Article Text

Abstract
Objectives To compare the clinical characteristics, burden of disease (eg, disease activity, function, quality of life), treatment modalities and treatment effect in patients with radiographic and non-radiographic axial Spondyloarthritis (r-axSpA and nr-axSpA).
Methods A systematic literature review (2009–2018) was performed using the participants, intervention, comparator and outcomes methodology. Studies reporting outcomes (clinical presentation, burden of disease, treatment modalities and treatment effect) of both r-axSpA and nr-axSpA were included. A pooled analysis was performed (standardised means difference and relative risk for continuous and binary variables, respectively) and random or fixed effects methods were used depending on the heterogeneity of the studies.
Results 60 studies out of 787 references were included. Pooled analysis showed that, compared with patients with nr-axSpA, patients with r-axSpA were more frequently men (69.6% vs 53.6%), smokers (37.7% vs 31.1%) and had higher mean disease duration (8.6 vs 5.0 years) and longer time to diagnosis (6.1 vs 4.2 years). Peripheral manifestations were more prevalent in nr-axSpA, while uveitis and structural damage on MRI of the sacroiliac joints were more prevalent in r-axSpA. C-reactive protein and the Bath Ankylosing Spondylitis Mobility Index were higher in r-axSpA, while Bath Ankylosing Spondylitis Disease Activity Index, Bath Ankylosing Spondylitis Functional Index and Ankylosing Spondylitis Quality of Life were similar in both groups. No significant differences were found with regard to treatment effect.
Conclusions Patients with r-axSpA and nr-axSpA share a similar clinical presentation except for peripheral involvement, which is more prevalent among nr-axSpA. Except for a more impaired mobility in r-axSpA, both groups showed a comparable burden of disease, treatment modalities and treatment effect.
- axial Spondyloarthritis
- meta-analysis
- disease outcomes
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Non-radiographic axial Spondyloarthritis (nr-axSpA) has been classically considered as an early form of axial Spondyloarthritis (axSpA) that would eventually progress to radiographic forms (r-axSpA).
However, some authors suggest that r-axSpA and nr-axSpA might not necessarily be part of a continuum of the same disease reflecting different phenotypical presentations.
What does this study add?
The results of this meta-analysis reveal a similar clinical presentation in patients with r-axSpA and nr-axSpA, except for peripheral involvement, which seems more prevalent among nr-axSpA, and uveitis which seems more prevalent in r-axSpA.
Despite higher levels of inflammatory biomarkers and reduced spinal mobility found in the patients with r-axSpA, both r-axSpA and nr-axSpA groups presented with comparable patient-reported outcomes (Bath Ankylosing Spondylitis Disease Activity Index, global assessment and quality of life) as well as comparable response to treatment.
How might this impact on clinical practice?
The results of this meta-analysis confirm that r-axSpA and nr-axSpA share similar characteristics and burden of disease, supporting the concept of axSpA as one disease.
INTRODUCTION
Spondyloarthritis (SpA) is a chronic inflammatory rheumatic disease involving the axial skeleton (spine and sacroiliac joints (SIJ)), entheses and peripheral joints, and may occur together with extra-articular manifestations, such as psoriasis, inflammatory bowel disease (IBD) and uveitis.1
Classically, the cornerstone feature for axSpA classification was the structural damage of the SIJ, which led to the development of the modified New York criteria.2 In the late 1990s, the broad use of MRI in patients with axial pain revealed that imaging abnormalities (namely inflammatory lesions) of the SIJ could be observed in patients with axSpA even in the absence of structural damage of the SIJ. This fact led in 2009 to the development of the Assessment of SpondyloArthritis international Society (ASAS) classification criteria, to allow the classification (and thus, the inclusion in trials) of patients with axSpA without structural damage of the SIJ. The ASAS criteria capture both patients with structural damage of the SIJ (ie, patients with radiographic axSpA (r-axSpA)) but also patients without structural damage (ie, non-radiographic axSpA (nr-axSpA)).3 Nr-axSpA has been classically considered as an early form of axSpA that could—but not necessarily—progress to r-axSpA.4 Some studies have reported that only 10%–20% of patients with nr-axSpA develop structural damage in 2 years, and 30% of them seem to never progress to r-axSpA.4 5 Also, one of the aims of the ASAS criteria was to allow patients to be classified as ‘axSpA’, regardless of the presence of radiographic sacroiliitis, emphasising the concept of ‘axSpA’ as the disease, and ‘r-axSpA’ and ‘nr-axSpA’ as different groups within such disease. However, since the publication of the ASAS criteria, the similarities and differences of these two groups of patients (ie, r-axspA and nr-axSpA) have been questioned repeatedly and it has been suggested that nr-axSpA would present only a milder form of axSpA, with less disease burden. In fact, treatment with biological drugs is not indicated in nr-axSpA in many countries based on this belief. This is in disagreement with the authors’ clinical practice experience, where patients with axSpA with and without radiographic sacroiliitis seem to have a similar disease burden.
