Article Text

Abstract
Objective: This study investigates parameters that could predict subclinical cardiac dysfunction in systemic lupus erythematosus (SLE) in the absence of valvular, clinical coronary artery and pericardial disease.
Design: A case-control trial.
Setting: Rheumatology clinic, a university teaching hospital.
Patients: Eighty-two female SLE patients (49 (SD 9) years) and 82 female normal subjects (49 (13) years) matched for age, body mass index, blood pressure and heart rate.
Interventions: All underwent standard echocardiography and tissue Doppler imaging.
Main outcome measures: Twenty-two (27%) patients had evidence of impaired left ventricular (LV) long-axis function with mean myocardial peak systolic velocity (Sm) of basal six segments <4.4 cm/s and also subnormal stress-corrected midwall fractional shortening. Thirty-four (42%) patients demonstrated impaired right ventricular (RV) long-axis function. These occurred in the presence of comparable normal LV ejection fraction, cardiac index, and RV fractional area change to the control group. Patients with subnormal mean Sm were older (49 (8) vs 44 (9); p = 0.043) and had a higher prevalence of hypertension (46% vs 22%; p = 0.034), longer disease duration >10 years (82% vs 50%, p = 0.01), higher disease activity score (73% vs 48% for Systemic Lupus Erythematosus Disease Activity Index (SLEDAI)⩾1, p = 0.049) and end-organ damage index (64% vs 47% with Systemic Lupus International Collaborating Clinics Damage Index (SLICC)⩾1, p = 0.049) than those with normal values. Disease duration >10 years, disease activity index and increased arterial stiffness provided additional incremental predictive value of LV long-axis function.
Conclusion: SLE patients have subclinical long and short-axis dysfunctions. Regular monitoring of cardiac function by tissue Doppler echocardiography may be indicated for patients who had SLE for >10 years, frequent flare or when arterial stiffening is demonstrated.
Statistics from Altmetric.com
Cardiovascular events are the most common single cause of death in systemic lupus erythematosus (SLE).1 Increased and subnormal left ventricular (LV) ejection fractions, impaired diastolic filling and increased LV mass have been reported in SLE patients.2–7 As clinically overt myocarditis is nowadays uncommon with corticosteroid therapy, such geometrical and functional changes may be due to underlying increased inflammation-mediated subclinical vasculitis, myocarditis or vascular stiffening, in addition to traditional risk factors, including premature subclinical atherosclerosis, established coronary artery disease, valvular heart disease, hypertension or renal disease. Preclinical detection of LV dysfunction in these patients is therefore important, as there may be a possible indication of early therapeutic intervention to attenuate the inflammatory process to control the disease and reduce arterial stiffening. Tissue Doppler echocardiography is a sensitive echocardiographic technique for quantitative assessment of subclinical myocardial dysfunction.8–10 Previous studies had demonstrated its clinical utility in providing prognostic information, incremental to clinical data and standard echocardiographic variables, for risk stratification of hypertensive patients under treatment and also in patients with a variety of cardiovascular diseases and LV systolic function.11–14 However, it remains uncertain whether the early LV dysfunction in SLE is disease-related or a result of other predisposing conditions. We hypothesised that early impairment of LV systolic function would be more prevalent in those with active inflammation and might be related to duration of the disease.
Thus, we performed a case-controlled study to evaluate various clinical and disease markers (serological indicators and inflammatory mediators) of SLE that are associated with preclinical LV systolic dysfunction as detected by tissue Doppler-derived myocardial velocity. Of note, we specifically excluded SLE patients with clinical or echocardiographic evidence of significant valvular, coronary or pericardial heart disease to eliminate confounding variables of earlier studies.3 4
METHODS
Study design
A total of 82 female SLE patients were enrolled from the rheumatology clinic of a teaching hospital between May 2005 and July 2007. All patients fulfilled the 1997 American College of Rheumatology (ACR) revised diagnostic criteria.15 They were matched to 82 control subjects on the basis of age, gender, body mass index, blood pressure, heart rate, LV ejection fraction and RV fractional area change. All the patients had a normal LVEF of >50%. Exclusion criteria included pregnancy, those with history or symptoms of heart failure or myocarditis, evidence of clinical coronary artery or pericardial disease, atrial fibrillation and echocardiographic evidence of segmental wall motion abnormalities or greater than mild aortic or mitral valve disease. Comprehensive medical histories of SLE patients were obtained via interviews and chart reviews. Disease activity and disease-related damage were assessed with the use of the Systemic Lupus Erythematosus Disease Activity Index (SLEDAI)16 and the Systemic Lupus International Collaborating Clinics Damage Index (SLICC)17 respectively. In brief, SLEDAI includes 24 items commonly contributing to disease activity present within 10 days of the evaluation, and a score of 0 is regarded as disease in remission. SLICC includes 12 descriptors of organ damage including renal involvement, diabetes, pulmonary hypertension and ischaemic heart disease. Glomerular filtration rate (eGFR) in ml/min per 1.73 m2 was estimated by the Modification of Diet in Renal Disease (MDRD) formula for females of Chinese origin = 186.3×serum creatinine (mg/dl)−1.154×age−0.203×0.742×1.233).18 Medication records were obtained that included use of prednisolone, azathioprine, cyclophosphamide and methotrexate. Serological markers of SLE, including inflammatory mediators and specific antibodies, were obtained using standardised laboratory assays. The Ethics Committee of the Chinese University of Hong Kong approved this study, which was conducted in compliance with the Declaration of Helsinki (2000) of the World Medical Association, and all patients provided written informed consent.
