Article Text

Statistics from Altmetric.com
INTRODUCTION
In this issue of the Annals of the Rheumatic Diseases, Gisondi et al (see page 26) present an ultrasonography study showing that otherwise asymptomatic patients with psoriasis often have evidence for subclinical disease involving the enthesis (ie, the site of insertion of a tendon, ligament or joint capsule to bone).1 The authors suggest that this may represent a useful approach for the future prediction of which patients with psoriasis will eventually develop an associated arthropathy. While the value of such a strategy in otherwise healthy patients with a common disease such as psoriasis is debatable, it is clear that, if validated and reproduced, the present findings could have far reaching consequences for understanding the link between skin and joints in psoriasis. In particular it further challenges the concept that the primary link between skin and joint disease is related to common autoimmune mechanisms affecting the skin and synovial membrane. Given that entheses are sites of particularly high joint stressing, it further supports the alternative emerging view that the link could be a biomechanical one.
WHAT ULTRASOUND SHOWED IN ASYMPTOMATIC ENTHESES IN PSORIASIS
In the study, the authors used an ultrasound-based approach to examine five asymptomatic entheses in the region of the knee and heel (insertion of the quadriceps tendon, both ends of the patellar ligament, the insertion of the Achilles tendon and the calcaneal attachment of the plantar aponeurosis) in subjects with psoriasis, using the previously reported system from the Glasgow group: the Glasgow Ultrasound Enthesitis Scoring System (GUESS).2 An enthesis is composed of both soft tissue components (ligament, tendon and their associated fibrocartilages) and hard tissue components (calcified fibrocartilage, immediately adjacent bone (the “subchondral bone plate”) and the underlying trabecular network).3 While magnetic resonance imaging (MRI) is well suited to depicting the adjacent osteitis that may accompany enthesitis, ultrasound is probably the imaging modality of choice for looking at the soft tissue components of the enthesis and the bone surface, where both entheseal-related new bone formation and erosion may be discerned.4
The sonographic soft tissue changes associated with enthesitis include loss of normal fibrillar architecture of tendons or ligaments at insertions, hypoechoic change compatible with inflammation and associated thickening of the attachment site.5 Another feature of enthesitis is oedema in the immediately adjacent tissues.6 It is important to point out that thickening of an enthesis per se does not necessarily imply the presence of inflammation, and that thickening of Achilles tendons in athletes may be a normal response to prolonged exercise.7
The present study showed thickening of the enthesis that was related to body mass index in both psoriatic patients and in normal individuals. This likely reflects physiological functioning and not disease. However, the authors found significantly more hypoechoic thickening and a loss of normal enthesis fibrillar architecture in more psoriatic patients compared to controls. Hypoechoic thickening and loss of fibrillar architecture are two ultrasound abnormalities indicative of inflammation at enthuses.1
Another very interesting finding in the psoriatic patients was low-grade retrocalcaneal bursitis, but the authors did not comment specifically whether this was related to inflammation at the Achilles tendon insertion. In any event, it is important to recognise that some parts of the Achilles enthesis organ actually form the walls of the retrocalcaneal bursae and are thus juxtaposed to synovium, thus forming a functional unit called a “synovio-entheseal complex”.8 It has recently been emphasised that the entheseal organ fibrocartilages of the Achilles tendon insertion are likely to be nourished and lubricated by synovium.8 Furthermore, microdamage of these fibrocartilages may be linked to adjacent synovitis.9 Therefore, we stress that these synovial related abnormalities could represent an integral component of the entheseal related pathology. As the walls of the retrocalcaneal bursa are part of the enthesis organ itself, the present findings are compatible with an immunopathology related to the enthesis.8
The authors also noted new bone formation at insertions in psoriatic patients. It would be tempting to assume that this represented a reaction to a previous bout of entheseal related inflammation and that new bone formation then ensued. However, this may not be the case as experimental studies in a murine model with features of psoriatic arthritis (PsA) have suggested that the relationship between inflammation and new bone formation may not be as straightforward as originally envisaged, since new bone formation may not be closely linked to the presence of inflammation.10 It was worth noting that small enthesophytes were present in controls and likely represent a normal variant, and it is just that the increased sensitivity of ultrasound is detecting changes not previously noted in normal individuals.