Several studies have reported clinical characteristics and burden of disease in patients with r-axSpA and nr-axSpA, but only one systematic literature review (SLR) compared their burden, reporting a similar burden in the two groups.6 However, no meta-analysis was performed, and several new studies have been published since. Prompted by all these factors, we decided to perform a SLR with a pooled analysis with the aim to compare the clinical presentation, burden of disease, treatment modalities and treatment effect in patients with r-axSpA and nr-axSpA.
Methods
Search methods and study selection
The search for this SLR was performed using PubMed, EMBASE and Cochrane Central databases, with a search strategy appropriately adapted for each database (online supplementary table 1). A university librarian was consulted to define the search string in each database, based on previously existing SLRs.6 7 Only full-text articles on human subjects, published in English and between January 2009 (date of publication of the ASAS criteria for axSpA) and October 2018, were included. The SLR was conducted in accordance with the Preferred Reporting Items for Systematic review and Meta-Analyses guideline.8
Supplemental material
The participants, intervention, comparator and outcomes approach was used to formulate the research questions: (a) participants: adult patients (age ≥18 years) classified as r-axSpA or ankylosing spondylitis; (b) intervention: any intervention, as well as no intervention; (c) comparator: adult patients (age ≥18 years) classified as nr-axSpA and (d) outcomes: clinical presentation, burden of disease (including disease activity, function, mobility, quality of life and work productivity), treatment modalities and treatment effect were included. The outcome ‘treatment effect’ was only considered in randomised controlled trials (RCTs) with a pharmacological intervention.
All observational studies (ie, cross-sectional, cohort and case control) and RCTs, including patients with r-axSpA as well as patients with nr-axSpA were eligible for inclusion. Meta-analyses were only used to identify the individual studies (in case they had not been captured by the search strategy) from which individual data were extracted.
Data extraction and assessment of risk of bias
First, title and abstract screening according to the predefined inclusion criteria was conducted on all citations identified. Second, a full article screening was conducted on all citations remaining after title and abstract screening and after duplicate removal. Both screenings were performed by two reviewers (CLM and AM) on a sample of 20% abstracts and articles: since they reached a 90% agreement, CLM continued the screening alone. Disagreements regarding the eligibility of the studies or data extraction were resolved by discussion and consensus. Risk of bias (RoB) was assessed for the main outcome in each study according to the ‘Cochrane tool’ for RCTs and ‘Hayden tool’ for observational studies.9 10
In the data extraction process (online supplementary table 2), study identifiers, study type (RCT or observational study), participants (definition of r-axSpA and nr-axSpA criteria and number of patients in each group) and the intervention were collected. Outcomes were divided into four categories: clinical presentation, burden of disease, treatment modalities and treatment effect. Clinical presentation included socio-demographic variables (age, gender, body mass index (BMI), ethnicity and smoking), disease features (age at symptom onset, Human Leukocyte Antigen B27 (HLA-B27) status, inflammatory back pain (IBP), non-steroidal anti-inflammatory drugs (NSAIDs) response, family history of SpA and peripheral and extra-rheumatological manifestations (uveitis, psoriasis and IBD), among others) and imaging, such as MRI sacroiliitis according to the ASAS definition,11 SpondyloArthritis Research Consortium of Canada (SPARCC) score on the SIJ and spine,12 13 the presence of erosions and fatty lesions on MRI-SIJ, modified Stoke Ankylosing Spondylitis Spinal Score (mSASSS)14 and the presence of syndesmophytes on the spine radiograph. Concerning the burden of disease, we collected data regarding: (a) disease activity (C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), Bath Ankylosing Spondylitis Disease Activity Index (BASDAI),15 Ankylosing Spondylitis Disease Activity Score using CRP (ASDAS-CRP),16 and patient and physician global assessments); (b) function (Bath Ankylosing Spondylitis Functional Index (BASFI)17 and Health Assessment Questionnaire (HAQ)18; (c) quality of life (SF-36 questionnaire)19; (d) mobility (by the use of the Bath Ankylosing Spondylitis Mobility Index (BASMI))20 and (e) work productivity (including days of sick leave and work loss, using the Work Productivity and Activity Impairment questionnaire (WPAI)),21 among others. Data concerning treatment modalities (NSAIDs, glucocorticoids, conventional synthetic disease-modifying anti-rheumatic drugs and biological disease-modifying anti-rheumatic drugs (bDMARDs) in both observational and RCTs studies were also collected. Finally, ‘treatment effect’ was only evaluated in RCTs: we extracted treatment response data available (ie, BASDAI, CRP, ASDAS, ASAS response criteria (ASAS20 and ASAS40),22 ASDAS clinically important improvement (∆≥1.1), ASDAS major improvement (∆≥2.0)23 and BASDAI50).