Echocardiographic study
Comprehensive echocardiography was performed by three experienced research technicians using standard techniques on a Vivid 7 system with a 3.5 MHz probe (GE Medical Systems, Milwaukee, Wisconsin), and interpreted by a single cardiologist who was unaware of the clinical characteristics of the patients and referent subjects. Conventional echocardiographic parameters were measured according to American Society of Echocardiography (ASE) recommendations.19 Additional off-plane images of the right ventricle were obtained to maximise the visualisation of RV morphology. The LV ejection fraction was calculated by the modified biplane Simpson method from apical four- and two-chamber views. Stroke volume was calculated from the difference between LV end-diastolic volume and end-systolic volume derived from the Simpson method, and was used to calculate cardiac index (stroke volume×heart rate cardiac output/body surface area). Endocardial fractional shortening (FS) was calculated as the LV dimension difference between the end-diastole and end-systole divided by the LV end-diastolic dimension. Midwall fractional shortening was calculated from the following formula: MWFS = ([LVIDd+SWTd/2+PWTd/2]−[LVIDs+inner shell])/(LVIDd+SWTd/2+PWTd/2), where inner shell = [(LVIDd+SWTd/2+PWTd/2)3−LVIDd3+LVIDs3]1/3−LVIDs with LVID as the LV dimension, SWT as the septal wall thickness, PWT as the posterior wall thickness, s as in end-systole and d in end-diastole. LV meridional and circumferential end-systolic systolic stress were estimated using the following formulae: mESS = (0.334×SBP×LVIDs)/(PWTs×[1+PWTs/LVIDs]) and cESS = [(SBP×[LVIDs/2]2)×{1+[LVIDs/2+PWTs]2/(LVIDs/2+PWTs/2)2}]/(LVIDs/2+PWTs)2−(LVIDs/2)2, where SBP is the brachial cuff systolic blood pressure.20 21 Both FS and MWFS were corrected for mESS and cESS respectively (stress-corrected FS or MWFS) to give load-independent measures of LV systolic performance.22
Pulmonary arterial systolic pressure (PASP) was estimated by Doppler echocardiography from the systolic transtricuspid pressure gradient (in mm Hg), using the simplified Bernoulli equation and adding estimated right atrial pressure based on the size of the inferior vena cava and its variation with breathing. The RV free wall thickness was measured from the subcostal view at the peak of the ECG R wave at the level of the tricuspid valve chordae tendinae. The RV fractional area change was calculated by contouring the end-systolic and end-diastolic images of the right ventricle in the four-chamber view and by using the formula (end-diastolic area–end-systolic area)/end-diastolic area.19
Real-time pulsed-wave tissue Doppler peak systolic velocities (S′) were recorded from the septal and lateral sites of the mitral annulus and the lateral tricuspid annulus in the apical four-chamber view. Images in at least three consecutive beats were stored and analysed using off-line analysis programs (EchoPac-PC 6.1.0). Peak mean systolic myocardial velocities based on colour tissue Doppler were measured offline from six basal and six mid segments of the LV taken from apical views (apical four-chamber, two-chamber and long-axis),10 and basal and mid segments of the RV free wall from apical four-chamber view for assessment of global ventricular function. Care was taken to place the Doppler sample within the myocardium of each segment throughout the cardiac cycle. We used the mean Sm from six basal LV segments of <4.4 cm/s and pulsed-wave Doppler systolic velocity of lateral tricuspid annulus <11.5 cm/s to define subclinical LV and RV systolic dysfunction respectively.10 23 In our laboratory, the intraobserver and interobserver variability for tissue Doppler velocity data were 3% and 5% respectively as previously reported.10 24