In the limited number of entheses assessed, the authors found a greater number of abnormalities in the psoriatic cases compared to the controls. Had it been possible to study more attachment sites, it is probable that abnormalities would have been present in an even greater proportion of cases. Indeed, given the prevalence of subclinical entheseal disease in the present study, one must ask the question that, if technology permitted and all entheses could be systematically evaluated, might subclinical entheseal abnormalities be universal in patients with psoriasis? Also, might there be differences between type 1 and type 2 psoriasis? And could the entheseal abnormalities be more closely related to plaque psoriasis rather than other variants?
EVIDENCE OF ENTHESITIS IN OTHER IMAGING STUDIES IN PSORIASIS WITHOUT ARTHRITIS
The findings of this study resonate with an important investigation from the 1970s in which Namey and Rosenthall demonstrated that in patients with psoriasis but no joint symptoms, bone seeking isotopes were taken up in a periarticular distribution.11 Given the strong functional interdependence between the enthesis and adjacent bone surfaces (that may be lined by fibrocartilage, forming part of an enthesis organ), a conceptual link between these pioneering studies and enthesitis now exists. Another imaging study published in the dermatology literature utilising conventional MRI showed that hand abnormalities were common in patients with psoriasis but not in healthy controls.12 Specifically, pericapsular tissue oedema that we would consider to be linked to an entheseal associated pathology was noted in asymptomatic finger joints in subjects with psoriasis.12
FUTURE STRATEGIES USING ULTRASOUND IN SUBJECTS WITH PSORIASIS BUT NOT ARTHRITIS
Although intriguing, the present findings must be taken as preliminary and need to be reproduced and extended. However, the wide availability, low costs and ability to scan repeatedly should allow ultrasound observations to be extended in a systematic way, unlike the previous nuclear medicine and MRI studies in normal individuals that have not been validated. The ease of access and utility of ultrasound in the assessment of the enthesis offers a major advantage over MRI and nuclear medicine. The authors are to be congratulated on the degree of forethought that was given in matching psoriasis cases with controls for body mass index (BMI). Also, the steps taken by the sonographers to avoid direct contact with patients so as not to see the psoriasis and scanning in a darkened room would help reduce bias. However, in those patients with plaque psoriasis around the knee, it would be difficult not to be aware of this. Furthermore, there is the issue of validation of the findings where the gold standard must always be histological assessment. While ultrasound is validated for florid synovitis there is understandably a lack of validation