From manuscripts reporting results from a same study population or cohort, information on such population was only extracted once, and the same study could be used for the evaluation of one or more outcomes for the purpose of this SLR.
Data analysis
The number of studies and number of patients per study were extracted. Medians were converted to means to pool results in a consistent format following the method published by Luo et al.24 For continuous variables, a pooled comparison between r-axSpA and nr-axSpA was performed using the standardised mean difference (SMD), which expresses the distance between two group means. We considered SMD <0.2 as small, 0.2>SMD < 0.8 as medium and SMD >0.8 as large magnitude of difference.25 For binary variables, the relative risk (RR) (probability of an event occurring in r-axSpA vs the probability of the event in nr-axSpA) was calculated. SMD and RR were estimated using fixed (I2 <50%) or random (I2 ≥50%) effects depending on the heterogeneity of the studies.
R-Cran V.3.5.1 software and the package ‘meta’ was used for the statistical analysis.26
Results
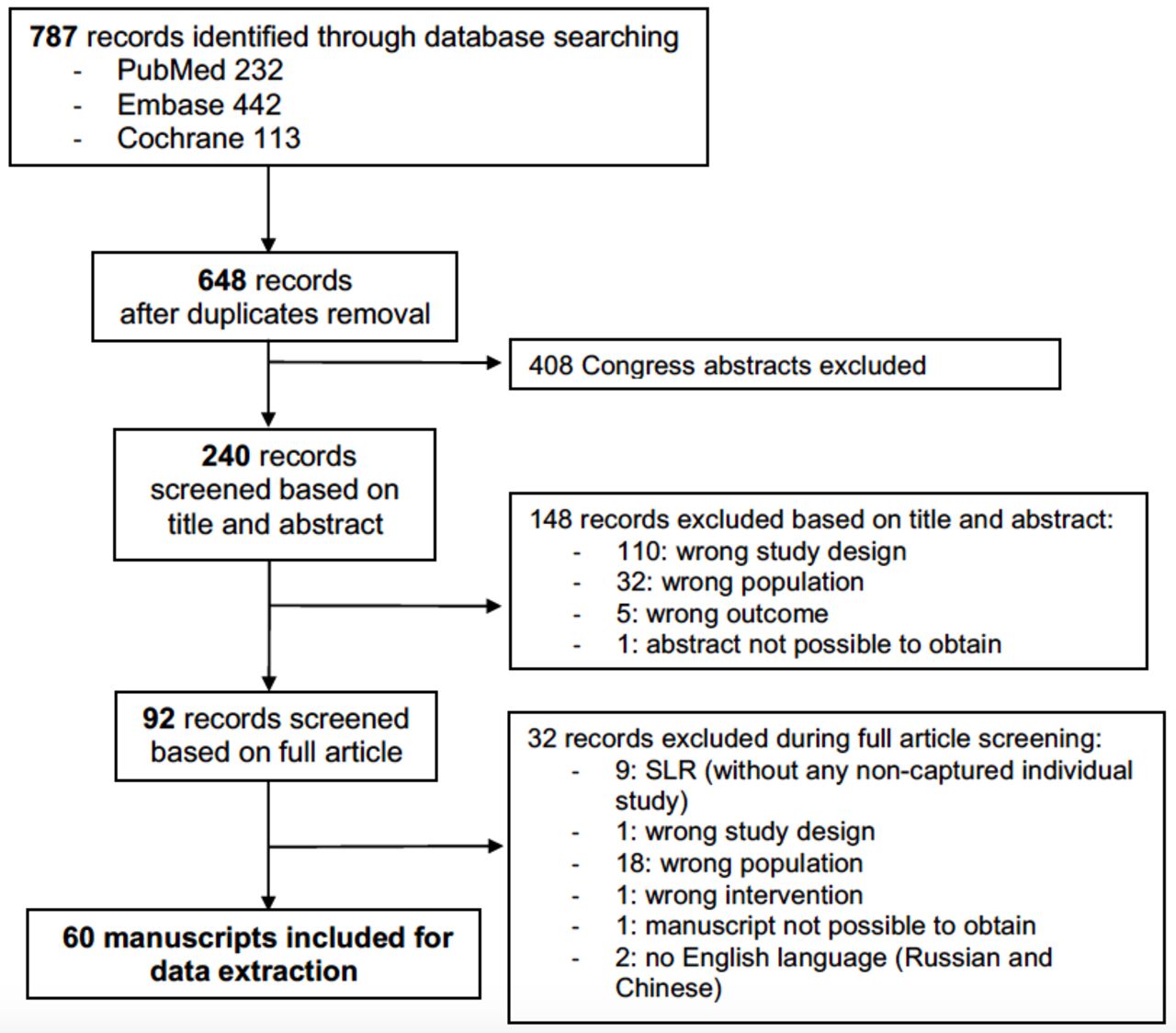
A total of 787 references were identified with the search strategy (232 in PubMed, 442 in EMBASE and 113 in Cochrane) (figure 1). After removal of duplicates and congress abstracts, 240 references were screened based on title and abstract, leading to 92 references to be screened based on full articles. Finally, 60 full-text articles were included in the SLR for data extraction (online supplementary table S3 and list of references). Regarding the study design, 10 (16.4%) were RCTs, 12 (20.0%) cohort studies, 36 (60.0%) cross-sectional studies and 2 (3.3%) had a case–control design (table 1). Clinical presentation, burden of disease (disease activity, function, mobility and quality of life), treatment modalities and treatment effect were evaluated in 54, 44, 19 and 9 manuscripts, respectively. A total of 14 manuscripts (23.3%) reported at least one variable as median. No manuscript showed a high RoB regarding the main outcome (table 1 and online supplementary table S3).

