

Abstract
Objective. The OMERACT-Adherence meeting was convened to discuss the conceptual and methodological challenges in developing a core domain set (Adherence-CDS) for trials of interventions for medication adherence in rheumatology.
Methods. Forty participants from nine countries participated.
Results. Four ideas emerged: for adherence trials, the Adherence-CDS could include adherence and the condition-specific CDS; many factors affect adherence and are intervention targets, contextual factors, or outcome domains; adherence is a critical factor in drug trials; and standardized adherence measures are needed.
Conclusion. Despite the challenges, the meeting clarified an approach to developing an Adherence-CDS that complements existing OMERACT work and methodology.
Medication adherence is suboptimal in rheumatic diseases and has been reported to be as low as 10% in gout and 30% in rheumatoid arthritis (RA)1,2. Broadly, adherence is defined as “the extent to which a person’s behavior — taking medication, following a diet, and/or executing lifestyle changes, corresponds with agreed recommendations from a health care provider”3. The Outcome Measures in Rheumatology Adherence Special Interest Group (OMERACT-Adherence Group) is currently developing a core domain set (CDS) for trials of interventions to improve medication adherence in rheumatology (Adherence-CDS). Our group includes patients, health professionals, and others in a project consisting of a systematic review, qualitative studies, a Delphi survey, and a consensus workshop4.
There are several trials of adherence interventions in rheumatology5. However, no group has examined what outcome domains should be measured in these trials, and those used currently are inconsistent and heterogeneous6. Historically, most CDS in OMERACT have been established for specific conditions. Developing a CDS that is focused on the intervention type rather than a specific condition requires careful thought. In addition, the work of this group is challenging because of the complexity of adherence. There are hundreds of determinants of nonadherence, and reviews of adherence interventions have shown that multifaceted, behavioral interventions are needed to address adherence and produce a substantial change7.
Developing a CDS for complex behavioral interventions that address adherence in rheumatic conditions does not easily fit with the existing OMERACT filter8,9. This report summarizes discussions during the OMERACT-Adherence Group meeting at OMERACT 2018 in Australia, which aimed to:
understand how an Adherence-CDS can be developed alongside existing condition-specific CDS;
review the candidate adherence-related domains from the work to date; and
modify the existing working plan.
MATERIALS AND METHODS
OMERACT-Adherence premeeting reading materials
Prior to the meeting, participants were provided with the OMERACT-Adherence protocol paper4, the European Society of Patient Adherence, COMpliance and Persistence Medication Adherence Reporting Guidelines (EMERGE)10, and the proposed meeting agenda.
Meeting presentations
The meeting commenced with presentations on the definition of medication adherence (including phases: initiation — when the patient takes the first dose of medication; implementation — extent to which a patient’s actual dosing corresponds to the prescription; and persistence — length of time between initiation and last dose)11, research plan4, and preliminary results of the systematic review and focus group studies. These studies will be reported separately; however, preliminary findings are provided below for background to the meeting discussion.
The systematic review examined adherence-related domains in existing randomized and nonrandomized trials of interventions to improve medication adherence in rheumatic conditions. Extracted domains included adherence and adherence-related domains (any domain related to adherence behavior). To date, the most common domains included medication adherence, concerns, knowledge, beliefs, and necessity. Preliminary findings from a nominal group technique study of patients and caregivers with RA, gout, and osteoporosis indicated that trust in doctor, medication effectiveness, medication side effects, doctor’s knowledge, and disease knowledge were important factors influencing medication adherence. The Australian Capital Territory Health Human Research Ethics Committee (ETHLR.15.137) provided ethical approval and all participants provided written informed consent to publish the results of our study.
Meeting discussion
Attendees were provided with an exercise sheet (Figure 1) and a list of preliminary adherence-related domains. Smaller group discussions facilitated by OMERACT-Adherence co-chairs and group members (AK, SJB, MDW, TD, VE, MG, GH, MSV, KT) preceded a larger group discussion facilitated by AK, summarizing participants’ perspectives and suggestions on a flip chart. OMERACT-Adherence Group member attendees contributed to this report.