for low-grade changes, such as those reported in the present study.13 It is also unlikely that these findings will be applied to the screening of asymptomatic patients with psoriasis given the prevalence of the latter and the lack of damage noted in the present study. However, if the findings can be replicated, they could provide a platform for the acceptance of a new model linking skin and joint disease in the psoriasis-related spectrum. Furthermore, the future addition of power Doppler imaging to study protocols could add additional useful information about subclinical entheseal associated vascular changes.14
WHAT IS IMAGING TELLING US ABOUT PSORIASIS AND THE PATHOGENESIS OF PSORIATIC ARTHRITIS?
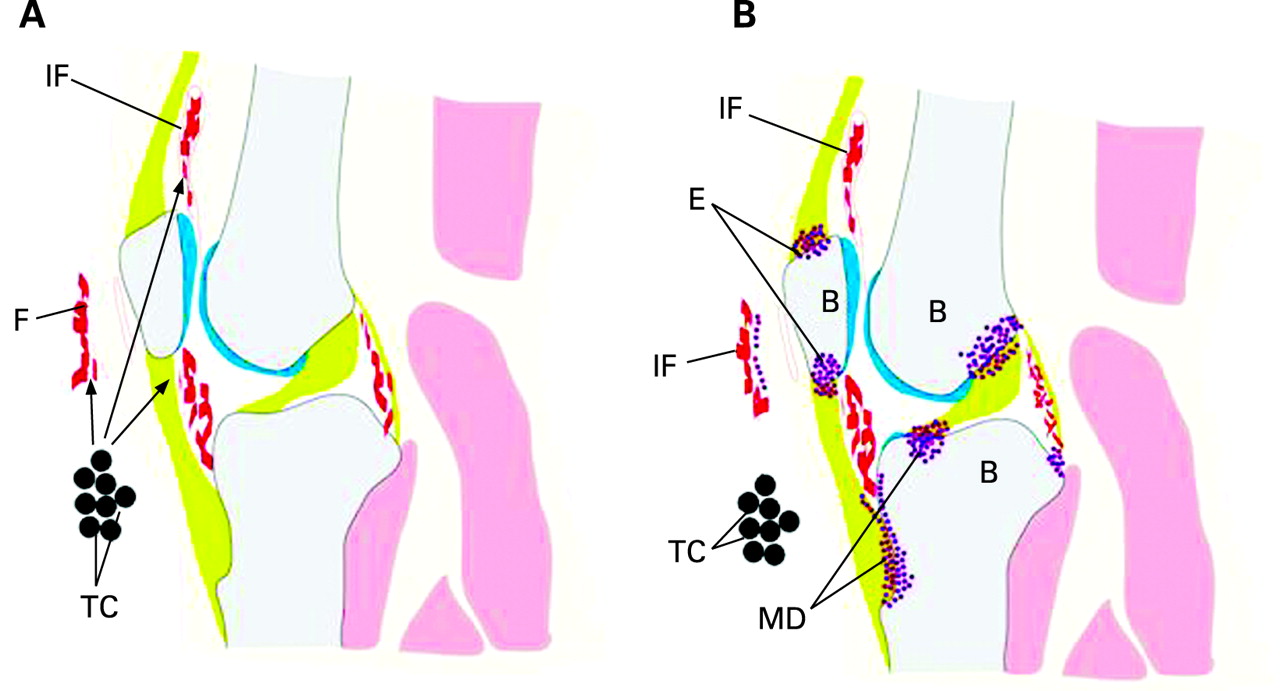
We feel that the accumulating imaging data, including that of the present study, increasingly suggest that the theories related to either autoimmunity directed against shared skin and synovial membrane antigens or some intrinsic angiogenic skin and synovial membrane perturbation, no longer adequately capture the essence of the disease (fig 1A). Indeed, imaging and pathogenesis studies such as the present one are supported by recent genetic studies challenging the MHC class 1 link with PsA.15 Because a prime feature of entheses is stress dissipation, and since even “normal” insertions are sites of microdamage, we think that “tissue specific factors” shared by the joint and skin are critical for disease expression (fig 1B).16
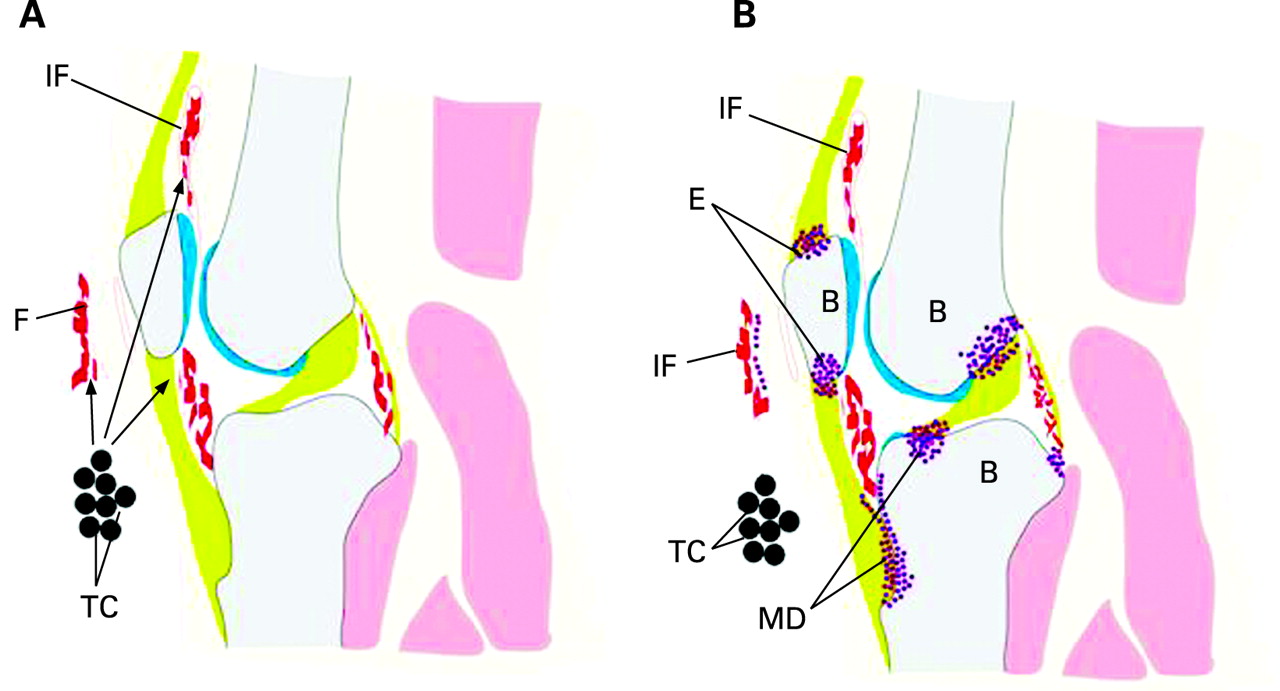
For the skin, a propensity for psoriasis is noted over extensor surfaces. It is also noteworthy that psoriasis can be induced in susceptible individuals by the mechanical effect of stripping sticky tape off the skin, which is thought to be related to tissue microdamage.17 With respect to the joint, an association between recalled joint injury and PsA, but not rheumatoid arthritis, is well reported.18 At the microscopic level we have recently shown that the normal enthesis is a structure that may be riddled with microdamage and tissue repair responses.9 19 It is possible that dysregulation of key molecular pathways at these “interface tissues” could trigger innate immune activation.20 This scenario is supported by emerging genetic studies in both psoriasis and PsA where pivotal innate immune cytokine polymorphisms have been reported.21 Given the predisposition of entheses to microdamage and the present findings in psoriatic patients, we believe that the time has now come to explore the molecular basis for this altered biomechanical response to joint stressing (fig 1B).
SHARED MICROANATOMICAL SIMILARITIES BETWEEN THE SKIN AND AN ENTHESIS