{kind=link}
Flowchart summarising the number of records at each step.
Summary of studies included for data extraction
Clinical presentation
The results from the pooled analysis of clinical presentation variables are presented in table 2. We found medium differences (0.2>SMD < 0.8) between r-axSpA and nr-axSpA with regard to disease duration (8.6 vs 5.0 years for r-axSpA vs nr-axSpA, SMD 0.55; 95% CI: 0.45 to 0.66), time to diagnosis (6.1 vs 4.2 years, SMD 0.31; 95% CI: 0.11 to 0.51) and mSASSS (8.1 vs 2.7, SMD 0.52; 95% CI: 0.41 to 0.63). Pooled analysis also showed in r-axSpA compared with nr-axSpA a significantly higher prevalence of males (69.6% vs 53.6%, RR 1.30; 95% CI: 1.18 to 1.43), smokers (37.7% vs 31.1%, RR 1.18; 95% CI: 1.09 to 1.28) and uveitis (18.0% vs 14.3%, RR 1.31; 95% CI: 1.05 to 1.62). However, peripheral manifestations such as peripheral arthritis (r-axSpA vs nr-axSpA: 32.8% vs 35.2%, RR 0.87; 95% CI: 0.81 to 0.93), dactylitis (5.6% vs 7.6%, RR 0.64; 95% CI: 0.50 to 0.82) and any enthesitis (23.0% vs 30.1%, RR 0.84; 95% CI: 0.74 to 0.96) were more prevalent among nr-axSpA compared with patients with r-axSpA. The percentage of patients with structural lesions, such as erosions on MRI-SIJ (70.8% vs 40.9%, RR 1.76; 95% CI: 1.05 to 2.97), fatty lesions on MRI-SIJ (79.4% vs 51.5%, RR 1.41; 95% CI: 1.17 to 1.70) and with at least one syndesmophyte (26.4% vs 9.7%, RR 2.6; 95% CI: 1.71 to 4.16) were significantly higher in patients with r-axSpA vs nr-axSpA. The grouping of this findings as the outcome ‘typical structural lesions’ was not available in the included studies. We did not find significant differences on BMI or inflammatory lesions on MRI (SPARCC total SIJ and Berlin activity score on MRI-spine). Ethnicity, HLA-B27 status, IBP, response to NSAIDs, family history of SpA, heel enthesitis, psoriasis, IBD and positive MRI-SIJ according to the ASAS definition were also similar in both groups (p>0.05). Education level was reported by only two manuscripts using different outcomes, which did not allow a pooled analysis.
