

Abstract
Objective. Systemic lupus erythematosus (SLE) is a disease of considerable morbidity, and this may place patients at greater risk for poor in-hospital postoperative outcomes for procedures such as arthroplasty. Our aim was to test this hypothesis.
Methods. We compared the in-hospital postoperative mortality risk for patients with SLE undergoing hip and knee arthroplasty to those with rheumatoid arthritis (RA) and the general population without either condition, using data from the Nationwide Inpatient Sample (1993–2006). We performed parallel, weighted, multivariable logistic regressions to calculate mortality risk stratified by joint site, type of admission, hospital type, income category, race, length of stay, surgical indication, and medical comorbidities.
Results. The unadjusted mortality rates (per 1000 procedures) for patients with SLE, patients with RA, and controls were 7.4, 3.0, and 6.5, respectively, for nonelective procedures and 2.4, 1.3, and 1.8 for elective procedures. After adjustment for potential confounders, patients with SLE had an OR of 4.0 (95% CI 1.9–8.0) for postoperative mortality with hip replacements and an OR of 1.2 (95% CI 0.2–7.5) for mortality with knee replacements. Mortality risk of patients with RA was not different from that of controls. The adjusted risk estimates for those who underwent arthroplasty before and after 2002 and those who underwent surgery for nonfracture indications were similar.
Conclusion. Arthroplasty, especially of hips, in patients with SLE is associated with relatively higher postoperative mortality risk.
Systemic lupus erythematosus (SLE) is a multisystem autoimmune disease predominantly affecting young women. Thirty years ago, 75% of patients with this disease died within 5 years of diagnosis1–3. More recently, over 90% of patients with SLE can expect a 10-year survival1. The use of glucocorticoids, which can be credited with improving the mortality outcomes, is also associated with excess risk for avascular necroses, osteoporosis, and pathological fractures. Further, as more of these patients survive young adulthood and enter middle and old age, the prevalence of both the damage from inflammatory arthritis and osteoarthritis (OA) also increases. Combined, these factors will continue to increase the need for and use of arthroplasty in patients with SLE.
Arthroplasty is almost always performed in an elective/selective fashion. Consequently, the in-hospital mortality after total joint arthroplasty is generally low, with mortality following total hip replacement consistently higher (0.18%–0.52%)4–6 than for total knee replacement (0.18%–0.27%)7. There are few published data that address whether these procedures are just as safe among patients with SLE. We hypothesized that patients with SLE have worse in-hospital mortality outcomes after total joint arthroplasty, and that this excess risk is not explained by other medical comorbidities.
MATERIALS AND METHODS
Database
This was a cross-sectional analysis. We pooled 14 years of hospital discharge data from the Healthcare Cost and Utilization Project Nationwide Inpatient Sample (NIS) for the period of 1993–2006. The NIS is the largest hospitalization database in the world. It is composed of a stratified sample from 20% of US community hospitals and contains about 7 million hospital discharge records per year. For each individual hospitalization, data from the discharge summary are abstracted into the database. The data include age, gender, type of hospitalization (elective vs nonelective), up to 15 diagnoses, 15 procedural codes performed during the hospitalization, and vital status at the end of the hospitalization. The NIS data have been previously described and used for health outcomes research on arthroplasty8. As our study uses data available to the public, the institutional review board at the University of Pittsburgh considers it exempt.
Study criteria, patient identification, and outcome
We identified all patients age 16 years or older who had a primary listed procedure code [International Classification of Disease-9 Clinical Modification (ICD9-CM) codes 81.51, 81.53, 81.54, and 81.55 for Procedures] corresponding to primary and revision hip and knee arthroplasty. Among this group we identified those with a discharge diagnosis of SLE (ICD9-CM 710.0) and rheumatoid arthritis (RA; ICD9-CM 714.0). We excluded those hospitalizations that had diagnosis codes for both SLE and RA, as these 2 diagnoses rarely occur concomitantly in 1 patient, and represent coding errors. We also excluded those that had a coexistent diagnosis of bone cancer or metastatic disease. The outcome of interest was in-hospital mortality among 3 groups of patients: SLE, RA, and all the rest (controls).
Comorbidity measure
We modified the Deyo-Charlson comorbidity index such that RA and SLE were excluded as scoring factors and used regression models to adjust for the effect of comorbidity8.
Statistics
Since these data were from a complex survey, we used survey weights in all analyses. All estimates are therefore weighted unless otherwise specified. We used multivariable logistic regression to estimate the effect of SLE and RA on in-hospital mortality among arthroplasty hospitalizations after adjusting for age, gender, race, comorbidity index, and surgical indication. Additional analysis stratified by elective/nonelective admissions, site, or arthroplasty. All analyses were performed using SAS 9 (SAS Inc., Cary, NC, USA).