Some important microanatomical considerations must be considered both by dermatologists and by rheumatologists with respect to a comparison between the structure of the skin and that of a fibrocartilaginous enthesis. Both share the common feature of integration between two different types of tissues: for the skin it is the epidermis and dermis, and for the enthesis it is the bone and fibrocartilage of the tendon or ligament (fig 2). At either site (skin or enthesis), the mechanical properties of the two integrated tissues differ considerably and this leads to stress concentration at the tissue interfaces. At both sites, stress concentration is dissipated and tissue union promoted by increasing the surface area of contact between the tissues (fig 1). This increases the resistance to shear. It is also important to note that the epidermis and the healthy enthesis fibrocartilage are avascular, but the dermis and the bone are both highly vascular. In both cases, blood vessels get as close to the avascular tissue as possible. In the skin, the vessels form a plexus in the papillary layer (the rete subpapillare) and in enthesis, exchange vessels are abundant in the subchondral bone marrow.

{kind=link}
{kind=link}
One could even consider that the tidemark at an enthesis (that marks the outer limit of calcification and thus separates two tissues of very different physical properties) has something of a counterpart in the abrupt interface that exists at the level of the stratum lucidum/granulosum between living and dead cells in the epidermis. Here, too, there must be an abrupt change in mechanical properties. A remarkable feature of reactive arthritis is a rash on the soles of the feet (keratoderma blenorrhagicum) that is histologically identical to psoriasis.22 The biomechanical similarities of weight-bearing thick skin to the enthesis provide a novel way of thinking about this condition.
In view of the breadth of similarity between the skin and entheses, it is worth remembering that the epidermis and the dermal papillary layer function as a unit in psoriasis. Whether the subchondral plate and enthesis fibrocartilage behave as a similar “unit” in spondyloarthropathy is not clear, but the strong association between enthesitis and adjacent osteitis perhaps suggests that this is now worthy of consideration.23
CONCLUSION
To summarise, the study of Gisondi et al in the current issue of Annals of the Rheumatic Diseases emphasises yet again how imaging has the potential to transform our understanding of psoriasis and PsA. Given that psoriasis and PsA represent inflammation at two different target tissues that cannot be explained adequately by traditional autoantibody and autoimmune paradigms, studies such as the present one have implications for diseases that manifest at two or more different locations. Estimates as to the prevalence of PsA in subjects with psoriasis vary greatly, ranging from 6% to 39%.24 Approaches such as those used by Gisondi et al could certainly address this from the epidemiological perspective and shed further light on both psoriasis and PsA.
REFERENCES
Footnotes
-
Competing interests: None declared