

Abstract
Objective. Rituximab (RTX) has been used successfully for the treatment of severe Jo1 antibody-associated antisynthetase syndrome. The aim of this retrospective study was to evaluate the effect of RTX in severe Jo1 antisynthetase syndrome and determine predictive factors for response.
Methods. There were 61 patients with Jo1 antisynthetase syndrome identified; 18 of these received RTX. One patient was lost to followup. The remaining 17 patients and 30 out of 43 patients who were treated with conventional immunosuppressive (IS) drugs were followed for a mean of 35 months and 84 months, respectively.
Results. Polymyositis/dermatomyositis (95%) and interstitial lung disease (ILD; 66%) were the dominant clinical manifestations. Detection of anti-Ro52 antibodies (43%) was significantly associated with acute-onset ILD (p = 0.016) with O2 dependency, and patients with high concentrations of anti-Ro52 (20%) had the highest risk (p = 0.0005). Sixteen out of 18 patients (89%) showed a fast and marked response to RTX. Among those patients who were highly positive for anti-Ro52, response to RTX was seen in 7 out of 7 cases (100%), but no response to cyclophosphamide (n = 4), cyclosporine A (n = 3), azathioprine (n = 9), methotrexate (n = 5), or leflunomide (n = 2) was observed. One patient treated with RTX died of pneumonia.
Conclusion. RTX is effective in the treatment of severe forms of Jo1 antisynthetase syndrome. In our retrospective study, the presence of high anti-Ro52 antibody concentrations predicts severe acute-onset ILD and nonresponse to IS drugs. In contrast to conventional IS, RTX is equally effective in patients with Jo1 antisynthetase syndrome, independent of their anti-Ro52 antibody status.
The antisynthetase syndromes are rare systemic autoimmune diseases characterized by polymyositis (PM)/dermatomyositis (DM), interstitial lung disease (ILD), arthritis, mechanic hands, Raynaud phenomenon, and detection of antiaminoacyl-tRNA synthetase antibodies in peripheral blood. To date, 8 different antiaminoacyl-tRNA synthetase antibodies have been described, with Jo1 antibodies being the most common1,2,3. Apart from myositis, ILD is the most frequent and often dominant organ involvement in Jo1 antibody-associated antisynthetase syndrome associated with increased morbidity and mortality3,4,5.
The cytoplasmic Ro/SSA antigen consists of 2 polypeptide components: Ro52 and Ro60. Whereas anti-Ro52 and anti-Ro60 antibodies are equally often seen, for example in Sjögren syndrome, only anti-Ro52 antibodies occur in patients with myositis (30%), showing a strong association with Jo1 antibodies3,6. The frequency of anti-Ro52 antibodies in Jo1 antisynthetase syndrome is 40% to 72% and is not attributable to cross-reactivity between Jo1 and Ro526,7,8,9. They are not associated with a concomitant Sjögren syndrome9. The coincidence of Jo1 and anti-Ro52 antibodies in antisynthetase syndrome has been related to more severe ILD, myositis, and arthritis, and in ILD, to acute-onset respiratory failure and more frequent development of lung fibrosis9,10,11. According to 2 authors, these patients show a worse response to various immunosuppressive drugs [IS; azathioprine (AZA), methotrexate (MTX), cyclosporine (CSA), cyclophosphamide (CYC), intravenous immunoglobulins (IVIG)] and a poorer prognosis with regard to overall survival9,11 in comparison with anti-Ro52–negative patients.
Rituximab (RTX) is a chimeric monoclonal antibody to human CD20, which leads to a depletion of peripheral B lymphocytes. In case reports and series, RTX has been shown to be effective in treating antisynthetase syndrome. So far, the highest reported number of patients with antisynthetase syndrome treated with RTX is 33, and the longest median followup is 52 months12–21,22,23. There are no placebo-controlled prospective studies or studies comparing the effect of RTX with that of conventional IS, to our knowledge. None of the case series with RTX referred to the coincidence of anti-Ro52 antibodies.
The aim of our study was to systematically analyze the outcome of patients with Jo1 antisynthetase syndrome treated with RTX or IS drugs in our centers and to determine the predictive value of anti-Ro52 antibodies for clinical manifestations and treatment outcome.
MATERIALS AND METHODS
We performed a systematic search in the institutional medical record index to identify all patients with Jo1 antisynthetase syndrome treated in 2 rheumatological centers since January 2006. Patients had to fulfill the International Myositis Assessment and Clinical Studies (IMACS)-modified Peter and Bohan criteria24,25 and have positive Jo1 antibodies. For diagnosis of ILD, they had to show significant clinical, functional [pulmonary function test (PFT)], and radiographic signs [computed tomography (CT)] of ILD in the presence of Jo1 antibodies. Bronchoalveolar lavage (BAL) was not compulsory and was left to the pulmonologist’s decision. Diagnosis of DM was made if Gottron papules or heliotrope rash were present. Mechanic hands were assigned to antisynthetase syndrome and not counted as DM.
Jo1 and anti-Ro52 antibodies were measured with the immunoblotting assay ANA Profil 3 EUROLINE (Euroimmun), which presents semiquantitative results separately for Jo1, Ro52, and Ro60. The antibody concentration is ranked on the semiquantitative scale with −, +, ++, and +++, which were validated by a fluorescence enzyme immunoassay (Phadia) in a random selection of 10 sera showing values of 25 U/ml to 240 U/ml in +++ sera and lower than 9.3 U/ml in ++ and + (normal value < 7). In 17 patients, Jo1 antibodies were measured quantitatively.
