Article Text

Statistics from Altmetric.com
According to the classification criteria of antiphospholipid syndrome (APS), lupus anticoagulant (LA), anticardiolipin (aCL) and anti-β2-glycoprotein I antibody (aβ2GPI)assays are independent risk factors for the occurrence of vascular thrombosis and pregnancy loss.1 It is generally accepted that patients carrying multiple positivity for antiphospholipid (aPL) antibodies have a more severe disease and higher recurrence rate despite treatment. On the other hand, the stable positivity of a single test is sufficient to classify a patient as having APS.2 As a consequence, clinicians have been wondering whether patients with similar clinical features, but with different positivity patterns (profiles) in the three aPL tests, should be considered completely comparable or not.
We retrospectively studied 3088 consecutive patients who were referred within a 24-month period (January 2007 to January 2009) to coagulation laboratory for the following indications: (A) suspected thrombophilia (thrombotic diathesis), (B) suspected obstetric APS, (C) unexplained prolonged clotting time, (D) other haemostatic problems if a prolonged and inhibited phospholipid-dependent clotting time was found, (E) screening in co-existent autoimmune disease. LA, aCL (ELISA kit, Phadia, EliA Cardiolipin IgG/IgM, Uppsala, Sweden) and aβ2GPI (ELISA kit, Phadia, EliA ß2GliocproteinI IgG/IgM) were searched in all the 3088 patients. LA measurement included four tests: dilute Russell's viper venom time (dRVVT, Hemosil, LA-screen/confirm, Instrumentation Laboratory, Lexington, Massachusetts, USA), partial thromboplastin time-LA (PTT-LA; Diagnostica Stago, Asnieres, France), silica clotting time (HemosIL; DiaPharma Group, Ohio, USA) and kaoline clotting time (homemade, according to Exner).3 If PTT-LA was prolonged, the hexagonal phospholipid neutralisation test was performed as a confirmation (STACLOT-LA, Diagnostica Stago). In 200 subjects (6.5%), LA was positive on two occasions; and of these, 72 (36%) patients were diagnosed as having APS, according to the revised criteria.2 In 425 subjects (13.8%), aPL (aCL and /or aβ2GPI, detected according to current criteria 2) were present in two occasions, in the absence of LA; and of these only 4 (0.9%) were diagnosed as having APS. Details are shown in table 1.
Epidemiologic, clinical and serologic characteristic of the subjects enrolled in the study