Subgroup analyses
It was recognized that arthroplasty for fracture, typically osteoporosis-related but also related to other metabolic bone diseases, might have systematically different outcomes compared to those performed for nonfracture indications. Therefore we performed parallel regression models for nonfracture arthroplasty separately.
African American ethnicity is associated with worse health outcomes in general9. Further, this ethnicity is associated with increased incidence of SLE and worse SLE outcomes10. Unfortunately, several states within the NIS did not provide ethnicity information, leading to a significant proportion of missing values for it (26.3%). We therefore performed parallel multivariable regressions excluding and including the race and income variables.
RESULTS
Sample characteristics
There were 1,544,473 hip or knee arthroplasties in the NIS database in the study period. After excluding 878 arthroplasties with a coexistent diagnosis of RA and SLE, and 3247 done on patients with a diagnosis of bone malignancy, a total of 1,540,348 arthroplasties were available for analysis. From these we identified 5585 arthroplasties in patients with SLE, 53,442 among patients with RA, and 1,481,321 in all others. The study sample characteristics are given in Table 1. As expected, the patients with SLE were younger, with a mean age of 54.5 years, and predominantly women (89.4%), compared to the RA group (mean age 64.3 yrs, 76.7% women) or the control group (mean age 67.7 yrs, 60.7% women).
Characteristics of patients undergoing hip or knee arthroplasty. Mean numbers (95% CI) are provided unless specified otherwise.
Race information was not available or missing in 26% of all observations. Where available, there was a greater proportion of African Americans amid the patients with SLE (22.9% vs the 8.9% with RA and 6.2% of controls). Patients with SLE undergoing arthroplasty were more likely to be located at urban teaching hospitals, and have more hip than knee arthroplasties.
Indications for arthroplasty
Patients with SLE underwent a higher frequency of hip compared to knee arthroplasties than patients with RA or the control group (56.4%, 35.6%, 37.7%, respectively; p < 0.001). The higher frequency of hip arthroplasty is likely related to the surgical indication for arthroplasty, which in SLE showed a significantly increased proportion of avascular necrosis, at 26.8%, compared to the frequency in RA (3.2%) or other patients (3.8%; p < 0.001). OA was the most common indication among controls, at 86.2%, and fracture was the indication for surgery in 1.97% of arthroplasties.
Comorbidity
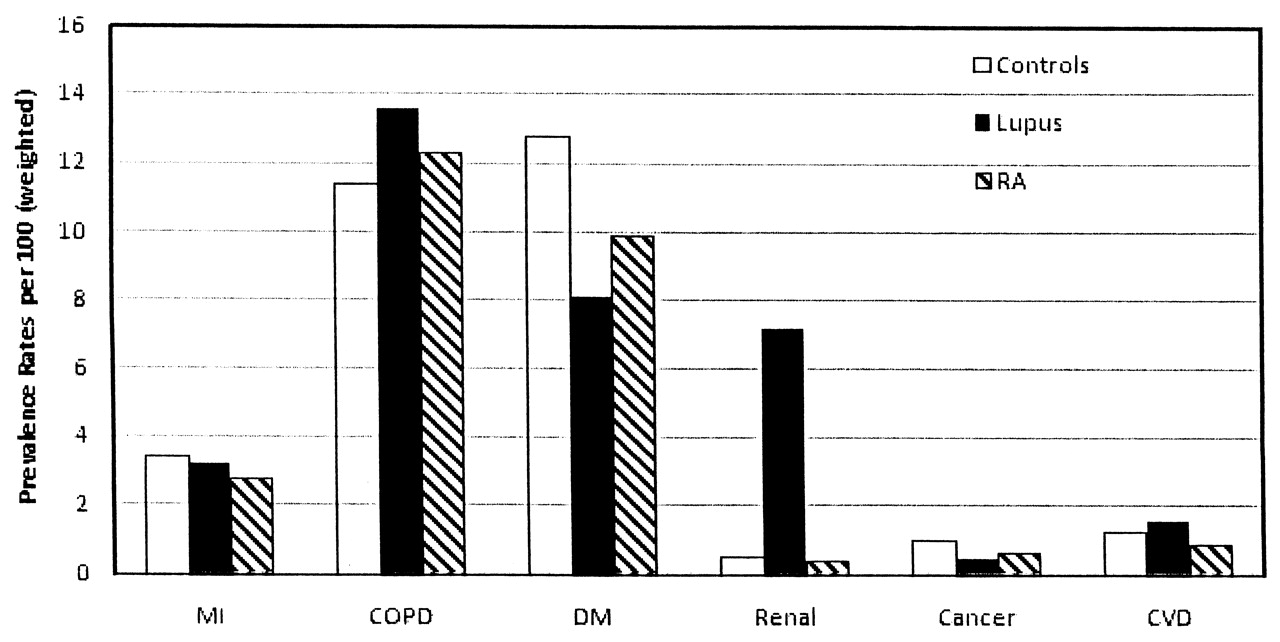
There were significant differences in the frequency of comorbidities between the 3 patient groups, as depicted in Figure 1. Patients with SLE who were undergoing arthroplasty had less frequent diabetes, coronary artery disease, and chronic obstructive pulmonary disease than controls, but nearly equivalent rates of obesity. Patients with SLE had a higher rate of osteoporosis, as expected, but also a higher rate of chronic kidney disease. The mean modified comorbidity index was 0.49 (in SLE), 0.35 (RA), and 0.40 (control) for the 3 groups in both the elective and nonelective categories (p < 0.001).