Further clinical and laboratory data were obtained from the patients’ medical records.
All patients were repeatedly screened for new organ involvement by clinical and laboratory examination (every 3 to 6 mos) and PFT (every 6 to 12 mos), the latter being performed as body plethysmography plus measurement of DLCO (single-breath method). In case of existing ILD, PFT were repeated every 3 to 6 months. Lung function was considered abnormal when volumes or DLCO were < 80% of the predicted values. In case of ILD, patients underwent high-resolution CT scan of the lungs (in the majority of patients repeatedly). Alveolitis and fibrosis were classified semiquantitatively as severe, moderate, or mild according to the results of CT scans and the radiologist’s judgment (1 radiologist in general, or 2 radiologists in unclear cases). Radiologists were blinded for the antibody status. Results were recorded of BAL, if performed, and in case of respiratory failure, duration and amount of O2 substitution. According to their clinical presentations, patients with ILD were divided into 3 groups as defined previously by Marie, et al and Tillie-Leblond, et al4,5: acute-onset ILD, chronic progressive ILD, and asymptomatic ILD with abnormalities in PFT or CT scan without clinical symptoms.
Ethical approval was given by the University of Heidelberg.
Therapeutic regimen
RTX was given according to the standardized protocol for rheumatoid arthritis with 2 × 1 g intravenously (IV; days 0 and 14) in 17 patients accompanied by premedication with 80 mg methylprednisolone IV, 4 mg dimetindenmaleat IV, and 1 g paracetamol administered orally 30 min before each infusion. One patient received 4 weekly RTX infusions of 375 mg/m2 body surface. In most patients, RTX was combined with an additional IS, and in all patients with corticosteroids. Choice of comedication, steroid dose, and tapering were individual decisions and recorded for each patient continuously. RTX cycles were generally repeated every 6 months. In 2006–2008, RTX was repeated after a longer interval (9–12 mos) in 3 patients, which resulted in a new clinical flare in all cases. Therefore, the following cycles were conducted every 6 months.
Outcome
The outcome was categorized as complete response, improvement, or deterioration in accordance with Oddis, et al and Rider, et al25,26 by using an adapted version of the IMACS core set measures, with the exception of validated muscle strength measurement, which was not available for all patients because of the retrospective design. Ascertained were laboratory results [creatine kinase (CK), lactate dehydrogenase, aspartate aminotransferase], physician’s and patient’s global disease activities by visual analog scale (VAS), presence and extent of extramuscular disease by screening as mentioned above, and physical function by a validated patient questionnaire of activities of daily living. Instead of the Health Assessment Questionnaire, the closely related German tool FFbH (Funktionsfragebogen Hannover) was used. Complete response was defined as the resolution of muscle pain and muscle weakness as reported by the patient and tested by physical examination together with the normalization of serum muscle enzyme levels (CK) in the case of myositis; the resolution of pulmonary symptoms, disappearance of radiographic signs of alveolitis, and normalization of standard PFT values in the case of ILD; and the resolution of joint symptoms or the disappearance of mechanic hands or Gottron papules/heliotrope rash in the case of joint or skin involvement, each for at least 6 months. Improvement was defined as the reduction of organ symptoms and the improvement of physician’s and patient’s VAS of at least 30% plus at least 30% improvement in CK levels in the case of myositis, at least 20% improvement of radiographic signs or PFT values in the case of ILD, and the improvement of skin manifestation in skin involvement. Lasting response was defined as the persistence of response in the case of continuous treatment until last followup (at least 6 mos). Refractory disease was defined as the absence of response in spite of treatment. Deterioration was defined as the worsening of symptoms, CK levels (continuous increase > 20%), radiographic signs (increase in alveolitis), or PFT values (decrease > 20%) despite therapy. Single outcome variables were ascertained every 6 months except for CT scans (individual timepoint and frequency).
Data analysis
The Mann-Whitney U test (WinStat) and the Fisher’s exact test (SAS) were used to calculate significance. Moreover, logistic regression was used to calculate predictors (SAS). The results were regarded as significant when p value was < 0.05.