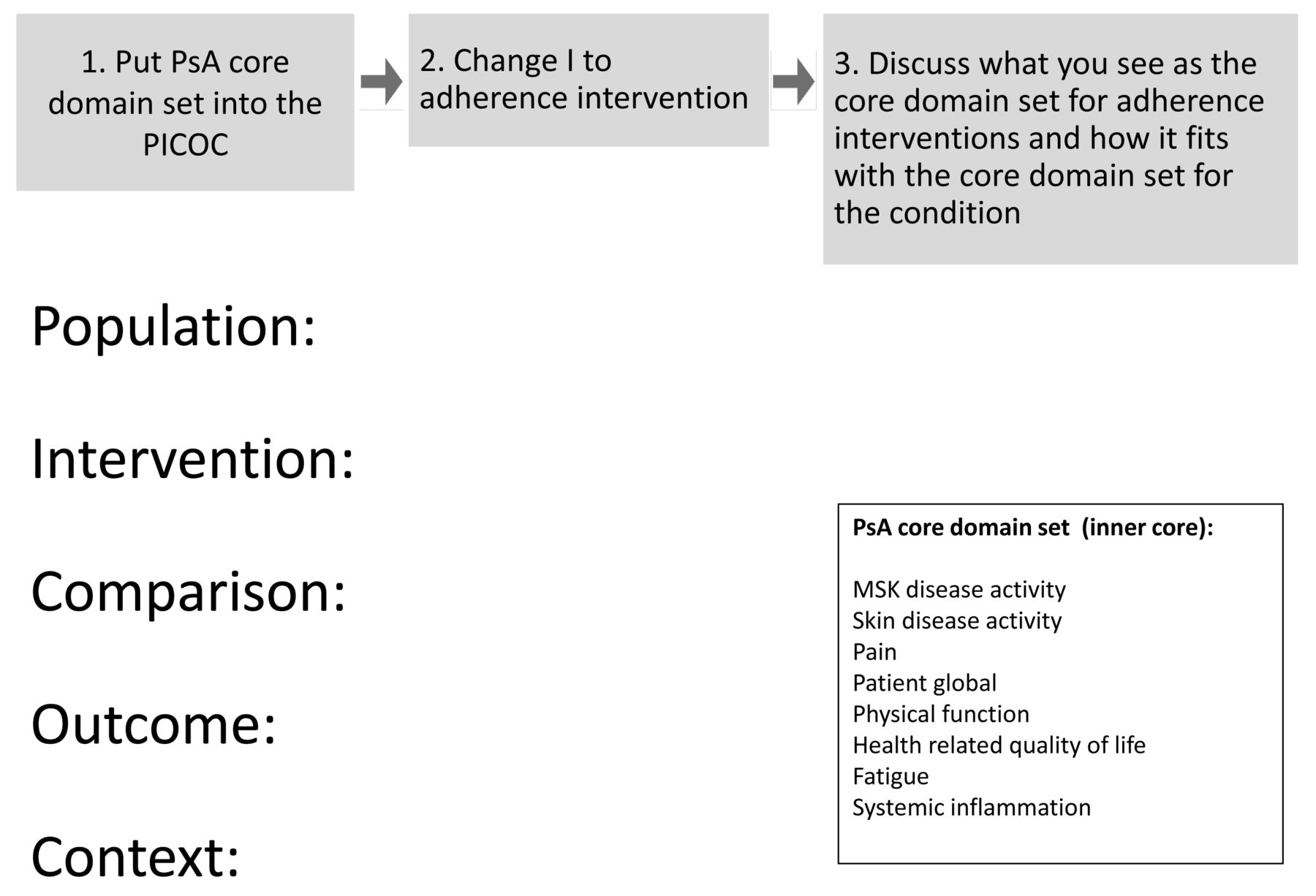
Exercise sheet for OMERACT-Adherence meeting discussion. OMERACT: Outcome Measures in Rheumatology; PsA: psoriatic arthritis; PICOC: Patient/Intervention/Comparator/Outcome/Context; MSK: musculoskeletal.
RESULTS
Forty participants including patients, health professionals, researchers, industry, and regulators from 9 countries contributed to 4 main themes (Table 1):
An Adherence-CDS could include adherence and the condition-specific CDS. Meeting attendees discussed the Adherence-CDS using the PICOC framework (Patient/Intervention/Comparator/Outcome/Context; Figure 2). They suggested adding adherence as a domain to the condition-specific CDS. Although adherence was perceived as a domain itself, it was also considered an explanatory variable, process measure, or biomarker for the condition-specific CDS. One participant suggested that subdomains of adherence could address the phases of initiation, implementation, and persistence. Participants noted that there may be inadequate power or duration of followup to demonstrate changes in disease outcomes even if adherence is improved. For example, use of a comparator group also taking antirheumatic medications may reduce the magnitude of clinical benefit. There was considerable disagreement about whether adherence versus clinical outcomes should serve as the primary outcome. It was suggested that trials aiming to improve adherence in the real-world setting should only be conducted on medications with established efficacy and should be specified in the “Context” of the PICOC framework for the Adherence-CDS.
Factors from the systematic review and focus groups should be classified as intervention targets, contextual factors, or outcome domains. Participants noted that some adherence-related domains identified from the systematic review and focus groups were more accurately classified as targets of interventions or explanatory variables/contextual factors/process measures that influence adherence (e.g., medication knowledge). They provide insight into how adherence interventions can be conceptualized and designed, or could be used to develop a tool to predict adherence, and were suggested to be termed “adherence-related factors.”