Comparison of clinical presentation between r-axSpA and nr-axSpA: pooled analysis
Burden of disease
Concerning the burden of disease (table 3), patients with r-axSpA showed significantly higher disease activity evaluated by CRP (9.3 vs 6.2 mg/dL, SMD 0.30; 95% CI: 0.20 to 0.39) and ESR (24.4 vs 20.4 mm/h, SMD 0.24; 95% CI: 0.15 to 0.33). Other variables, such as ASDAS-CRP, VAS back pain, Physician Global Assessment, BASFI, ASQoL and HADS-depression, were significantly different between r-axSpA and nr-axSpA, but the SMDs were less than 0.2 in all cases. We did not find differences between the two groups concerning BASDAI, VAS pain, Patient Global Assessment, HAQ-S, SF-36 questionnaire, EuroQoL questionnaire-5D or HADS-anxiety. Interestingly, medium differences between r-axSpA and nr-axSpA were found with regard mobility (evaluated with BASMI) (2.8 vs 1.6, SMD 0.69; 95% CI: 0.5 to 0.9).
Comparison of the burden of disease between r-axSpA and nr-axSpA: pooled analysis
Quantitative data from the WPAI questionnaire were only provided in one manuscript, precluding from a pooled analysis.27 Individual data showed that presenteeism and activity impairment scores were higher in patients with nr-axSpA (24.2 vs 31.6 and 28.6 vs 36.6 for r-axSpA vs nr-axSpA, respectively). No differences were found in either absenteeism or work productivity loss.
Treatment modalities and treatment effect
Modalities of all drug classes were comparable between both groups (table 4). Nine manuscripts belonging to three RCTs evaluating the effect of bDMARDs were included for the assessment of treatment effect. A pooled analysis could not be performed due to the different interventions and different follow-up periods across the studies. Results from the individual studies are summarised here: in the ESTHER trial (etanercept vs sulfasalazine), no significant differences after 1 year of follow-up for either ASAS partial remission or ASDAS major improvement between the r-axSpA and nr-axSpA were found (online supplementary table S4). Furthermore, both groups showed similar ASDAS and BASDAI scores at the 3-year time point. The RAPID trial (certolizumab vs placebo) was the only one with stratified randomisation for r-axSpA and nr-axSpA (online supplementary table S5). A direct comparison between these two groups was only reported for the 6-month time point, without significant differences regarding the ASAS40. We calculated by ourselves a χ2 test using data from the manuscript to determine whether differences exist between these two groups at the 2-year and 4-year time point, and we found no significant difference for the ASAS40. The same holds for the INFAST study (infliximab +naproxen vs placebo +naproxen), where efficacy outcomes were provided by groups, but not formally statistically compared (online supplementary table S6). However, using data from the manuscript, we found that the percentage of patients who achieved ASAS40 among the Infliximab+naproxen arm was significantly higher (86.9% vs 60.0%) for the r-axSpA group.
Comparison of treatment modalities between r-axSpA and nr-axSpA: pooled analysis
Discussion
This SLR and meta-analysis, aiming to compare patients with r-axSpA and nr-axSpA, has revealed large similarities with regard to clinical presentation, burden of disease, treatment modalities and treatment effect.