RESULTS
Baseline characteristics
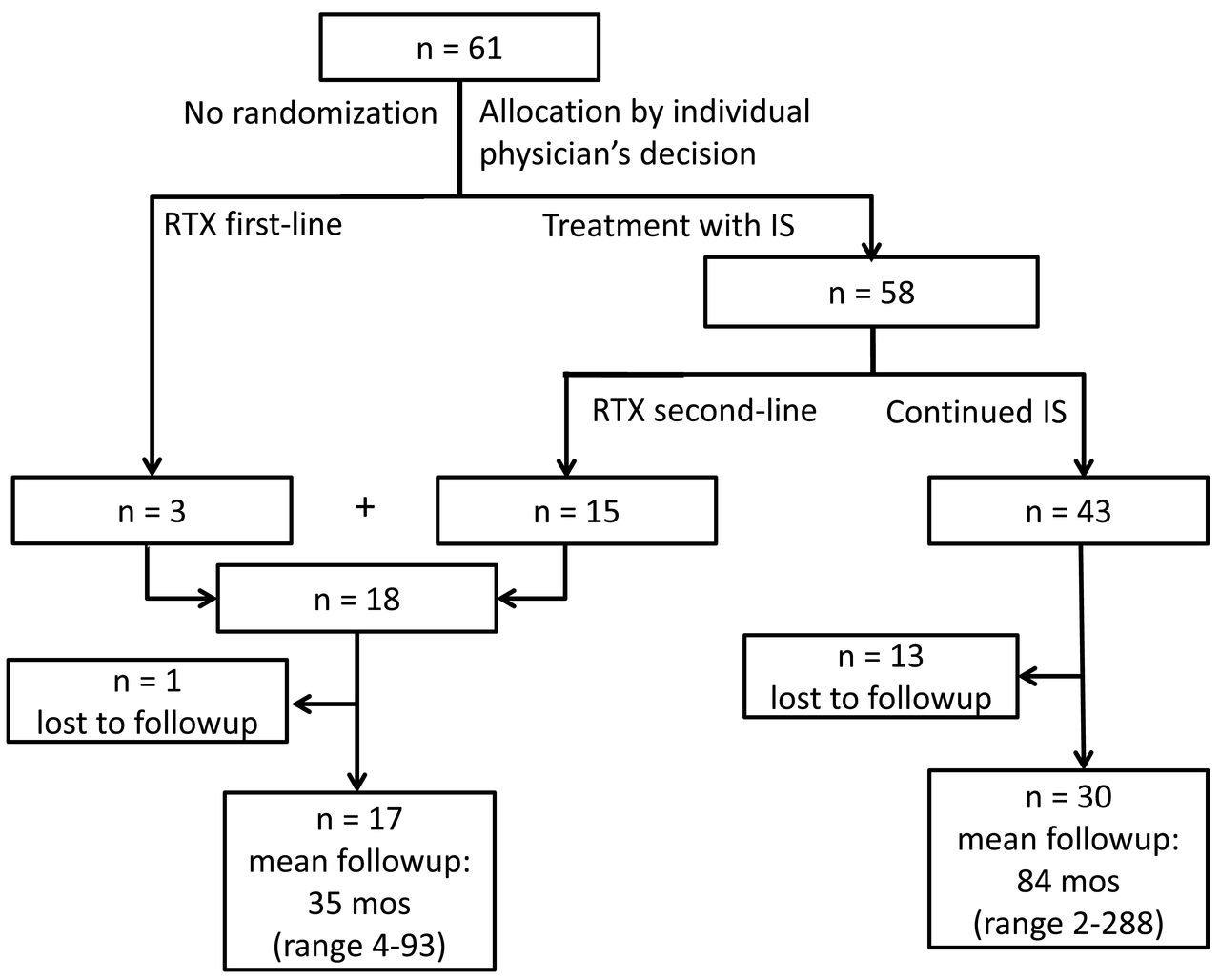
Between January 2006 and August 2014, 61 patients with Jo1 antisynthetase syndrome were identified (Figure 1). Jo1 antibody concentrations were measured semiquantitatively in 44 patients. Results were +++ in 25 (57%), ++ in 9 (20%), and + in 10 patients (23%). Eighteen patients received RTX; 1 was lost to followup. The other 17 were followed with a mean followup of 35 months. Forty-three patients received IS drugs. Thirty of them could be followed up with a mean duration of 84 months.
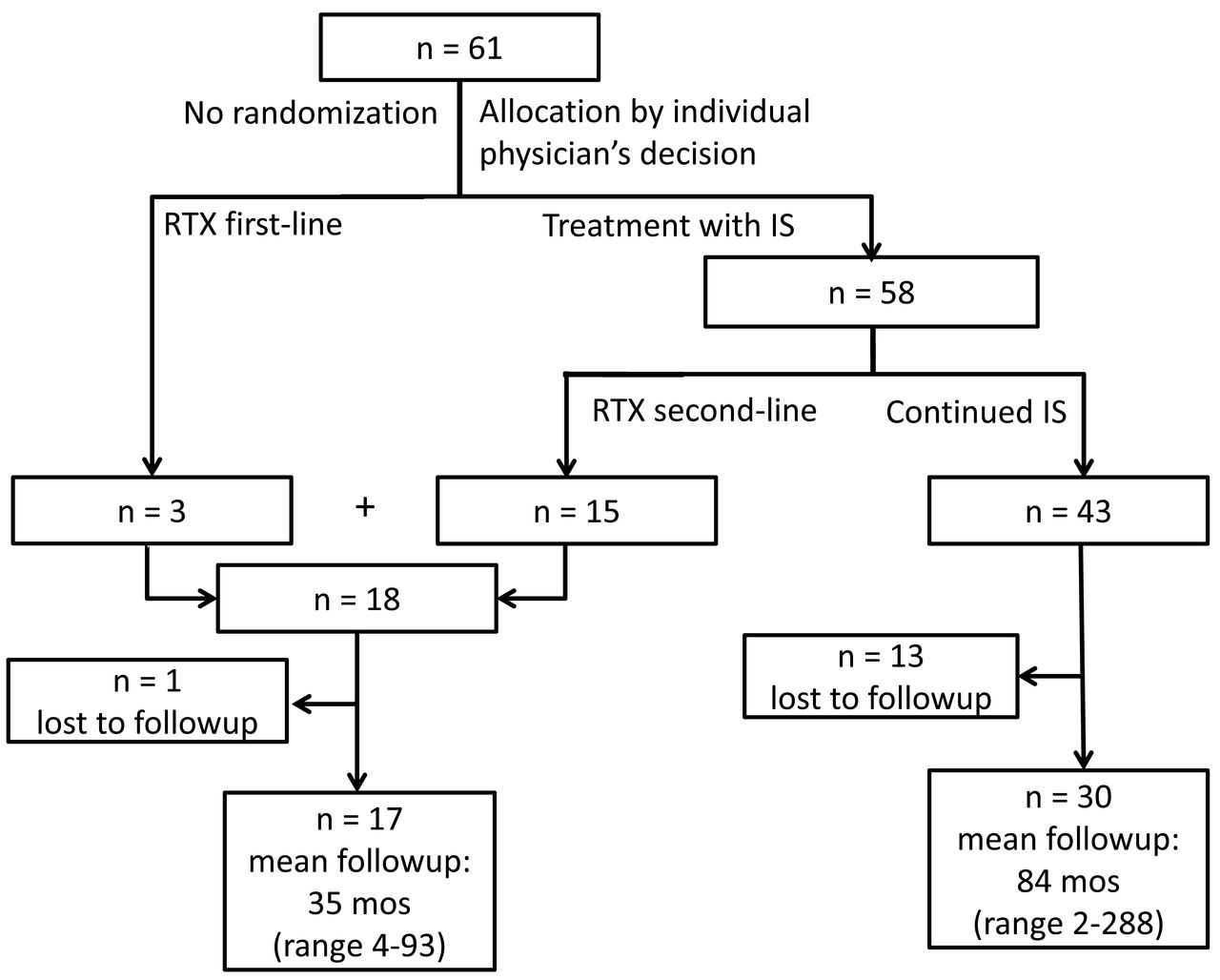
Documentation and followup of patients with Jo1 antibody-associated antisynthetase syndrome. RTX: rituximab; IS: immunosuppressive drugs.
