

To the Editor:
Psoriatic arthritis (PsA) is a seronegative spondyloarthropathy that develops in 1% to 39% of patients with psoriasis1. It may present clinically in different forms, including distal interphalangeal joint arthritis, asymmetrical oligoarthritis, symmetrical polyarthritis, spondylitis, and arthritis mutilans (AM)2. Although AM accounts for less than 5% of all PsA, it undeniably represents the most severe and disabling form. Therefore, AM requires timely diagnosis and therapy aiming to prevent or block the irreversible destruction of small joints, mainly involving distal interphalanges of digits and toes. However, data on patients with such arthritis have been published as anecdotal reports or as very small series, so that the available information is sparse.
We describe a series of patients with delayed diagnosis of AM, and a systematic review of studies published in the last decade.
Case 1
A 77-year-old woman, with a 37-year history of psoriasis, was diagnosed with PsA at age 55 years when a symmetric polyarthritis involving both hands and feet occurred. She received longterm therapy with different nonsteroidal antiinflammatory drugs (NSAID) without significant improvement of arthritis, because she was intolerant to disease-modifying antirheumatic drugs (DMARD). She refused biological therapy. When significant deformity in phalanges of the left hand developed, she was referred to our ambulatory service. Biochemical tests revealed erythrocyte sedimentation rate (ESR) 50 mm/h, C-reactive protein (CRP) 5.84 g/l; clinical assessment showed pain score 70 on 100-cm visual analog scale (VAS), Health Assessment Questionnaire (HAQ) score 1.75, swollen joint count (SJC) = 6, tender joint count (TJC) = 5, and DJC = 5. Figure 1A illustrates AM involving the hands. We suggested biologic therapy with an anti-tumor necrosis factor-α (anti-TNF-α) agent, but she declined treatment.
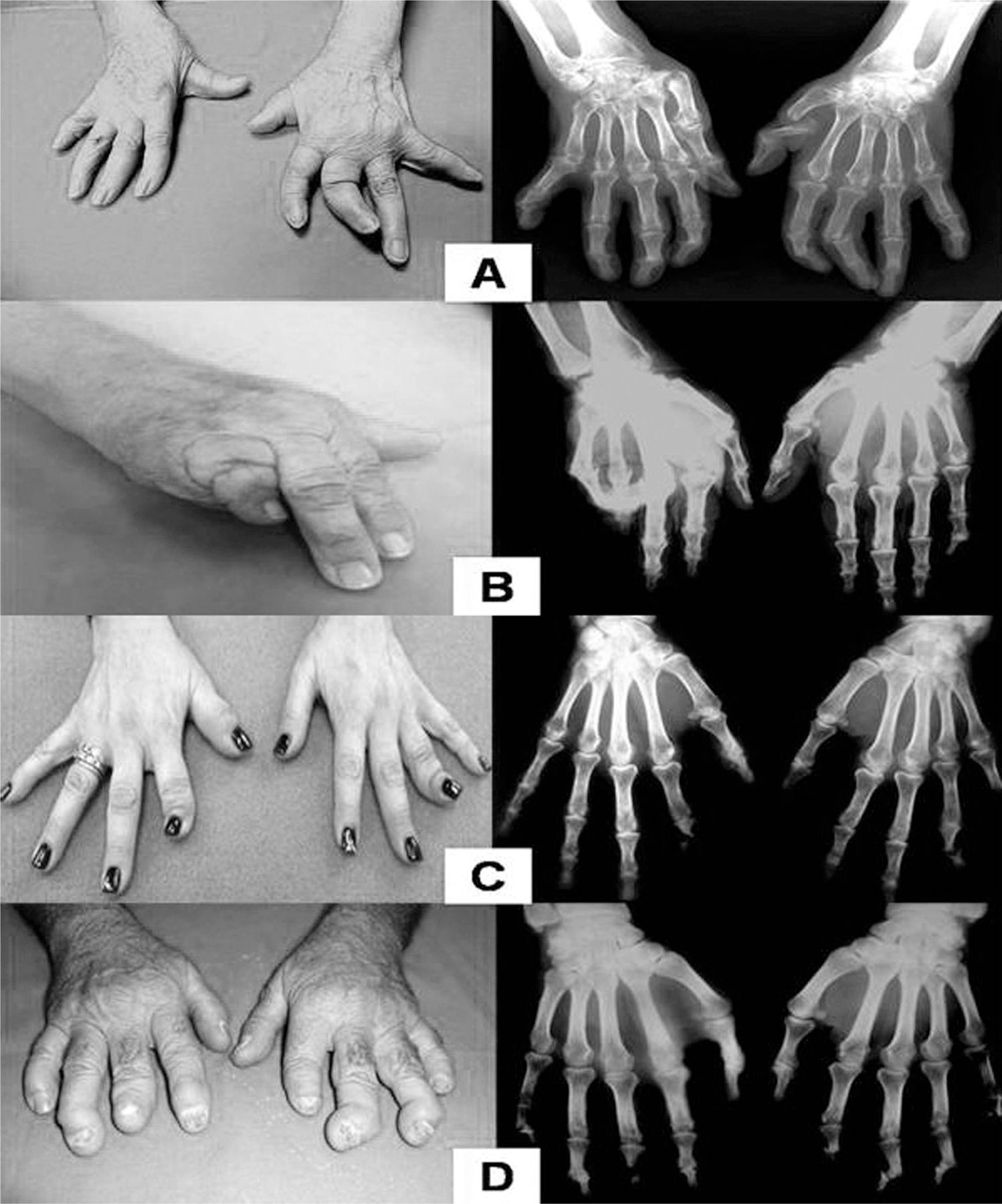
Destructive involvement of distal interphalangeal (DIP) joints and subluxation of the metacarpophalangeal joints (A). Mutilation of fourth and fifth digits of the right hand (B). Destructive involvement of the DIP joints, with telescoping of second finger of the right hand and fourth finger of the left hand (C). Shortening of third finger of right hand and second finger of left hand, and subluxation of DIP joints; onycholysis is also evident (D).
Case 2
A 74-year-old woman developed psoriasis at the age of 20 years and arthritis when she was 45 years old, with both axial and peripheral involvement. Therapy with indomethacin 50 mg daily achieved adequate control of arthritis-associated pain, so that no other therapies were performed. However, she was referred to our center with the following measures: ESR 43 mm/h, CRP 2.39 g/l, VAS for pain 50, HAQ score 1.25, SJC = 5, TJC = 3, and DJC = 4. Figure 1B shows the patient’s hands with AM. She refused treatment with a biologic therapy despite information on the potential benefits for cutaneous and rheumatic manifestations.
