Article Text

Statistics from Altmetric.com
Recently we reported on a good clinical response at week 24, especially in tumour necrosis factor (TNF)-blocker-naive patients with ankylosing spondylitis (AS) who were treated with a first course of rituximab (two infusions of each 1000 mg of rituximab with 100 mg methylprednisolone at baseline and week 2).1
Here we report on the follow-up of these patients with a special focus on the good responders.
At week 24, patients regarded as responders were offered to be followed up and to receive a second course of rituximab in case of flare. A response was defined as reaching 20% improvement in disease activity according to the Assessment of SpondyloArthritis international Society criteria (ASAS20)2 compared with screening on at least two consecutive visits (out of four visits: week 12, week 16, week 20 and week 24). Flare was defined as a 1.5-point worsening of the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) compared to the lowest BASDAI between week 12 and week 24. Flare patients were then followed for another 48 weeks (between the flare visit (=R-baseline) and R-week 48; R=re-treatment). Patients who did not flare were followed between week 24 and week 48 without further treatment. Clinical outcome assessments were performed as reported before.1
Statistical analysis was performed as an intention-to-treat analysis. The non-parametric Wilcoxon signed rank test was used to compare changes between baseline to after-treatment values; p values <0.05 were considered significant.
Among the nine responders, there were six TNF-naive and three TNF-blocker failure patients. Five of the nine responders flared, and the other four patients were followed until week 48 without further treatment.
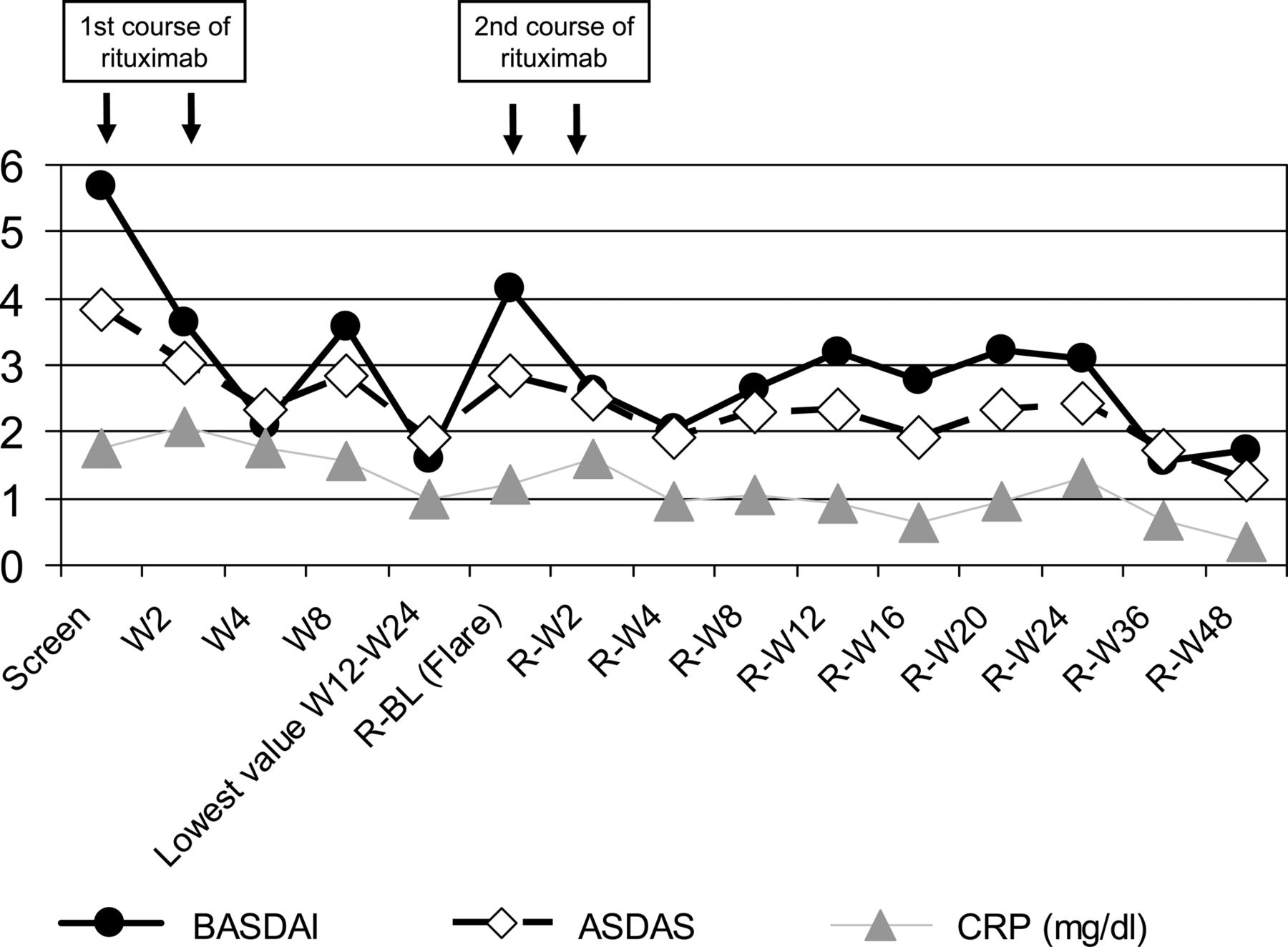
In the five flare patients who received a second course of rituximab, the mean BASDAI at screening decreased from 5.7 (±1.9) to a lowest mean value of 1.6 (±1.6) (this was the lowest value between week 12 and week 24), increased to 4.2 (±1.6) at the time of flare and reached a value of 1.7 (±1.5) at R-week 48 after application of a second course of rituximab (table 1 and figure 1). The development of the Ankylosing Spondylitis Disease Activity Score (ASDAS) and C reactive protein (CRP) even showed lower mean values at R-week 48 compared to the lowest value between week 12 and week 24 (table 1 and figure 1).
Efficacy parameters in (A) the group of patients who received a second course of rituximab and (B) the group of patients who were followed until week 48 without further re-treatment
{kind=link}
Mean Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), Ankylosing Spondylitis Disease Activity Score (ASDAS) and C reactive protein (CRP) between screening and re-treatment week 48 (R-W48) in the subgroup of patients who received a second course of rituximab.
