA, such as distal interphalangeal hand joints, and feet joints. For this reason, 28-joint count Disease Activity Score (DAS28), as well as other composite indices evaluating 28 joints, was discarded. MDA was considered as an alternative for both peripheral and axial PsA, because MDA is the only composite index evaluating skin disease. Nonetheless, it was noted that MDA is not a measure of disease activity and does not assess acute-phase reagents such as the C-reactive protein (CRP).
Instruments to evaluate HRQOL in patients with PsA
In relation to PROM, PsAID12 (hereinafter referred to as PsAID) was the only PsA-specific multidomain HRQOL questionnaire found. It is a reliable instrument, developed and validated by the European League Against Rheumatism (EULAR) for use in clinical practice, covering most core and middle circle domains21. HCP agreed to use PsAID rather than the Dermatology Life Quality Index (DLQI) because the latter assesses only skin involvement.
Sets of instruments
Finally, 3 sets of instruments were proposed to reach a consensus in Delphi consultation: (1) DAPSA + PsAID, (2) MDA + PsAID + CRP, and (3) ASDAS + PsAID. Sets 1 and 2 were presented to patients with peripheral involvement and sets 2 and 3 were implemented for patients with axial involvement.
First-round Delphi consultation
Sociodemographic characteristics of the participants are described in Table 2. HCP who participated in the discussion groups (n = 19) as well as other rheumatologists and dermatologists (n = 143) were invited. A total of 115 panelists with a mean PsA management experience of 21.7 years (SD 19.3), representing almost all Spanish regions, completed the first-round questionnaire (response rate 70.9%).
Sociodemographic characteristics of panelists.
Instrument suitability
Most participants considered that both composite indexes DAPSA (89.6%) and MDA (91.3%) were useful to evaluate the efficacy of bDMARD in patients with peripheral involvement whereas only ASDAS was considered useful (90.4%) in patients with axial involvement. PsAID was considered a useful PROM to assess the effect of PsA on HRQOL in patients with both peripheral (83.5%) and axial (76.5%) involvement.
Suitability of sets and feasibility of their use in routine clinical practice
In patients with axial involvement, consensus was reached on the use of ASDAS + PsAID [agreement on suitability (S) 85.3%; agreement on feasibility (F): 86.9%] but not on the use of MDA + PSAID + CRP (S: 69.6%; F: 76.5%). In patients with peripheral involvement, consensus was reached on the use of either DAPSA + PsAID (S: 91.4%; F: 85.2%), or MDA + PsAID + CRP (S: 90.5%; F: 76.5%).
Second-round Delphi consultation
One hundred six HCP completed the second-round questionnaire (response rate from the first-round 92.2%). For peripheral PsA, DAPSA + PsAID were prioritized over MDA + PsAID + CRP (72.6% vs 27.4%).
Health outcomes to qualify for treatment continuation
Responses from 97 participants who answered the test scenario properly were analyzed. Panelists agreed that bDMARD-naive patients with PsA (profile A) should achieve at least low activity (defined as DAPSA ≤ 14 or ASDAS ≤ 2.1) and CII on HRQOL (established as PsAID Δ ≥ 3) within 3–6 months of starting treatment to continue the bDMARD. Experts were less strict in the case of patients with PsA lacking structural damage, and functional disability, and/or mild-moderate psoriasis, and failure to respond to 1 bDMARD (profile B). In this respect, they reached a consensus on continuing bDMARD when patients achieved low activity and CII on HRQOL, or remission (defined as DAPSA ≤ 4 or ASDAS ≤ 1.3) regardless of the HRQOL. Finally, experts agreed to continue treatment when PsA patients with structural damage, serious sequelae, and failure to respond to several bDMARD achieved low activity (independent of HRQOL), or moderate/high activity with CII (defined as DAPSA Δ ≥ 85% or ASDAS Δ ≥ 1.1) and optimal HRQOL (established as PsAID ≤ 4) within 3-6 months of starting treatment (Table 3).
Minimum health outcomes for treatment continuation.