Prevalence of specific comorbidities among patients with systemic lupus erythematosus, patients with RA, and control groups of patients undergoing hip and knee arthroplasty between 1993 and 2006. Weighted estimates are provided. Data from the Nationwide Inpatient Sample. MI: myocardial infarction; COPD: chronic obstructive pulmonary disease; DM: diabetes mellitus; Renal: renal disease; Cancer: any malignancy; CVD: cerebrovascular disease.
Mortality outcomes
Unadjusted mortality rates by site of arthroplasty and admission type are displayed in Table 2. In general, elective arthroplasty was associated with lower mortality rates compared with the corresponding nonelective arthroplasty group. Among those in the nonfracture arthroplasty group, the overall mortality rate was 2.97, 1.45, and 2.04 per 1000 patients in the SLE, RA, and control groups, respectively. Specifically, the mortality rate in the nonfracture groups was 5.82, 2.52, and 3.70 for 1000 patients with SLE, patients with RA, and those in the control group undergoing elective arthroplasty, and 2.38, 1.23, and 1.73 for 1000 patients with SLE, patients with RA, and those in the control group undergoing nonelective arthroplasty.
Unadjusted in-hospital mortality by site of arthroplasty and admission.
Logistic regression models
In age-adjusted and sex-adjusted logistic regression models, having SLE was associated with an overall large increase in mortality risk compared to controls, whether the procedure was elective (OR 3.7, 95% CI 2.1–6.7) or not (OR 3.5, 95% CI 1.7–7.1). This contrasted with patients with RA, who did not have an increased risk of death compared to controls (elective: OR 0.98, 95% CI 0.8–1.3; nonelective: OR 0.73, 95% CI 0.5–1.1). This pattern was observed among those who underwent hip and knee replacements. Additionally, we performed analyses for the nonfracture subgroup, and the results were similar to the overall results (SLE vs controls: elective OR 3.8, 95% CI 2.1–6.8, and nonelective OR 4.2, 95% CI 1.9–9.6; RA vs controls: elective OR 0.98, 95% CI 0.8–1.3, and nonelective OR 0.97, 95% CI 0.6–1.5).
In multivariable regressions that adjusted for age, gender, comorbidity index, length of hospital stay, presence of avascular necrosis, and location, SLE was associated with excess mortality risk compared to controls, while RA was not (Table 3). Nonelective procedures were associated with excess risk; elective procedures were associated with higher risk but the confidence bounds included unity. In the nonfracture subgroup we observed that SLE was associated with about a 2-fold excess risk for elective procedures and a 4-fold increased mortality risk compared to controls.
Results of multivariable weighted logistic regression for the determinants of postarthroplasty mortality. Mortality risk adjusted for the following factors: age, sex, hospital type, surgical indication, length of hospital stay, and modified comorbidity index.
We then evaluated the potential differences across calendar years, as the quality of medical care is changing over time. Prior to 2002 (an arbitrarily chosen cutoff), both elective and nonelective arthroplasty among patients with SLE were associated with excess mortality risk. In the later period the excess risk was significant only in the nonelective group.
When analyses were repeated after including race and income in the model, the mortality risk pattern was similar to the previous model, but statistical significance was limited to nonelective arthroplasty (Table 4).
Results of multivariable regression including race and income. Adjusted for race, age, sex, hospital type, surgical indication, length of hospital stay, income, and modified comorbidity index.