Determination of vascular function
Total arterial compliance was estimated by the SV-to-pulse-pressure ratio and systemic vascular resistance index by mean brachial cuff pressure [diastolic blood pressure+(pulse pressure/3)] divided by cardiac index×80.25
Statistical analyses
Comparisons between SLE patients and referent subjects and between patients with and without longitudinal LV systolic dysfunction (using a cutoff value of 6-basal segment mean Sm <4.4 cm/s) were made using two-sample t tests for continuous variables and by χ2 analysis for categorical variables. Results of continuous variables are presented as mean (SD) unless otherwise stated. Univariate logistic regression models were used to assess the relation of significant clinical comorbidities, and echocardiographic Doppler variables to the presence of subclinical LV systolic dysfunction (mean six basal segmental Sm<4.4 cm/s). All variables that had a significant association but did not exhibit excessive collinearity with each other were evaluated for inclusion in a model predicting mean Sm<4.4 cm/s using multivariable regression analysis; odd ratios (OR) with their 95% confidence intervals were reported. Statistical analysis was performed using dedicated software (SPSS 13.0, SPSS, Chicago). Two-sided values of p<0.05 were considered statistically significant. The authors had full access to and took responsibility for the integrity of the data. All authors read and agreed to the manuscript as written.
RESULTS
Clinical characteristics of SLE patients
The mean disease duration was 11.8 (SD 6.0) years with 48 patients (59%) suffering more than 10 years. There were 51 patients (62%) with nephritis, 23 (28%) with hypertension, 21 (26%) with history of vasculitis, four (5%) with cerebrovascular disease and two (2%) with diabetes mellitus. Forty-five patients (55%) had active disease identified by SLEDAI ⩾1 (median 1; range 0–10), and organ damage with SLICC ⩾1 (median 1; range 0–5). There were no current smokers in our patients. Anti-DNA antibodies were present in 43 patients (51%) and antiphospholipid antibodies in 11 patients (13%). For medications, current or former use of prednisone was present in 62 patients (76%), whereas other immunosuppressive therapy was less common (azathioprine in 41%, ciclosporin A in 13%, cyclophosphamide in15%). Hydroxychloroquine had been used in 47 patients (57%). Antihypertensive therapy included angiotensin-converting enzyme inhibitors/angiotensin receptor blockers in 23%, beta-blockers in 15% and diuretics in 7% of patients.
Comparison of conventional echocardiographic parameters between SLE and control groups
There was no difference in age, blood pressure and heart rate between the patient group and normal controls. For conventional echocardiographic parameters of LV systolic function, all the SLE patients had a normal ejection fraction of >50% (mean of 67.9 (5.8)%). The LV volume, LVEF, stroke volume and cardiac index were not different between the patient and control groups (table 1). However, there was evidence of an increase in LV mass and LV wall thickness in the SLE group. For RV systolic function, despite a higher PASP in the patient group, there was no difference in RV fractional area shortening. The RV free wall thickness was increased in the patient group (table 1).
