Article Text

Abstract
Mycobacterium xenopi is a water-related mycobacterium with low pathogenicity in humans. Little is known about the association between anti-tumour necrosis factor (TNF)α and non-tuberculous mycobacterial infections. The case history is presented of fatal M xenopi infection in a patient receiving anti-TNFα treatment.
- TNFα, tumour necrosis factor α
Statistics from Altmetric.com
Mycobacterium xenopi is a water-related mycobacterium with low pathogenicity in humans. Although the association between anti-tumour necrosis factor (TNF)α treatment and Mycobacterium tuberculosis is well known,1,2 relatively little is known about the association with non-tuberculous mycobacterial infections. We present the first case of fatal M xenopi infection in a patient receiving anti-TNFα treatment.
CASE REPORT
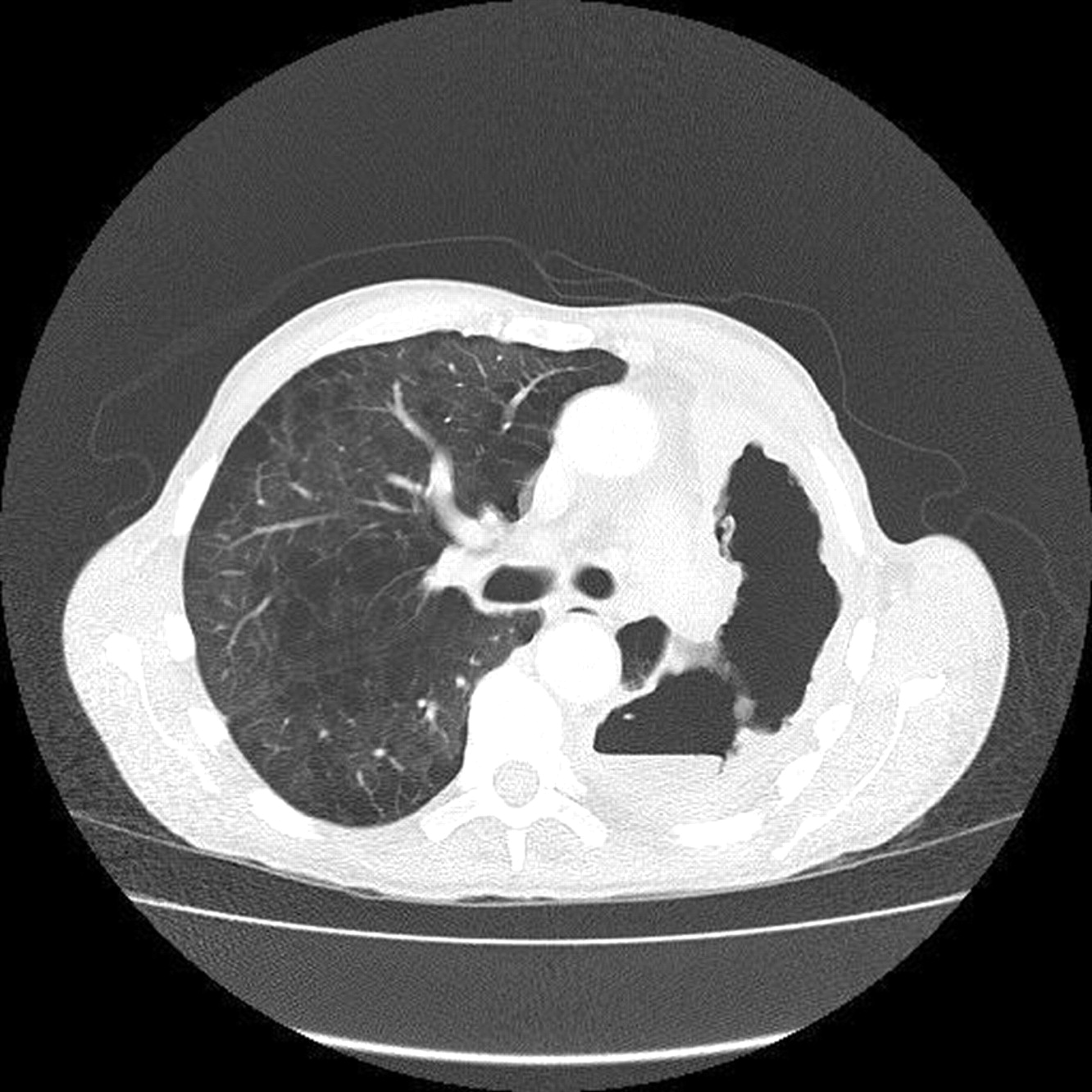
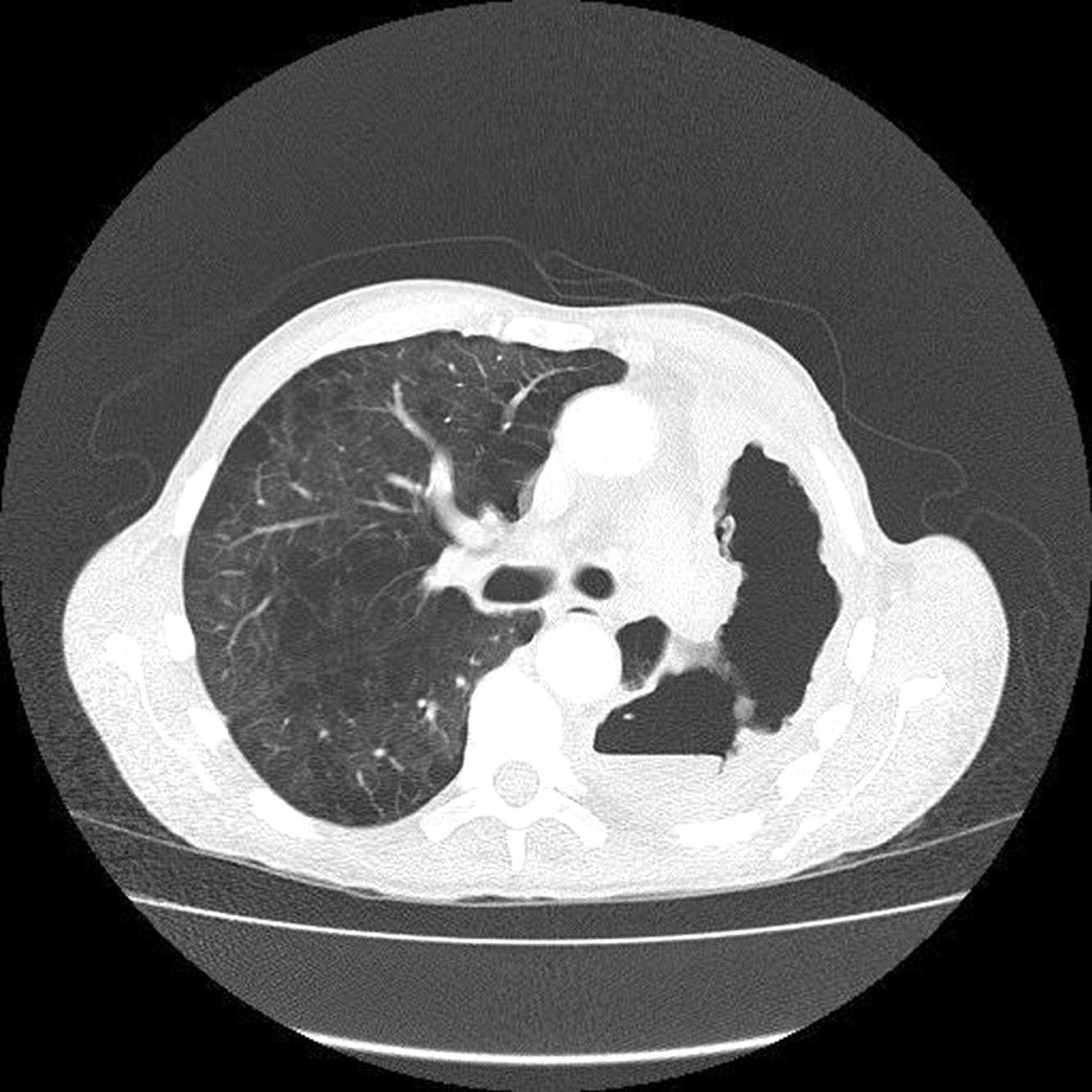
A 71-year-old Caucasian man was admitted to our institution in 2005 with progressive dyspnoea and weight loss over the preceding 12 months. He had moderate to severe emphysema and severe rheumatoid arthritis, previously well controlled with methotrexate and prednisone. In 2002 he experienced an acute exacerbation of the rheumatoid arthritis and the TNFα receptor antagonist etanercept was started. He had a complete response to the new medication and no side effects were noted. However, less than 12 months later he was admitted to another hospital with increasing dyspnoea, productive cough and weight loss. A chest radiograph revealed a new left upper lobe consolidation and macrolide treatment was initiated. After 2 weeks with an incomplete response he underwent bronchoscopy which yielded negative bacteriological assessment, negative