Further baseline characteristics are listed in Table 1 separately for the whole cohort, the RTX group, and the non-RTX group. Frequency of organ involvement and median age at diagnosis corresponded to literature8,27 and were not different between the treatment groups. Further, there was no difference in baseline characteristics between patients with and without followup. Anti-Ro52 antibodies were measured prior to the start of RTX. BAL was performed in 16 patients with ILD (8 RTX, 8 non-RTX), showing lymphocytic alveolitis with reduced CD4:CD8 ratio in 13 patients and neutrophilic alveolitis in 3 (with acute-onset ILD).
Baseline characteristics at first presentation in our centers. No randomization. Values are n (%) unless otherwise specified.
Patients received RTX if they had severe ILD or PM refractory to IS drugs. The mean number of failed IS and mean disease duration before the start of RTX are given in Table 1. IS given before RTX, partly in combination, were AZA (n = 14), MTX (n = 11), CSA (n = 6), CYC (n = 6), leflunomide (LEF: n = 3), mycophenolate mofetil (n = 2), etanercept (n = 2), hydroxychloroquine (n = 2), and infliximab, tacrolimus, or IVIG (n = 1 each). Four patients had received pulsed glucocorticoids before RTX (250 mg prednisolone to 1 g methylprednisolone IV). Time between pulsed glucocorticoids and RTX was 2 to 12 months. Mean CK level at start of RTX was 663 U/l (range 39–2994 U/l, reference < 170 U/l).
All 6 patients with acute-onset ILD in the RTX group needed O2 substitution because of partial hypoxic respiratory failure. They had moderate to severe alveolitis and partly moderate to severe fibrosis, and 1 had pulmonary arterial hypertension (PAH) before RTX. Five patients showed chronic progressive ILD with moderate alveolitis and/or moderate to severe lung fibrosis; of them, 2 also showed PAH (in 1 accompanied by a cor pulmonale with longterm O2 therapy). One patient had mild asymptomatic ILD with predominant PM.
Patients received on average 4.6 cycles of RTX (range 1–13) in a mean interval of 6.4 months, and in 16 of the 18 patients, it was combined with an IS agent. Those were AZA (n = 8), MTX (n = 5), CSA (n = 4), and CYC IV (n = 2, both in severe acute-onset ILD; in 1 patient parallel to the first course of RTX; the other patient was refractory to 5 cycles of CYC and therefore receiving RTX on top of CYC cycles 6 to 8). The concomitant IS were given prior to RTX and were judged as being ineffective in 12 of the 16 patients (partially in combination of several substances). They were introduced together with RTX in 4 patients.
One patient received pulsed prednisolone with 250 mg IV for 3 days parallel to the first dose of RTX. Otherwise, maximum prednisolone-equivalent dose at the start of RTX was 100 mg/day orally or less with a mean of 30.4 mg/day.
Course of disease after RTX treatment
Sixteen out of 17 patients with followup showed complete response of myositis (16 out of 16 patients with myositis) and/or in the case of ILD, complete response (in 1 out of 10 patients with ILD) or improvement (in 9). Mechanic hands was resolved (complete response) in 2 of the 3 patients and there was no response in 1 patient. The 1 patient with DM in the RTX group showed complete response of skin manifestation. One patient with predominant polyarthritis and panniculitis did not respond to the first cycle of RTX.