Adherence is a critical factor in drug trials. Drug trials (e.g., placebo-controlled trial for an osteoporosis medication) are different from adherence trials (e.g., randomized trial of intensive pharmacist support to address nonadherence). The OMERACT-Adherence Group is currently developing a CDS for adherence trials. Attendees discussed that in drug trials, adherence is an important contextual factor affecting the interpretation of clinical benefit and safety, although this is currently out of the scope of the OMERACT-Adherence work. There was agreement that the reasons for nonadherence in drug trials may differ from those in adherence trials, and therefore different studies would be required to investigate this topic. Some attendees thought that nonadherence was not an issue in drug trials, although there is existing evidence to the contrary12.
Standardized adherence measures are needed in all trials. Participants recognized the need to standardize adherence measures in both adherence and drug trials. There was agreement that in trials, objective measures of adherence are essential, given the well-recognized bias associated with self-reports. Several individuals noted the potential role for measuring serum drug levels and use of technology such as micro-biosensors integrated into pills. The OMERACT-Adherence Group plans to develop a core outcome measurement set after the CDS is established. However, a few participants proposed moving directly to standardizing adherence measures because they felt the OMERACT filter was difficult to apply to an adherence trial.

Proposed OMERACT-Adherence CDS. OMERACT: Outcome Measures in Rheumatology; PsA: psoriatic arthritis; CDS: core domain set.
Key recommendations from the OMERACT-Adherence workshop.
DISCUSSION
Forming consensus on what to measure in complex behavioral interventions that address medication adherence across rheumatic conditions is challenging, and the direct application of OMERACT Filter 2.19,10 is not straightforward. The suggestion to add adherence to the inner circle of a condition-specific CDS (as being mandatory in an adherence trial) offers a potential solution. Adherence-related factors must be clearly classified as targets of interventions or explanatory variables for adherence, though some may be candidate outcome domains. Adherence as a contextual factor of drug trials, and consensus on standardized adherence measures, are important and require further investigation.
Participants who found it difficult to apply the OMERACT filter to an adherence trial did not see the value in reaching consensus on outcome domains and suggested proceeding immediately to standardization of adherence measures. However, similar to condition-specific CDS, an Adherence-CDS can reduce inconsistent reporting and reporting bias and promote measurement of outcomes that matter to patients10.
Clinical outcomes represented by the condition-specific CDS are infrequently reported domains of adherence trials, but are examples of outcomes that matter to patients and were highly valued in our focus groups. The importance of measuring medication side effects was demonstrated in a cohort study of kidney transplant recipients who had increased risk of malignancy with higher medication adherence13. Making it mandatory to report the condition-specific CDS in all adherence trials could provide valuable information and progress in adherence research. Although discussions highlighted the difficulties of using the condition-specific CDS in adherence trials, limitations in power and duration of followup can also apply to drug trials for some clinical outcomes such as mortality.
Future steps need to address the interdependence of the condition-specific CDS with the Adherence-CDS and whether clinical outcomes are important and feasible to measure in all adherence trials. These activities have been prioritized to move forward. We will update the systematic review and assess whether existing adherence trials also include the condition-specific CDS, including reporting of medication side effects. Domains extracted from the systematic review and focus groups will be termed adherence-related factors, with further work to scrutinize what will be candidate domains for the Adherence-CDS. We plan to reconcile the disagreement regarding the primary outcomes in adherence trials (improved adherence vs clinical benefit).
Adherence is important in the clinical setting not only to patients and clinicians, but also to regulators and payers to ensure that patients maximize the potential health benefits from medications. As an increasing number of interventions are conducted to improve adherence in rheumatology, these need to measure relevant and consistent outcome domains. Key recommendations from the OMERACT-Adherence group following the workshop are summarized in Table 1.
Acknowledgment
The authors acknowledge the contribution of other members of the OMERACT-Adherence group who have contributed to the development, design, conduct, and analysis of the studies to date: Alexa Meara, Annica Barcenilla-Wong, Bart Van den Bemt, Beverley J. Shea, Catherine Hill, Christine Bailey, Clare O’Sullivan, Daniel Sumpton, Francois Nantel, Helen Keen, Irwin Lim, Karine Toupin-April, Lara Maxwell, Luke Crimston-Smith, Maria Suarez-Almazor, Marita Cross, Mary De Vera, Peter Cheung, Rani Sinnathurai, Renske Hebing, Rieke Alten, Robby Nieuwlaat, Robin Christensen, Sabrina Mai Nielson, Sean O’Neill, Stephen Hall, Willemina Campbell, and Yomei Shaw.
Footnotes
The work of OMERACT-Adherence to date has been supported by a 2018 Arthritis Australia project grant. JAS is a member of the executive of OMERACT, an organization that develops outcome measures in rheumatology and receives arms-length funding from 36 companies.
- Accepted for publication November 26, 2018.








{kind=link}
{kind=link}