Comparison of tissue Doppler parameters of ventricular systolic function and vascular parameters between SLE and control groups
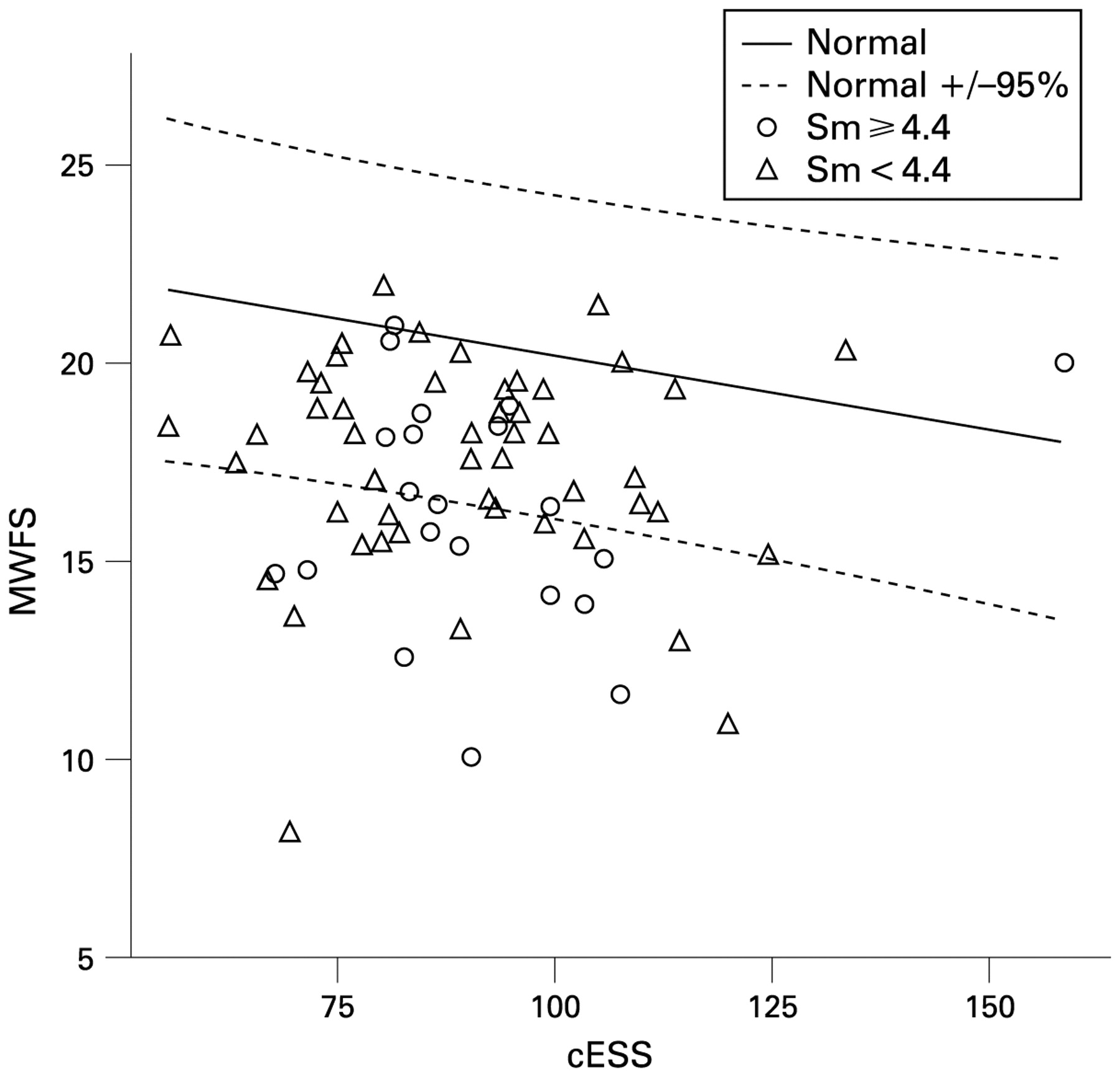
Despite similar LVEF and other parameters of systolic function, SLE patients exhibited impaired LV longitudinal and short-axis systolic function with a reduction in the mean Sm of six basal segments or 12 LV segments, MWFS and stress-corrected MWFS. A cut-off value of mean Sm from six basal LV segments <4.4 cm/s has been validated previously to define systolic long-axis dysfunction.13 Thus, the prevalence of subclinical systolic longitudinal dysfunction in SLE patients was 27% (22 patients) in that they also demonstrated impaired short-axis function with depressed stress-corrected MWFS when compared with the normal subjects (0.18 (0.04) vs 0.22 (0.04) cm2/kdyne·10−2; p<0.05), as illustrated in fig 1.

{kind=link}
Stress-shortening relationships in systemic lupus erythematosus (SLE) patients with preserved and depressed long-axis function. Midwall fractional shortening (MWFS) is plotted against circumferential end-systolic wall stress (cESS; an index of myocardial contractility). Data from SLE patients are plotted with reference to the mean±95% prediction interval for normal controls. Sm, mean myocardial systolic peak velocity.
For RV systolic function, there was significant reduction in mean Sm of RV free wall as well as reduction in S′ at the tricuspid annulus (table 1). Vascular assessment showed an increase in systemic vascular resistance index in SLE patients when compared with the controls (table 1).