Case 3
A 62-year-old woman with a 25-year history of psoriasis was diagnosed with PsA at age 50 years. She was irregularly treated with DMARD and with some cycles of etanercept, which she discontinued because of an “intolerance.” Consequently, she remained without any therapy for several months. At clinical assessment, ESR was 25 mm/h, CRP 1 g/l, VAS for pain = 30, HAQ score = 0.75, SJC = 2, TJC = 2, and DJC = 3. Figure 1C shows her hands. She declined reintroduction of biologic therapy.
Case 4
A 70-year-old man with psoriasis at age 40 years developed arthritis involving the hands when he was 63 years old. He had previously received NSAID with nonsignificant control of pain, but no DMARD therapy. Referred to our clinic, he provided a radiograph with features of AM of the hands (Figure 1D). We undertook biochemical tests to start an appropriate therapy, but the patient was lost to followup.
Literature review
A literature search was performed in PubMed with MeSH terms “psoriatic arthritis mutilans” and “opera-glass hand” for the period January 2002 to December 2012. Only studies in which clinical data of patients with AM were specifically reported were extracted. Full articles of all relevant studies were retrieved, and manual searches of reference lists from these articles were performed, identifying 14 suitable studies (Figure 2)3,4,5,6,7,8,9,10,11,12,13,14,15,16. Including our series, a total of 120 patients with AM are described (Table 1). It was impossible to extrapolate data for 37 other AM cases reported in 5 studies because they were cumulatively described among other patients with PsA17,18,19,20,21. There was a weak prevalence of the male sex, with male/female ratio being 1.29. Duration of psoriasis and PsA before diagnosis of AM ranged from 10 to 52 years and 6 to 35 years, respectively; acute onset of AM (3 months) was reported in 1 patient9. In 4 cases, psoriatic AM was associated with Charcot-like joint disease6, while 1 patient presented with an axial bone proliferation causing cervical myelopathy12. In the largest series3, the AM was significantly associated with arthritis duration, involvement of distal phalanges, and reduced functional capacity. The prevalence (55%) of psoriatic nail involvement in AM did not differ from that of other psoriatic patients3. A study found that bone edema, erosion, and proliferation on magnetic resonance imaging (MRI) were significantly more severe in the patients with AM than in controls4.