Some differences between patients with r-axSpA and nr-axSpA were found, namely for classical risk factors for structural damage (longer disease duration, male gender, smoking and increased CRP, which were indeed more frequently observed in patients with r-axSpA) and peripheral involvement (which was more frequent in patients with nr-axSpA). However, this latter finding should be interpreted with caution, since peripheral manifestations might have allowed the classification of nr-axSpA in the absence of positive radiographic sacroiliitis, creating an artificial increased prevalence of such feature among this group. Interestingly, no significant differences were found for the HLA-B27 positive prevalence. This result is in line with a previous study, in which HLA-B27 was equally prevalent in both groups.28 An interesting explanation is provided by these authors, who considered that HLA-B27 might be artificially over-represented in nr-axSpA because a positive HLA-B27 is mandatory to fulfil the clinical arm for nr-axSpA in the ASAS criteria.
As expected, our data showed a greater structural damage also on MRI of the SIJ (erosions and fatty lesions) and in the spine (higher mSASSS), as well as poorer mobility (evaluated by BASMI) in the r-axSpA group. This higher structural damage in patients with r-axSpA could also be a reflection of the longer disease duration and time to diagnosis (ie, diagnostic delay), despite a similar age at symptoms onset between r-axSpA and nr-axSpA. However, in spite of this increased structural damage in the r-axSpA group, no differences were found in terms of local inflammation, patient-reported outcomes for disease activity/function/quality of life, nor for treatment modalities. This suggests that patients with nr-axSpA, even if they never develop radiographic sacroiliitis, have a comparable disease activity and disease burden to those with r-axSpA and need similar treatment.
Concerning the treatment effect, no conclusions could be drawn due to the limited studies, but the data available did not suggest any differences concerning efficacy outcomes between the two phenotypes. This lack of RCTs including r-axSpA and nr-axSpA provides evidence for the necessity of studies covering the entire axSpA group.
Our study has some limitations but also some strengths that are worth mentioning. First, we have included in the analysis studies that were not designed to compare these two populations, and this could have led to over-represented subpopulations among a group: for example, MRI-SIJ-positive patients among the nr-axSpA group in the RCTs.
Another limitation concerns the nr-axSpA group itself, that encompasses both patients with MRI-SIJ positive (ie, fulfilling the imaging arm of the ASAS criteria) and patients who have no imaging abnormalities of the SIJ but are HLAB27 positive (ie, fulfilling the clinical arm of the ASAS criteria): some have criticised the clinical arm, arguing its low specificity (compared with the imaging arm) and its potential for misclassification. We acknowledge that an over-representation of positive MRI-SIJ could exist in this meta-analysis among nr-axSpA group: first, because we only included manuscripts that classified patients according to the ASAS criteria (ie, nr-axSpA group should have either positive MRI-SIJ or fulfil the clinical arm); and second, because some of the included RCTs had a positive MRI-SIJ as a mandatory inclusion criterion for nr-axSpA group. We acknowledge that the ideal scenario would be to compare r-axSpA vs nr-axSpA with/without positive MRI-SIJ; however, we could not perform this subanalysis since in 83.3% of the studies outcomes were not reported separately for these subgroups. However, this is the first meta-analysis reporting comparative data on r-axSpA and nr-axSpA outcomes, accounting for the heterogeneity in each variable (through the use of fixed or random effects) and with a high accuracy of the pooled estimates.
All these data suggest that r-axSpA and nr-axSpA present differences mainly related to the factors that will lead or have led to structural damage, but that the burden of the disease and clinical presentation are essentially similar. Furthermore, even in the limited data available, treatment response seems comparable. This supports the concept of axSpA as one single disease. Therefore, patients with both r-axSpA and nr-axSpA should be treated with equal priority, and a distinction between r-axSpA and nr-axSpA should only have implications for clinical research but not for clinical practice. This means that bDMARDs should be prescribed according to ASAS-EULAR recommendations, that is, should be considered in patients with axSpA with active disease and refractory to NSAIDs with either structural damage at SIJ X-rays or objective signs of inflammation (ie, MRI inflammation or increased CRP).29
Further studies comparing patients with nr-axSpA with and without imaging abnormalities should be performed to shed more light on the understanding of axSpA disease burden.
Acknowledgments
We wish to thank Catherine Weill, librarian from 'Bibliothèque Interuniversitaire de Santé – Pôle Médecine et Odontologie', for her help in the systematic literature review.
References
Footnotes
Contributors AM and SR conceived the study, participated in its design and coordination, and critically revised the manuscript. CLM performed the data collection, statistical analysis, interpretation and drafted the manuscript. DvdH, MD and JS participated in the design, data interpretation and critically revised the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.