Comparison of SLE subgroups with and without subclincial LV systolic dysfunction by tissue Doppler imaging
Table 2 compared the clinical characteristics of SLE patients with normal and subnormal LV systolic function based on tissue Doppler evidence of reduced mean Sm of six basal LV segments. Patients with subnormal mean Sm were older (49 (8) vs 44 (9); p = 0.043), had higher systolic, mean and pulse pressures, a higher prevalence of hypertension (46% vs 22%; p = 0.034), a greater proportion suffering with longer disease duration >10 years (82% vs 50%, p = 0.01) and a higher disease activity score (76% vs 51% for SLEDAI ⩾1, p = 0.045) and end-organ damage index (64% vs 47% with SLICC ⩾1, p = 0.049) than those with normal mean Sm. There were no differences in other clinical features, including estimated GFR, blood tests for immunological markers, serum biochemistry, lipid profile and cell counts as well as medications between the two SLE subgroups (table 2).
For comparison of echocardiographic variables between SLE subgroups with normal and subnormal LV systolic function by tissue Doppler imaging (TDI), almost all the conventional parameters failed to show any difference except a significantly greater LV posterior wall thickness in the latter group. However, the S′ at both the septal and lateral mitral annulus were further reduced in those with subnormal LV systolic function. Furthermore, parameters of RV systolic function were similar including S′ at tricuspid annulus and Sm at RV free wall, though the RV wall thickness was increased in patients with subclinical LV systolic dysfunction (table 3). Interestingly, the mean early LV diastolic velocity based on six basal or 12 (6-basal, 6-mid) segments decreased further from preserved to depressed longitudinal function, despite the fact that LV diastolic patterns were similar in both SLE subgroups. For vascular parameters, patients with a subnormal LV systolic function had a higher systemic vascular resistance index (p = 0.022) but lower total arterial compliance (p = 0.007) than the control group (table 2).
Predictors of subclinical LV systolic dysfunction
Table 4 outlines all the significant covariates that predicted subclinical LV systolic dysfunction (mean Sm of six basal segments <4.4 cm/s) in a univariate followed by multivariate analysis models. In the univariate model, significant covariates included age, hypertension, disease duration >10 years, SLEDAI⩾1, SLICC ⩾1, LV mass index, stress-corrected MWFS and fractional shortening, systemic vascular resistance index as well as total arterial compliance. In multivariable regression analysis, independent predictors of LV systolic dysfunction included disease duration >10 years (OR = 5.49; 95% CI 1.41 to 21.34, p = 0.014), SLEDAI⩾1 (OR = 4.92; 95% CI 1.28 to 28.86, p = 0.02), and total arterial compliance (OR = 0.04; 95% CI 0.003 to 0.41, p = 0.007) (table 4). The stepwise addition of all three independent covariates also provided incremental predictive values for abnormal LV long-axis systolic function (χ2 for disease duration >10 years = 6.1, χ2 for disease duration >10 years and SLEDAI = 10.7, and that for disease duration >10 years, SLEDAI and TAC = 20.1).
DISCUSSION
To our knowledge, this is the first study to confirm the hypothesis of the presence of subclinical LV systolic dysfunction in SLE patients with relatively mild disease and organ. Not only had 27% SLE patients evidence of impaired LV long-axis function and depressed circumferential stress-corrected midwall shortening, but also 42% demonstrated impaired RV long-axis function. These occurred in the presence of normal LV ejection fraction, cardiac index and right ventricular fractional area change. Of note, the mean LV early diastolic velocity was significantly decreased in those with impaired LV longitudinal systolic function than those without, even though they have comparable severity of diastolic dysfunction. We further explored independent predictors of LV systolic dysfunction, which included a long disease duration of >10 years, a high disease activity index ⩾1 and increased arterial stiffness. In addition, assessment of these factors provided incremental predictive value in a stepwise manner.