acid-fast stain and mycobacterial cultures. However, sputum collected before starting treatment grew M xenopi. He improved after a few weeks of macrolide monotherapy and about 18 months later, after 12 months of progressive dyspnoea and weight loss, he was referred to our centre for further assessment. A CT scan (fig 1) revealed extensive emphysema in the right lung and near complete destruction of the left lung with air-liquid levels.
{kind=link}
CT scan showing extensive emphysema in the right lung and near complete destruction of the left lung with air-liquid levels.
Bronchoscopic examination was positive for M xenopi only. Treatment with rifampicin, ethambutol and clarithromycin was initiated and immunosuppressive medications for rheumatoid arthritis (including etanercept) were discontinued. Unfortunately the patient was unable to tolerate the initial antimycobacterial drug regimen and also refused parenteral aminoglycoside therapy. Over the subsequent 9 months he tolerated only intermittent single agent therapy and continued to deteriorate. He was admitted to his regional hospital for palliative inpatient care and died from respiratory failure and wasting illness.
DISCUSSION
Etanercept is a genetically engineered dimer of the soluble TNFα receptor II in which the extracellular domain of the p75 receptor has been fused to the Fc portion of IgG1. This agent has been used effectively in a variety of rheumatological diseases.3 Treatment with etanercept in short-term clinical trials has been reported to be well tolerated, but post-marketing surveillance has identified serious infectious side effects. TNFα has been shown to play a central role in the formation and maintenance of granulomas that contain and kill