DISCUSSION
The assessment of treatment efficacy in a holistic and standardized approach is challenging in PsA. The main hurdles include heterogeneity of PsA manifestations, transition between phenotypes during disease course, and the wide variety of instruments available16,22,23,24. Currently, Spanish rheumatologists are not following specific criteria to assess the response to biologic therapies in patients with PsA. To some extent, this is due to the absence of specific recommendations in the main national guidelines, such as the one developed by the Spanish Society of Rheumatology25. Our present study shows that the MERECES group has reached a consensus on the instruments to be used in clinical practice for the evaluation of bDMARD effectiveness (in 3–6 mos) in patients with PsA. In addition, experts have agreed on the use of both clinical outcomes and PROM in line with the GRAPPA-OMERACT recommendations.
Aligned with an international task force26 and GRAPPA-OMERACT group recommendations13, the use of DAPSA + PsAID or MDA + PsAID was proposed for followup of patients with peripheral PsA. However, DAPSA + PsAID were prioritized over MDA + PsAID. Research shows DAPSA is a disease-specific, validated, and feasible tool for PsA assessment20,27. Its main advantage compared to other composite indices assessing 28 joints is that DAPSA covers a greater number of joints (n = 68), including some of those commonly affected in patients with PsA that are not covered by DAS2828,29. However, because of the lower time requirements, the DAS28 is still widely used in clinical practice. In addition, the main disadvantage of DAPSA is its lack of skin assessment capacity. Therefore, the GRAPPA-OMERACT group recommends undertaking skin disease evaluation in conjunction with DAPSA measurement13. The HCP discussion groups proposed the combination of DAPSA + PsAID. One of the main limitations of most composite indices (including DAPSA) is that they do not address objective indicators of skin disease, dactylitis, and enthesitis. However, HCP proposed that these domains could be indirectly assessed through the skin and functional ability items contained in the PsAID, which is supported by the differences observed in these items between treatment responders and nonresponders30. Moreover, in Spain most patients with PsA are followed by both rheumatologists and dermatologists. Thus, the extent of skin involvement is usually considered when selecting the more appropriate therapy for the patient.
It is worth noting the importance of monitoring axial symptoms, which usually overlap with peripheral joint affectation. Although axial involvement is less frequent in patients with PsA (12%)7,31, they are more likely to have severe psoriasis, higher tender joint counts, and worse physical function and HRQOL31. Currently, PsA-specific composite indices are not available and nonspecific PsA instruments have been proposed to followup axial involvement. ASDAS has been proposed to evaluate axial PsA, whereas the GRAPPA-OMERACT group does differentiate instruments for each type of disease13,26. HCP recommend the use of ASDAS (plus PsAID) in those patients with prevalent axial involvement because it includes objective and subjective measures32,33.
By combining PRO with clinical outcomes, patients’ disease perception is taken into account, thus providing patient-centered care and complementing clinical practices34. EULAR and GRAPPA-OMERACT groups recommend the use of PRO, which is in line with the American and European drug agencies, for which data related to HRQOL are mandatory for submissions35,36,37. The MERECES group unanimously agreed on the use of PsAID to assess treatment effects on the patient’s HRQOL. PsAID has been developed considering the patient’s perspective, covering nearly all core domains, and has been tested in both clinical trials and real-world settings21,38,39. In addition, individual PsAID items have correlated strongly with other specific PROM, such as the skin item included in DLQI39, supporting PsAID’s ability to assess skin affectation. The GRAPPA-OMERACT group has described PsAID as one of the instruments demonstrating superior measurement properties14.
One of the main factors limiting the combined use of clinical outcomes and PROM in routine clinical practice is the time required to complete them, by both physicians and patients. During the discussion groups, patients showed willingness to complete PROM, even at every appointment, if they did not exceed 15 items (about 5–10 min). Similar results were observed in a previous study in which 115 physicians considered it reasonable to fill in a questionnaire on clinical outcomes requiring < 5–10 min13. Time of ASDAS/DAPSA + PsAID completion is in line with these preferences and with the time per consultation used in Spain (about 30 and 15 min for the first and subsequent visits, respectively).
Current recommendations on PsA patient management state that the conceptual treatment goal should be remission or low disease activity13,25,40. However, the specific criteria to define them is under debate41,42. Although to establish the therapeutic objective of PsA treatment falls outside the scope of this study, our results provide useful information on which health outcomes should be considered as acceptable for continuing treatment. As the disease progresses, such health outcomes may vary, and therefore the MERECES group has defined health outcomes for 3 different patient profiles with increasing levels of severity.