Using these data, we set-up a risk model for APS diagnosis based on aPL positivity, their titre and methods used for LA research. Estimates for the probability of APS diagnosis were derived from logistic regression equations.
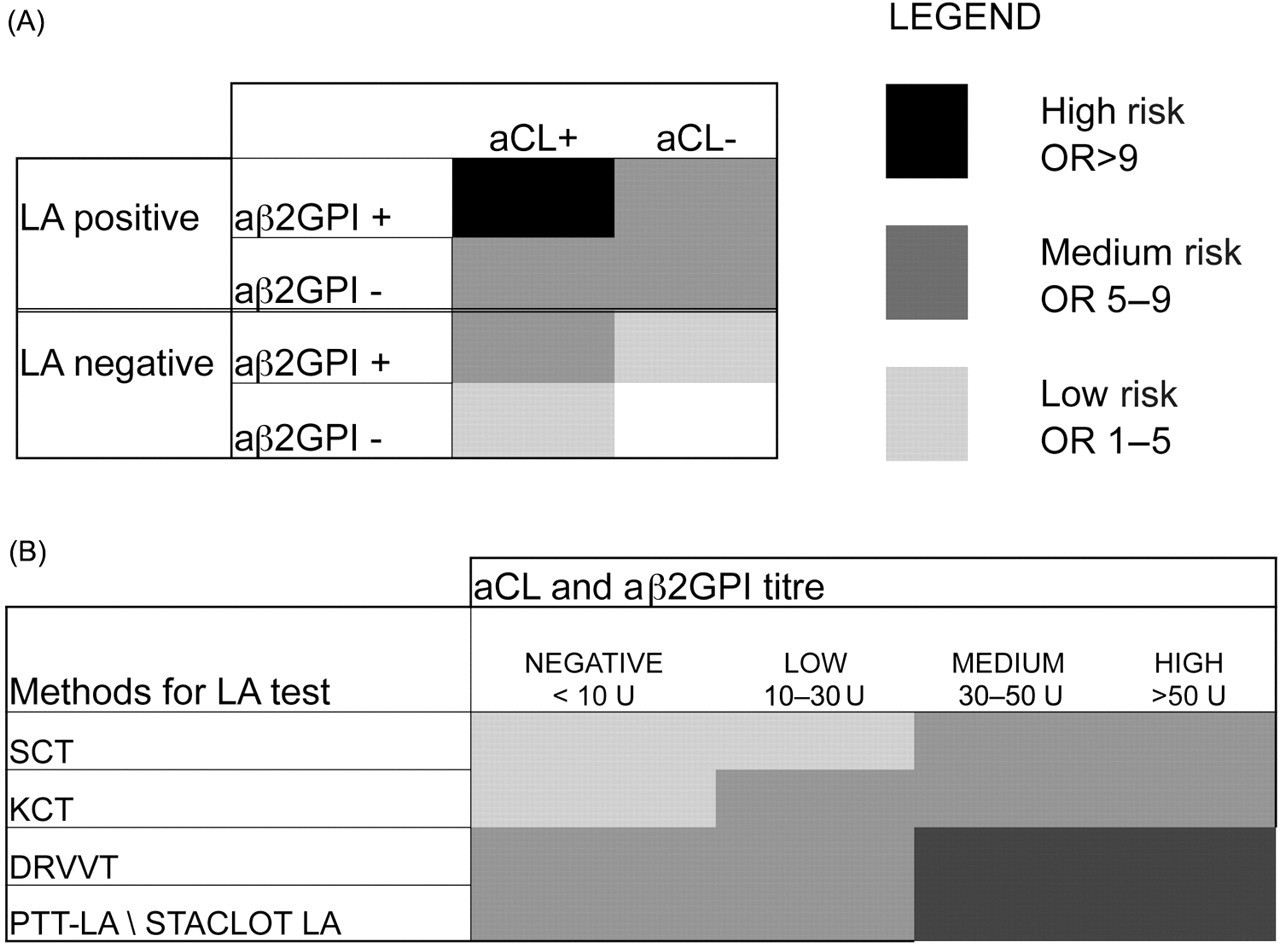
The resulting chart (figure 1) shows that multiple aPL positivity, particularly the triple association of LA, aCL and aβ2GPI, increases the risk of APS. Among the aPL, LA is more strongly associated with the diagnosis of APS, particularly if detected with PTT-LA/STACLOT-LA or dRVVT. Interestingly, multiple positivity for different LA tests is not associated with a higher risk. Besides, the risk is estimated as ranging from low risk to high risk, according to subclassification of subjects based on aCL and aβ2GPI titres (as defined in figure 1).
{kind=link}
Risk model for antiphospholipid syndrome (APS) diagnosis based on antiphospholipid (aPL) positivity, their titre and methods used for lupus anticoagulant (LA) research. (A) APS risk is estimated according to aPL profile, showing that each further positivity increases the risk of APS diagnosis. Multiple aPL positivity, particularly the triple association of LA, anticardiolipin (aCL) and aβ2GPI, further increases the risk of APS. (B) Chart for the risk of APS shows risk ranging from low to high risk based on aPL (aCL and aβ2GPI) titres and methods for LA research (dRVVT, PTT-LA/STACLOT-LA, SCT, KCT). In our experience, a titre of 30 U/litre represents a value ≥99 percentile (according to current criteria), thus we set this cut-off value to determinate moderate aCL and aβ2GPI positivity. The 50 U/litre as cut-off value for high titre was set arbitrarily. The highest aCL or aβ2GPI isotype was used in the analyses. aPL, antiphospholipid; aCL, anticardiolipin; LA, lupus anticoagulant; aβ2GPI, anti-β2-glycoprotein I antibody; dRVVT, dilute Russell's viper venom time; PTT-LA, partial thromboplastin time-LA; SCT, silica clotting time; KCT, kaoline clotting time.
These data suggest a substantial improvement in risk prediction of APS diagnosis based on the assessment of the aPL profile, having the advantage of the quantification of such a risk by APS risk scale.
From a speculative point of view, such an approach on the subclassification of patients based upon different combinations of positive tests may in future influence not only the prognostic judgment but also, more critically, the pharmacological treatment.
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.