Article Text

Statistics from Altmetric.com
The Disease Activity Score1 is widely used to quantify disease activity and gauge response to treatment. A rather complex calculation conceals the relative contribution of each measure to the composite score. The 28 joint version (DAS28) is used in the British Society for Rheumatology guidelines to determine response to anti-tumour necrosis factor α (anti-TNFα) treatment.2 A reduction in DAS28 of ⩾1.2 is considered significant improvement, as is a reduction in DAS28 score to <3.2. These figures are important, as under current guidelines clinicians are advised to discontinue anti-TNF treatment if either of these criteria is not achieved at 3 months.
In the course of reviewing decisions on whether or not to continue anti-TNF therapy, we identified several patients in whom the change in DAS28 score did not correlate with clinical findings. It was also noted that the clinicians relied heavily on the change in DAS28 score to determine if the treatment should be continued. In some cases, a relatively insignificant change in erythrocyte sedimentation rate (ESR) seemed to be responsible for a disproportionately great change in the DAS28 score.
To give an example, a 53 year old patient was treated with infliximab. At baseline his patient global assessment was 24, he had 10 swollen and five tender joints, and his ESR was 13 mm/1st h, resulting in a DAS28 score of 5.25. At the 3 month review the patient global assessment was 25; there were eight swollen and two tender joints, and the ESR was 4 mm/h. The second DAS28 score was 3.8, an impressive improvement of 1.45. Thus, even though there had been little or no discernible improvement, the DAS28 response exceeded the cut off point of 1.2 stipulated in the BSR guidelines. In this case, the guidelines advise continuation of treatment.
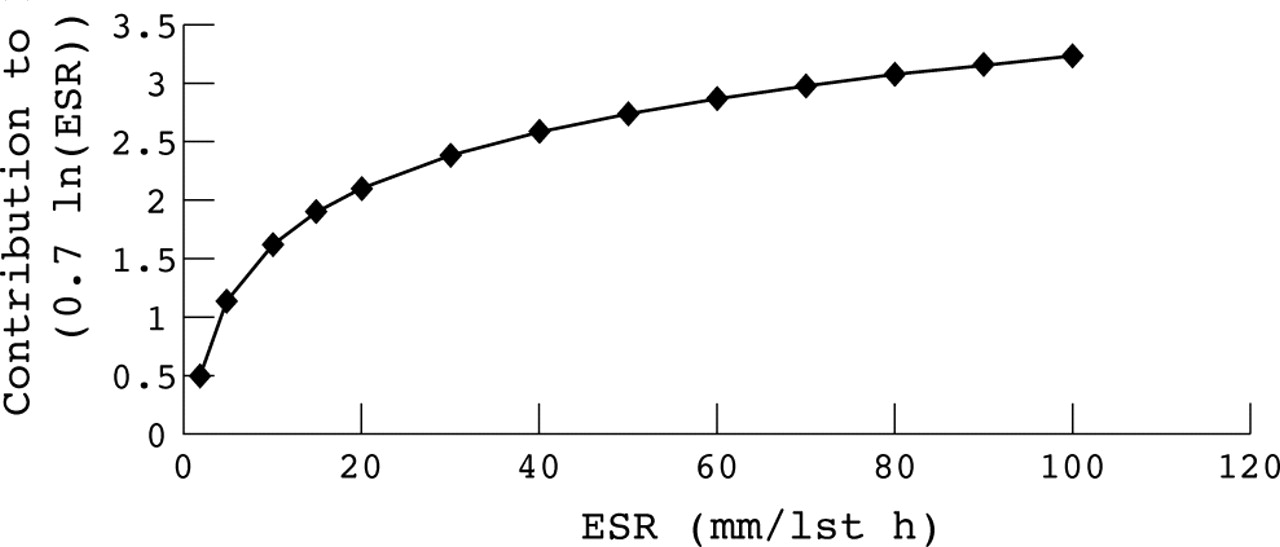
Figure 1 shows the contribution of the ESR to the DAS28 score. As a result of the log transformation of ESR values used to calculate the DAS28 score, changes in ESR below 20 mm/1st h have an inordinately large effect on the change in DAS28 score. Patients with a low initial ESR are thus more likely to show greater improvements in the DAS28 score than those with a high initial ESR. The contribution of an ESR change of 17 to 2 mm/h to the change in DAS28 score is 1.5, whereas a change in ESR from 90 to 60 mm/1st h would have contributed just 0.27.
{kind=link}
Contribution of ESR values to the DAS28 score.
The DAS28 score continues to be a useful tool in clinical practice, particularly when auditing response to treatment in groups of patients. We would, however, caution against the use of the DAS28 score as the main response criterion in an individual patient, where the score seems to conflict with the assessments of the patient and clinician. In these cases misinterpretation may be avoided by careful evaluation of the individual components of the DAS28 score. It may be necessary to modify the guidelines to take into account situations where the change in DAS28 score is not representative of the clinical situation.