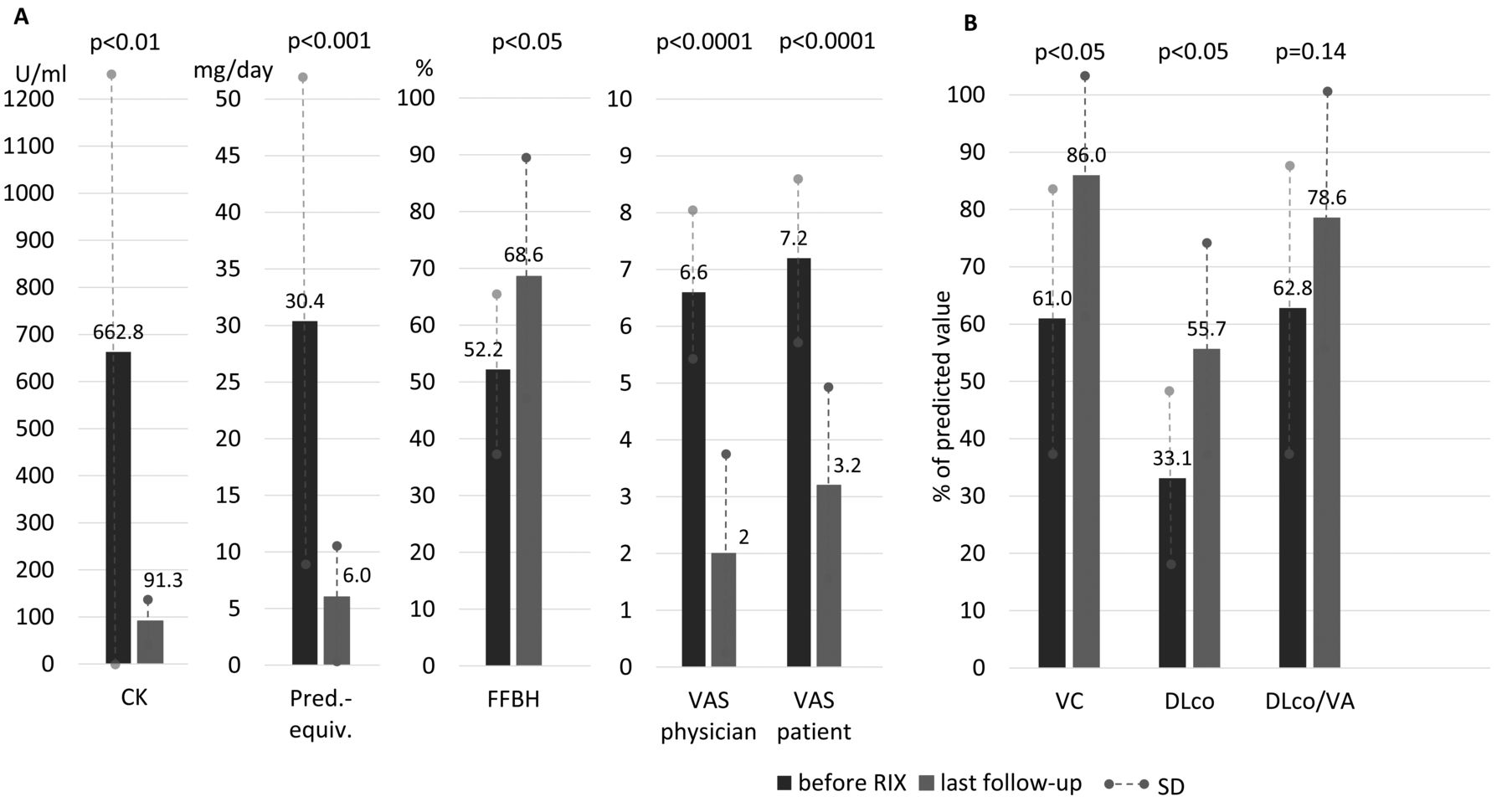
Mean CK concentrations decreased from 663 U/l to 92 U/l (p < 0.01) and prednisolone-equivalent doses per day from 30.4 mg/day to 6.0 mg/day (p < 0.001). Mean vital capacity (VC) increased from 61% at the start of RTX to 86% at the last followup (p < 0.05), DLCO from 33.1% to 55.7% (p < 0.05), and DLCO/alveolar volumes (VA) from 62.8% to 78.6% (p = 0.14), which corresponded to an increase of 40%, 68%, and 25%, respectively. The ascertained IMACS outcome variables are shown in Figure 2 and longitudinal PFT in Figure 3. Two patients with ILD had normal VC at the start of RTX. Of the other 8 patients with ILD, VC increased to ≥ 80% in 4 patients at last followup (plus > 70% in further 2 patients). DLCO/VA increased to ≥ 80% in 5 patients (plus > 70% in further 2). One patient with ILD had DLCO ≥ 80% at last followup and a further 3 patients ≥ 70%. Values for forced vital capacity (FVC) did not differ from VC and are not presented for reasons of clarity. All patients with acute-onset ILD no longer needed O2 substitution after the first cycle of RTX. The 1 patient with cor pulmonale and longterm O2 therapy continued treatment with O2, although PFT results improved as well. CT scans were repeated in 6 of the 10 patients with ILD 6 or 12 months after the start of RTX. Alveolitis completely disappeared in all patients, and fibrosis was stable or slightly improved. Best results in ILD were seen in patients with a short disease duration. In 5 patients with acute-onset ILD, RTX was started within the first 6 months. Their VC improved by 75% (47 ± 11% to 82 ± 6%), DLCO by 126% (26 ± 12% to 59 ± 13%), and DLCO/VA by 56% (55 ± 24% to 86 ± 11%).