The recommendations provided in this document should be used as an aid to determine bDMARD effectiveness in patients with PsA. However, decisions should also consider the patient’s individual characteristics, values, and preferences, and any further appraisals or possible complications of the disease or treatment.
The main strength of our study is the large number of highly experienced experts from different Spanish regions who participated in the Delphi consultation. In addition, we followed rigorous research methods, with both patient and HCP representation in discussion groups.
Our study has some limitations to take into consideration. HCP were mostly rheumatologists, which may have biased results toward the greater preference for DAPSA (without objective skin assessment) compared to MDA (with objective skin assessment). However, it is important to note that DAPSA feasibility was one of the main reasons for its preference in routine clinical practice. In addition, this consensus has been contextualized within the Spanish health system; results may differ in other countries. Nonetheless, in general terms, the recommendations established in our study are in line with other international approaches (e.g., GRAPPA-OMERACT).
To our knowledge, this is the first multidisciplinary consensus on the evaluation of bDMARD effectiveness in PsA, in routine clinical practice. A combination of clinical outcome measures and PROM has been agreed upon to establish the minimum health outcomes for treatment continuation. The consensus reached may help in making decisions about the continuity of biological therapy, in a standardized manner through appropriate outcome measures.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
APPENDIX 1.
In addition to the authors, these additional investigators of the MERECES Working Group participated in the consensus: Isabel Belinchón, Eugenio Chamizo, Jesús Babio, Raquel Almodóvar, Tamara del Río, José Luis Poveda, Ángel Abad, Carlos Mur, Pablo de la Cueva, Cristina Fernández-Carballido, Beatriz Joven, José A. Pinto, Ana Lozano, Leticia León, José Soto, Eva Galíndez, Mari L. García-Vivar, Ana Ruibal, Natalia Palmou, Raúl Veroz, Esteban Rubio, José L. Álvarez-Vega, Elena Alonso, Jesús Marzo, Laura Garrido, Lola Fabregas, Álvaro García-Martos, María C. Ortega, Consuelo Díaz, Juan C. Nieto, Carmen Torres, Pepe Pérez-Venegas, Jesús Sanz, Pedro Zarco, Santiago Muñoz, Txaro García-Vicuña, Carlos García-Porrúa, Francisco J. Meceiras, Carolina Álvarez-Castro, José A. Hernández-Beriain, Beatriz González, Mireia Moreno, Agustí Sellas, Julio Ramírez, Ana Urruticoechea, Andrés Ponce, Carlos Feced, Angels Martínez-Ferrer, Nagore Fernández-Llanio, Anna Martínez-Cristóbal, Cristina Campos, Arantxa Conesa, Enrique Batlle, Francisca Sivera, Vega Jovaní, Enrique Judez, Manuel Moreno, Fernando Rodríguez-Martínez, Ana María Laiz, Lourdes Mateo, Manel Pujol, Juan C. Torre, Pablo Coto, Jaume Notario, Mercé García-Font, Antonio J. Chaves, Conrad Pujol, Lluis Puig, Esteban Daudén, José L. Sánchez-Carazo, Gregorio Carretero, José L. López-Estebaranz, Anna López-Ferrer, Juan Pereyra, Lourdes Rodríguez-Fernández, José M. Carrascosa, Pedro Herranz, Ricardo Ruiz-Villaverde, Ana Turrión, Andrea M. Cuervo, Carlos A. Montilla, Concepción Delgado, Deseada Palma, José F. García-Llorente, José L. Rosales, José M. Senabre, Juan J. Lerma, María J. Moreno, María López-Lasanta, María R. Oliva, María T. Navío, Patricia Tejón, Santos Castañeda, Sara Alonso-Castro, Senen González-Suárez, Vicente Torrente, Rosa García-Portales, Jorge Cancio, Victoria Navarro, Julio A. Medina, Sergio Rodríguez-Montero, Pilar Ahijado, Azucena Hernández, Cruz Fernández-Espartero, José Antonio Mosquera, Delia Reina, Antonio García, Alejandra López, Ana Uceda, and Joaquín Belzunegui.
Footnotes
The project was supported by UCB Pharma.
- Accepted for publication January 16, 2020.








{kind=link}