Subclinical left ventricular systolic dysfunction in SLE patients
This study revealed that both subclinical long and short-axis LV dysfunctions can occur in SLE patients with predominantly mild disease and organ damage despite normal LVEF. We employed TDI to examine comprehensively the long-axis function in all the basal LV walls, as long-axis function has been shown to be the major axis of myocardial function26 and is sensitive to myocardial ischaemia, hypertension and LV hypertrophy. Furthermore, TDI velocities have been shown to be a sensitive tool in detecting early myocardial dysfunction before the occurrence of reduced LVEF or in situation where the compensatory circumferential fibre contraction may maintain an apparently normal LVEF.8–10 27 28 The validity of using mean value of the six basal LV segments (mean Sm) <4.4 cm/s to represent preserved global LV systolic function (LV ejection fraction ⩾50%) was based on our previous study of 106 normal control subjects. This cut-off value was derived from offline colour TDI images that represented −2SD of mean myocardial velocities. The use of 2D colour-coded TDI images has the advantage of providing a faster way of assessing cardiac function than pulsed-wave TDI and could be performed offline and in a blinded fashion. It is important to realise that myocardial velocities obtained from the online pulsed TDI curve are about 20% higher than those reconstructed offline from 2D colour-coded TDI images.29
Previously, low midwall LV performance was observed in about one-sixth of hypertensive adults in a population-based study. In this study, this was about one-quarter, but the values were not different between normal and subnormal long-axis SLE subgroups. Calculation of the circumferential stress-corrected MWFS is particularly useful in revealing underlying systolic dysfunction in hypertrophic hearts with normal shortening at the endocardium and no evidence of heart failure.21 30 Interestingly, early diastolic myocardial velocity based on basal six segments of the LV was also depressed in SLE patients with impaired systolic longitudinal function, even though there was no difference in diastolic grading between the SLE subgroups. The long- and short-axis changes may reflect the underlying hypertension but more importantly the increased LV mass index that SLE predicts independent of traditional risk factors including hypertension.7
We also observed the RV systolic dysfunction in SLE patients despite a normal RV fractional area change of >45%. Interestingly, it appears that the RV systolic dysfunction does not predict the occurrence of LV systolic dysfunction. Gin et al found that S′ at the tricuspid free wall annulus decreased with increasing PASP in a cohort of 40 SLE patients.31
Predictors of subclinical LV systolic dysfunction in SLE
We also sought to determine potential predictors of subclinical LV systolic dysfunction in the current study. Independent predictors included a prolonged disease duration of >10 years, SLE Disease Activity Index score ⩾1 and reduced total arterial compliance. Therefore, it appears that the chronicity of disease, in particular when combined with SLE disease flare, will result in more significant damage of the LV systolic function. Arterial stiffness was recently shown to be increased in SLE, which was related to disease duration and severity of vascular inflammation as reflected by circulating inflammatory markers.32 This finding was consistent with the observation that systolic myocardial velocity varies with arterial loading.25 Therefore, stiffness of the arterial wall in SLE is likely associated with vascular inflammation and atherosclerosis, which may play a contributory role to early impairment of LV contractility. Furthermore, patients with depressed long-axis function also had depressed stress-corrected MWFS, a load-independent measure of short-axis function, indicating that a substantial percentage of SLE patients have a true decrease in LV contractility.
Limitations
This was an observational study, and we have not adjusted for the multiple comparisons of various end-points, which may have inflated our alpha error. We chose hypertension instead of systolic, mean or pulse pressure in the multivariate analysis because blood pressures can be variable for hypertension under treatment. Hypertension selected as one of the univariate factors would take into account both optimally and suboptimally controlled hypertensive SLE patients. Furthermore, blood pressures interact with total arterial compliance that might better reflect the afterload as it is corrected by stroke volume. The inclusion of SLE patients suffering from stage 4 chronic kidney disease (estimated GFR<30 ml/min/1.73 m2) reflected the prospective nature of our patient recruitment. Moreover, the degree and prevalence of chronic renal impairment were equal in the two SLE subgroups that would normalise its impact on the myocardium and peripheral vasculature. Inclusion or exclusion of these five patients will not affect our overall results but rather strengthen generalisation of these data and clinical findings. Whether the same clinical predictors of subclinical LV systolic dysfunction can be applied to SLE patients with more active disease and organ damage will require further study. However, this incremental model of predicting subclinical LV systolic dysfunction confirms and extends existing knowledge of LV structural and functional abnormalities in SLE in the absence of valvular, clinical coronary artery and pericardial disease.
Implications of the study
This is the first study to demonstrate the presence of subclinical LV systolic dysfunction even when LVEF appears to be normal. It also revealed potential predictors of such a condition. Our findings call for regular careful clinical assessment plus the use of appropriate investigation to identify early impairment of LV systolic function. In addition, these data may support prompt and aggressive treatment to prevent or alleviate SLE disease flare, and further studies on the development of therapeutic strategies in SLE patients with subclinical systolic dysfunction. Finally, regular monitoring of cardiac function by TDI may be advisable for patients who had SLE for >10 years, frequent flare or when arterial stiffening is demonstrated.
REFERENCES
Footnotes
Funding: The work by GW-KY and L-ST was jointly supported by a research grant from the Department of Medicine & Therapeutics, Chinese University of Hong Kong, China.
Competing interests: None.
Ethics approval: Ethics approval was provided by the Ethics Committee of the Chinese University of Hong Kong.
Patient consent: Obtained.