(A) Course of CK, prednisolone-equivalent dose, FFbH, VAS physician/patient, and (B) PFT results during RTX therapy. Values for CK and prednisolone-equivalent doses were available in all 17 patients with followup, and values for FFbH and VAS physician/patient were available in 14 patients. PFT shown for the 10 patients with ILD with followup. Significant reductions of CK, prednisolone-equivalent dose per day, and VAS physician/patient were found, and significant increases in FFbH, VC, and DLCO were found. Relative improvement of VC was 40%, relative improvement of DLCO was 68%, and relative improvement of DLCO/VA was 25%. Values for FVC did not differ from VC (not shown). Values given as mean ± SD. CK: creatine kinase; FFbH: Funktionsfragebogen (questionnaire) Hannover; VAS: visual analog scale; PFT: pulmonary function test; RTX: rituximab; ILD: interstitial lung disease; VC: vital capacity; VA: alveolar volumes; FVC: forced VC.
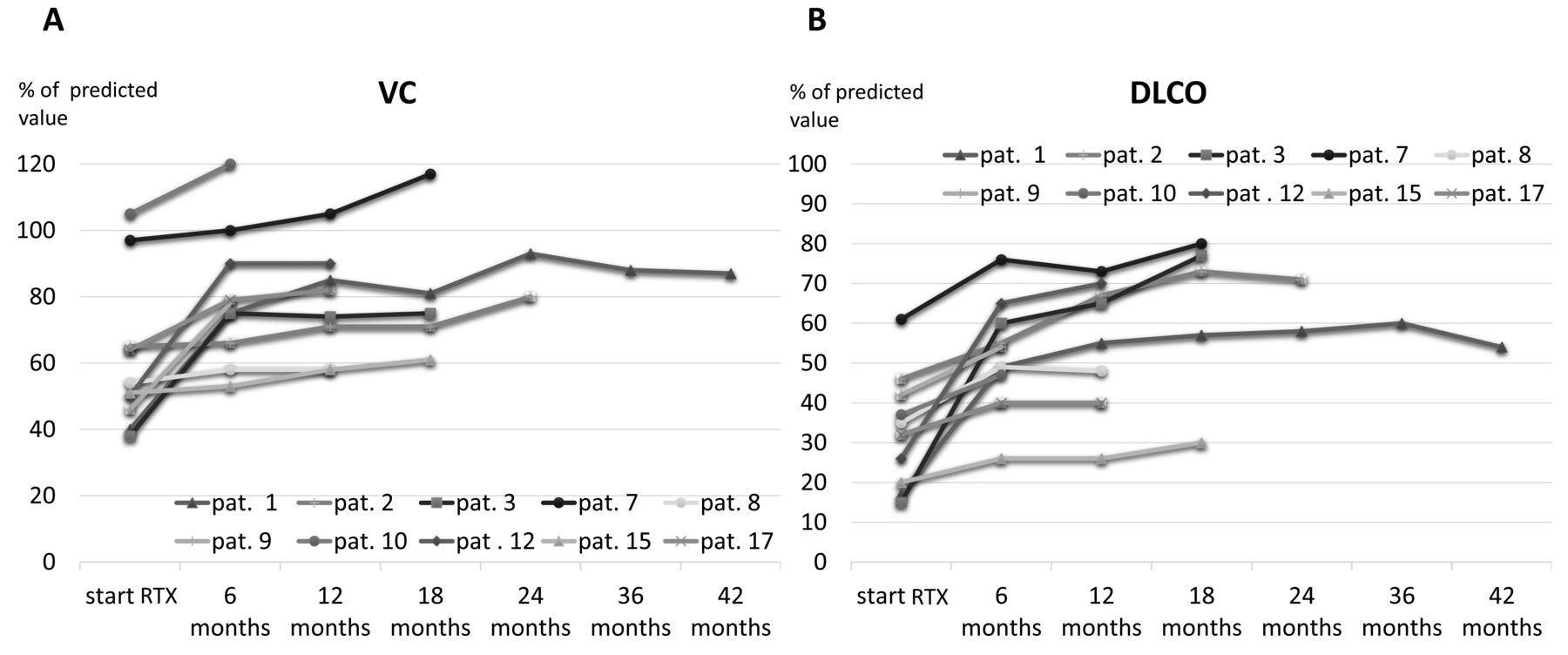
(A) Course of VC and (B) DLCO over time. VC: vital capacity; pat.: patient; RTX: rituximab.
There were 5 relapses in 4 patients; 3 of them in RTX intervals longer than 6 months. In all, RTX was repeated and again had a good effect. In 3 patients with predominant PM and stable complete response, RTX dosage was reduced to 1 g IV per cycle and in 1 of them further to 0.5 g IV per cycle without relapse. In another patient with predominant PM, RTX was stopped after 7 courses, continuing the comedication with MTX and low-dose prednisolone (5 mg/day); this patient has achieved a stable longtime complete response over 3.5 years so far.
Adverse events
One patient died of pneumonia after the second cycle of RTX. After a disease duration of 7 years, this patient had severe lung fibrosis and PAH at the start of RTX, having been refractory to various IS with mean prednisolone doses of 20 mg/day for years.
One patient with high doses of prednisolone before RTX developed a urosepsis only 3 days after the first dose of RTX. It is questionable whether this was a consequence of RTX. After antibiotic treatment, RTX was continued without any further complication. There were several mild urinary tract and upper airway infections and 1 hypertensive crisis with flush. None of them led to a stop of RTX.