Identification of studies of arthritis mutilans (AM).
Clinical characteristics of patients with arthritis mutilans (AM) reported in the last decade.
Therapy with 1 or more DMARD was performed before AM diagnosis in all but 1 patient, although such therapy was carried out irregularly in the majority of cases. Following AM diagnosis, biologic therapy with etanercept was performed in 6 cases (Table 1). The functional capacity improved significantly in 3 cases, with recovery of some movements allowing patients to make a fist and to walk easily7. Of note, therapy provided a stable bone disease without onset of new mutilation, as documented by radiographic features at 2-year followup in 2 other cases14. Unfortunately, no followup is available for the remaining AM patient treated with etanercept13.
AM involves fewer than 5% of patients with PsA1, the disease being particularly infrequent in Asian countries. Recent studies found an AM prevalence ranging from 1.5% to 4.9%18,20,21. AM represents an aggressive form of arthritis characterized by marked erosion of small joints of hands and feet, progressing to irreversible joint disruption. The resulting finger and toe mutilations severely impair patients’ functional capacity. Much more effort is required to diagnose those patients whose PsA is progressing toward mutilation in an earlier stage. Development of AM has been associated with a longer arthritis duration, involvement of distal phalanges, and impaired functional capacity3, suggesting these patients should undergo tight disease control and therapy. Radiological assessment of joints may be useful for clinical management of PsA. A study found that as many as 23% of patients with PsA have damage at the initial visit that was not detectable at clinical examination22. Similarly, it has been found that joint erosions are detectable at early radiographic assessment in nearly 50% of patients, i.e., within 2 years of arthritis23. Another study found that bone edema, erosions, and proliferation assessed with MRI scans were significantly more severe in patients with psoriatic AM than in those with other forms of PsA, suggesting that bone edema visible on MRI may be a pre-erosive feature of arthritis4. Thus, it is possible to diagnose early joint alterations in psoriatic patients in advance of their clinical manifestation.
An early treatment may prevent joint damage and irreversible finger destruction. A trial showed that structural joint damage in patients with PsA was significantly prevented by infliximab therapy, and that even a 6-month delay in starting such therapy was associated with a lower therapeutic gain18. A dramatic repair of joint damage has been observed in a patient with PsA following 2 years of etanercept therapy, with fill-in and disappearance of typical destructive erosions in both fingers and toes24. Similar observations were described by others in clinical practice25.
Thus, biologic therapy may reduce radiologic progression and possibly induce regression of erosive damage in such patients. Such therapy could prevent or significantly delay the development of AM, but data for this remain scarce. Our review included 6 cases in whom the etanercept therapy was performed after AM diagnosis, that is, when both joint and bone alterations were already irreversible. However, the absence of progression at 2-year followup would suggest that such therapy may be beneficial even in these cases. In 1 patient from our series, etanercept was administered before onset of AM, but only a few irregular therapeutic cycles were administered because of patient refusal, so no reliable conclusions can be drawn from that case.
Different guidelines suggest that psoriatic patients with peripheral arthritis should receive anti-TNF-α therapy (grade A) or DMARD (grade B) following failure of NSAID26. Unfortunately, all our patients declined consent for such therapy. In our practice, such diffidence is much less evident in patients with other rheumatic diseases or inflammatory bowel diseases. Speculatively, it cannot be excluded that a general reluctance of these patients to accept effective drugs, including biologic agents, may be a factor for the development of AM.
AM is an infrequent but highly disabling form of PsA. Based on our findings, therapy with DMARD seems unable to prevent its development. A potential role for biologic therapy is expected, and prospective studies are urged.








{kind=link}
{kind=link}