DISCUSSION
Arthroplasty can improve health-related quality of life for patients with SLE11. Relatively few studies have examined the outcomes of total hip or knee replacement in patients with rheumatic diseases. Those published studies have largely focused on RA. Large series from the Mayo Clinic12, the Veterans Administration hospital13, and single surgeon reports14 did not find an increased risk of 30-day mortality in patients with RA compared to other surgical indications, or OA. This is consistent with our data that demonstrate no difference in age-adjusted and sex-adjusted mortality outcomes in RA compared to controls. One study from Norway examined 60-day age and sex-adjusted mortality in RA and other surgical indications compared to OA, and demonstrated a greater risk. This may reflect the difference between in-hospital and 60-day mortality. A small case series of 31 patients with SLE undergoing hip arthroplasty for avascular necrosis reported relatively higher risk for postoperative wound infections15. Another uncontrolled study of 33 patients with SLE suggested no such excess morbidity and reported a 5-year survivorship of about 80%16. None of these studies evaluated relative risk for mortality in SLE.
Careful preoperative risk assessment, case selection, and patient preference influence the decision to undergo joint arthroplasty. In spite of such selectivity and younger age, we observed that patients with SLE have a 2- to 7-fold higher risk of in-hospital mortality following arthroplasty. This excess risk was observed in both elective and nonelective arthroplasties and is independent of age, sex, and major medical comorbidities. These results have implications for risk stratification and preoperative care for patients with SLE undergoing arthroplasty.
Among the control group, the postoperative mortality rates for knee arthroplasty observed were similar to those reported from a large retrospective study of 22,450 patients seen at the Mayo Clinic13. The postoperative mortality rates for total hip replacement are generally slightly higher than those found in our study, but frequently include data from before the routine use of chemoprophylaxis for thromboembolic events; this may contribute to the higher rate1,2,17,18.
The reason for the excess mortality observed among patients with SLE in our study is unclear, but may represent factors associated with the disease or an independent risk of the disease itself. Risks of the disease could include chronic inflammation or thrombosis associated with antiphospholipid antibodies. Potential important factors associated with SLE include unrecognized comorbid atherosclerotic cardiovascular disease19, secondary chronic renal insufficiency, infection in the setting of immunosuppression20, and the effect of therapy on postoperative healing21. Additionally, both the physicians and the patients themselves may underestimate the degree of disease activity when deciding to go ahead with arthroplasty. The role of comorbidities in our observation is unclear. For example, we assessed the effect of chronic kidney disease (CKD) as a potential factor and found it to have increased risk of death when present in patients with SLE. Unfortunately, given the limitations inherent in hospital discharge data with scant specific clinical data, we could not reliably test this effect further or evaluate mechanistic hypotheses. The effect of specific comorbidities, such as CKD, on in-hospital mortality in patients with SLE should be evaluated further in future studies. As expected, the frequency of avascular necrosis was highest in our group of patients with SLE, while its prevalence in other populations is reported to be between 3% and 30%22,23.
The strengths of our study are that it was a large, population-based sample that allowed for large numbers of observed events that could not be attained in a single-center institution. The primary limitation of the study arises from the characteristics of the dataset, which is based on administrative coding. The risk exists of misclassification as SLE or RA for a patient, both in failing to identify those who may indeed have SLE or RA, or attributing a diagnosis classification in a discharge summary to a person who may have ill-defined disease. In either case, the pattern of misclassification is likely random, and thus may not lead to a systematic bias. Additionally, there is a lack of clinical detail in the administrative database, which limits the analysis of comorbidities, cause of death, and additional clinical factors, including the number of joint replacements done at a specific hospital. Other important limitations are the cross-sectional design of the analyses and the unavailability of longer-term mortality data beyond hospital discharge. Thus we were unable to compute the 30-day or 60-day mortality risk that is customary in studies addressing postoperative risk. Finally, when evaluating such a large number of observations, statistically significant differences may be reported, but clinical significance must be considered.
Patients with SLE undergoing total hip or knee arthroplasty have an increased in-hospital mortality rate compared to all patients and to those with RA. This disparity persists despite adjustments for major medical comorbidities and surgical site. The etiology of this risk is unclear, and further studies are needed to help elucidate the mechanism. Our data indicate that patients with SLE should be carefully evaluated preoperatively, particularly those with chronic renal insufficiency. However, we must not lose sight of the fact that the overall rate of in-hospital mortality, even in patients with SLE, remains low for total knee and hip arthroplasty.
Acknowledgments
The authors thank Molly Vogt, PhD, for her comments on the manuscript.
Footnotes
- Accepted for publication February 17, 2010.








{kind=link}