Immunoglobulin (Ig) G/IgM levels were available in 12 patients with mean IgG 10.7 ± 1.7 g/l, IgM 1.5 ± 0.16 g/l before RTX, and 8.0 ± 2.8 g/l, 0.8 ± 0.5 g/l at last followup (normal values IgG 7.0–16.0 g/l and IgM 0.4–2.3 g/l, respectively). Five patients (60%) developed hypogammaglobulinemia with IgG 4.8 g/l to 6.3 g/l (range) and IgM 0.31 g/l to 0.37 g/l. There was no correlation to occurring infections. The patients with fatal pneumonia and urosepsis had normal Ig levels (but high prednisolone doses), whereas patients with hypogammaglobulinemia showed no increase in infections with the need of antibiotic treatment.
Association of anti-Ro52 antibodies with clinical manifestations and treatment outcome
Results of anti-Ro52 testing were available in 56 of the 61 patients (Table 1). Anti-Ro52 antibodies were positive in 43% (+, ++, +++) and significantly associated with acute-onset ILD (p = 0.016) with high anti-Ro52 concentrations (+++, in 20%) showing the highest risk (p = 0.0005). There was no association between high anti-Ro52 concentrations and chronic progressive ILD, CK level, patients’ age at diagnosis, and joint or skin involvement (p > 0.34 each). As well, there was no significant association between the concentrations of anti-Ro52 antibodies and Jo1 antibodies (p = 0.41) as measured with the semiquantitative immunoblot.
Anti-Ro52–positive patients responded better to RTX than to IS. Counted in cumulative numbers for each drug (several patients received various drugs consecutively), treatment with RTX resulted in complete response of myositis and improvement or complete response of ILD in 9 out of 10 cases (90%), but with CYC in 0 out of 4 (0%), CSA in 2 out of 8 (25%), AZA in 4 out of 17 (23%), MTX in 3 out of 13 (23%), and LEF in 2 out of 7 (29%). Other IS or biologics were given only in 1 to 3 patients (Table 2).
Treatment response and outcome of patients with high anti-Ro52 antibody concentrations versus patients with low/negative anti-Ro52 antibodies treated with RTX or immunosuppressives. Only patients with followup are shown.
There was a clear difference between patients with high (+++, n = 11, followup in 11) and low (+, ++, n = 13, followup in 9) anti-Ro52 concentrations. Patients with high anti-Ro52 antibodies showed response to RTX (7 out of 7 = 100%), but no response to any given IS (CYC, n = 4; CSA, n = 3; AZA, n = 9; MTX, n = 5; LEF, n = 2). In contrast to that, patients with low anti-Ro52 antibodies responded at least partly to IS [CSA 2 out of 3 (67%), AZA 4 out of 8 (50%), MTX 3 out of 7 (43%), LEF 2 out of 5 (40%); no CYC given to patients with low anti-Ro52 antibodies]. Patients without anti-Ro52 antibodies (n = 32, followup in 27) had comparable response rates to patients with low anti-Ro52 antibodies [CYC 5 out of 9 (56%), CSA 7 out of 10 (70%), AZA 12 out of 22 (55%), MTX 7 out of 13 (54%), LEF 2 out of 4 (50%)]. Because patients without and patients with low anti-Ro52 antibodies responded similarly, we combined them into 1 group (“patients with low/negative anti-Ro52 antibodies”) and compared their response and outcome to “patients with high anti-Ro52 antibody concentrations” (Table 2 and Table 3). Regarding RTX, there was no significant difference in treatment response and outcome between these 2 groups (response rates 100% and 90%).
Disease course of patients with high anti-Ro52 concentrations and patients with low/negative anti-Ro52 antibodies during RTX therapy. Values are mean ± SD.
Anti-Ro52 antibodies converted from +++ to ++ in 1 patient during RTX. Otherwise there was no change of the antibody concentrations of anti-Ro52 and Jo1 antibodies in the used semiquantitative immunoblot during RTX therapy.
The 4 patients with high anti-Ro52 concentrations who did not receive RTX had a poor outcome (Table 2). One had acute-onset ILD, the other 3 had predominant myositis ± chronic progressive ILD. Two died — 1 of urosepsis while taking AZA plus prednisolone (30 mg/day at last followup) and the other of sudden cardiac death during CYC. A third patient with severe PM developed ILD later and was refractory to CSA and CYC. She received RTX on top of CYC in another institution and achieved complete response quickly. The fourth patient showed persistent active disease while receiving AZA, having been refractory to CSA before.
DISCUSSION
The treatment of severe forms of antisynthetase syndrome remains a challenge. IS such as CYC are frequently given. However, no clinical trials about these drugs in antisynthetase syndrome are available. Although RTX has been reported to have a good effect in case series12–21,22,23, the best treatment for refractory cases remains unclear. So far, no predictive marker for treatment response has been described. Coincident anti-Ro52 antibodies have been associated with more severe disease and worse prognosis in Jo1 antisynthetase syndrome9,10,11.
Our retrospective study shows a very good, rapid, and persistent effect of RTX in severe Jo1 antisynthetase syndrome with complete response of myositis and improvement or complete response of ILD in the great majority of patients (89%), with 1 patient lost to followup. Only 1 patient with predominant polyarthritis and panniculitis showed no response.
RTX led to a mean increase in DLCO of 68% and VC of 40%. CK concentrations in serum decreased rapidly to normal values and prednisolone dosage from a mean of 30.4 mg/day to 6 mg/day. All effects were statistically significant, and in terms of lung function, even stronger than those described by Andersson, et al22. Best results in ILD were seen in patients with a short disease duration, presumably because of a lower rate of irreversible lung damage.