Due to the small number of patients, p values were not significant. BASDAI50 response and ASAS partial remission at R-week 48 were reached only by the two TNF-naive patients; these two patients reached also ASDAS inactive disease with an ASDAS <1.3.
Therefore, the five patients who received a second course of rituximab showed even a better improvement in BASDAI, ASDAS and C reactive protein at R-W48 compared to the first course of treatment.
In the four responders (among them three TNF-naive) who did not flare and were followed until week 48, a constant and stable response was observed until the end of the follow-up period at week 48 (table 1B).
Thus, all patients (45% of the initially treated patients) who were regarded as responders at week 24 showed a good clinical response at the end of the first year, about 50% each with and without a second course of rituximab treatment.
Based on the experience with other immunosuppressive drugs which showed no clinical response (anakinra,3 methotrexate,4 abatacept,5 tocilizumab6 or sarilumab7) in AS, the response rate in the TNF-naive group seen in the present trial might be real.
The reasons for a potential effect of rituximab in AS are not clear but have briefly been discussed previously.1 A larger controlled study evaluating the role of a B cell directed therapy in active AS seems to be justified.
Acknowledgments
We like to thank Roche Pharma AG for study drug supply and for financial support of this study. We like to thank the study nurses in Berlin (Beate Buß, Renate Pauli) and Herne (Dagmar Krinitzki, Nadja Siebert) for performing the studies.
Footnotes
-
Contributors I-HS: study design, project management, patient recruitment, data analysis, data interpretation, manuscript preparation. FH: patient recruitment. MR: study design, data interpretation. JL: statistical analysis. HA and JB: data interpretation. IH-R: project management. JS: study design, principal investigator, sponsor, data interpretation, manuscript preparation.
-
Funding This study was supported by an unrestricted grant from Roche.
-
Competing interests This study was supported by an unrestricted grant from Roche. IS and FH: Wyeth Pharmaceuticals, Merck Sharp Dohme/Schering Plough, Abbott Immunology Pharmaceuticals: consulting fees or other remuneration. IR: employee from Roche Pharma AG. MR, JB and JS: Wyeth Pharmaceuticals, Merck Sharp Dohme/Schering Plough, Abbott Immunology Pharmaceuticals, UCB: consulting fees or other remuneration. HA and JL: none.
-
Patient consent Obtained.
-
Ethics approval Ethics approval provided by Landesamt für Gesundheit und Soziales, Geschäftsstelle der Ethik-Kommission des Landes Berlin, Sächsische Straße 28, 10707 Berlin, Germany.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement We collected blood for cytokine analysis.