mycobacteria. It also appears to reduce tissue damage caused by the inflammatory response.4 Cases of reactivation of tuberculosis associated with the use of TNFα antagonists have led to a requirement for patients to be screened for active and latent tuberculosis before anti-TNFα treatment is given.
Mycobacterium xenopi is a water-related mycobacterium with low pathogenicity. Because of increased frequency of isolation of this organism and the relative infrequency of advanced infection, caution is advised in interpreting the clinical significance of M xenopi isolation.5 In our case, the diagnosis was established by repeated isolation of M xenopi in the setting of severe progressive systemic and pulmonary disease and in the absence of other pathogens. In view of our patient’s unsuccessful clinical course, it is suggested that a thorough pulmonary assessment should be performed before introducing etanercept or other anti-TNFα medication. In the presence of underlying lung disease such as emphysema, bronchiectasis or fibrosis, or in the presence of radiographic signs of current or prior pulmonary infection, assessment should include respiratory cultures for mycobacteria and fungi. Positive cultures for non-tuberculous mycobacteria mandate either pre-emptive treatment or close monitoring for progression if TNFα inhibition is initiated. A decision as to whether a patient with pulmonary non-tuberculous mycobacteria requires antimycobacterial treatment before receiving a TNFα inhibitor may be difficult and should involve clinicians with expertise in mycobacterial infection.
Footnotes
-
NM is supported by the Princess Margaret Hospital Foundation, Toronto, Canada and SACTA-RASHI Foundation, Israel.
-
Competing interests: None.