In contrast to the study by Andersson, et al22, only 1 patient in our cohort received CYC parallel to RTX. The other patient with CYC had been refractory to 5 cycles before starting RTX. In this and all other cases, we judged the strong and rapid effect to be a result of RTX. An additional effect of the concomitant IS, which had been given to 16 of the 18 patients, or the pulsed prednisolone in 1 patient, cannot be excluded. However, because these drugs had been ineffectively used in most patients prior to the treatment with RTX, we think that a major effect is unlikely.
There was 1 lethal pneumonia in a high-risk patient with advanced lung fibrosis, pretreatment of various IS, and high prednisolone doses for years prior to RTX. No other serious adverse event related to RTX was observed.
We were able to confirm previously reported data that show a more severe ILD in case of coincident anti-Ro52 antibodies. Risk of severe acute-onset ILD was particularly high when anti-Ro52 antibodies were found in high concentrations. In contrast to the results of Marie, et al9, we found no association of anti-Ro52 antibodies with more severe myositis and joint or skin manifestations. Moreover, there was no significant association between concentrations of anti-Ro52 antibodies and those of Jo1 antibodies in the semiquantitative measurement. This demonstrates that both antibodies are independent variables.
Patients with Jo1 antisynthetase syndrome and coincident anti-Ro52 antibodies were reported to respond worse to various IS9,11. Our data confirm these findings. However, looking more closely, this is almost completely attributable to patients with high anti-Ro52 concentrations who did not show any response to conventional IS, including CYC and CSA, whereas patients with low anti-Ro52 antibodies showed similar response rates to patients without anti-Ro52 antibodies. This is remarkable because CYC is often used in cases of severe organ involvement, particularly in antisynthetase syndrome-associated ILD; moreover, calcineurin inhibitors have been reported as a good therapeutic option for patients with antisynthetase syndrome-associated ILD28,29,30. In terms of RTX, all patients with high anti-Ro52 antibodies responded well with no difference to patients with low or negative anti-Ro52 antibodies (Table 2 and Table 3). Moreover, patients with high anti-Ro52 concentrations who did not receive RTX showed a poorer outcome (Table 2). Although this observation is based on a very small number of patients, it corresponds to the poorer prognosis mentioned by other authors9,10,11. However, because the number of patients in our study was small, further investigations are necessary.
The total anti-Ro52 positivity rate of 43% corresponds to previous data6,7,8,9. However, the given frequency ranges widely between 40% and 72%6,7,8,9, which may be due to the different test systems with different sensitivities6. In previous reports about anti-Ro52 antibodies in antisynthetase syndrome, dichotomous qualitative measuring (+, −) was used7,8,9,10,11. Using a semiquantitative test, we were able to show that the height of anti-Ro52 concentration seems to be important for detecting patients with a high risk of severe disease and for predicting treatment response. At the same time, a significant number of patients seem to have low anti-Ro52 antibody concentrations without clinical relevance.
The observation that high anti-Ro52 antibodies are associated with severe organ manifestation in Jo1 antisynthetase syndrome leads to the hypothesis that they are involved in the onset or at least in sustaining the inflammatory process that leads to severe lung and muscle tissue damage. Ro52 is an interferon (IFN)-inducible E3 ligase that mediates the ubiquitination and proteasomal degradation of various IFN regulatory factor transcription factors31,32,33,34,35,36, which leads to a downregulation of proinflammatory cytokines (Type I IFN)34,35,37. Autoantibodies against Ro52 inhibit its E3 ligase activity by steric hindrance38. Suppressed Ro52-mediated ubiquitination may lead to an uncontrolled production of proinflammatory cytokines37 and thereby to an increased disease activity.
Limitations of our study are its retrospective design and the small number of patients. Moreover, patients were not randomized. Therefore, the comparison of the 2 treatment groups might involve a bias. However, by systematically analyzing all patients with antisynthetase syndrome in our 2 centers, we tried to reduce the risk of observational errors. Because antisynthetase syndrome is a rare disorder, no large numbers can be expected. The semiquantitative measurement of anti-Ro52 antibodies does not allow for the determination of absolute cutoff values, and validation of the semiquantitative immunoblot by fluorescence enzyme immunoassay was performed in a subset of patients only. A further limitation is that muscle strength as a part of the proposed IMACS core set measurement for myositis was not available in our patients. However, the available data were sufficient to judge the predefined criteria for improvement and complete response.
RTX appears to be a rapid-acting and safe therapeutic option with lasting effect in patients with severe Jo1 antisynthetase syndrome in general, and in particular in patients with coincident anti-Ro52 antibodies. Anti-Ro52 antibodies (especially in high concentrations) seem to be valuable risk markers for a more severe disease, in particular for severe acute-onset ILD. High anti-Ro52 concentrations may predict resistance to conventional IS including CYC and calcineurin inhibitors, but equally good response to RTX compared with patients with low or negative anti-Ro52 antibodies. Prospective controlled studies should be conducted to verify these results. Quantitative measurement of anti-Ro52 antibodies should be used to identify cutoff values. Until such studies are available, patients with severe Jo1 antisynthetase syndrome should be stratified by anti-Ro52 antibodies and treatment with RTX should be considered early in patients with high anti-Ro52 concentrations, even before the use of CYC or calcineurin inhibitors.
Acknowledgment
We thank the patients and their physicians for their cooperation and willingness to share data with us.
Footnotes
C. Fiehn and H.M. Lorenz have received speaking honoraria from Roche.
- Accepted for publication April 20, 2016.








{kind=link}
{kind=link}
{kind=link}