

Abstract
Objective. To describe the cross-sectional and longitudinal associations between knee regional effusion synovitis and knee pain in older adults.
Methods. Data from a population-based random sample (n = 880, mean age 62 yrs, 50% women) were used. Baseline knee joint effusion synovitis was graded (0–3) using T2-weighted magnetic resonance imaging (MRI) in the suprapatellar pouch, central portion, posterior femoral recess, and subpopliteal recess. Effusion synovitis of the whole joint was defined as a score of ≥ 2 in any subregion. Other knee structural (including cartilage, bone marrow, and menisci) lesions were assessed by MRI at baseline. Knee pain was assessed by the Western Ontario and McMaster Universities Osteoarthritis Index questionnaire at baseline and 2.6 years later. Multivariable analyses were performed after adjustment for age, sex, body mass index, and other structural lesions.
Results. The prevalence of effusion synovitis was 67%. Suprapatellar pouch effusion synovitis was significantly and independently associated with increased total and nonweight-bearing knee pain in both cross-sectional and longitudinal analyses (for an increase in total knee pain of ≥ 5, RR 1.26 per grade, 95% CI 1.04–1.52), and increased weight-bearing knee pain in longitudinal analysis only. Effusion synovitis in posterior femoral recess and central portion were independently associated with increases in nonweight-bearing pain (RR 1.63 per grade, 95% CI 1.32–2.01 and RR 1.29 per grade, 95% CI 1.01–1.65, respectively) in longitudinal analyses only.
Conclusion. Knee joint effusion synovitis has independent associations with knee pain in older adults. Suprapatellar pouch effusion synovitis is associated with nonweight-bearing and weight-bearing knee pain, while posterior femoral recess and central portion effusion synovitis are only associated with nonweight-bearing pain.
Knee pain is one of the most prominent and disabling symptoms of knee osteoarthritis (OA) among older adults. Knee pain is multifactorial, and its risk factors may include body mass index (BMI)1 and knee structural abnormalities such as cartilage defects and bone marrow lesions (BML)2,3, as well as inflammation4. An “inflamed” synovium is indicated by palpable joint swelling, and can arise from synovial thickening or synovial fluid effusion5, both of which may induce knee pain6,7. Although some cross-sectional studies revealed that knee effusion was associated with pain in OA8,9,10,11, only limited cohort studies investigated the associations12,13. It is unknown whether synovial inflammation can cause knee pain independently or through interacting with other structural abnormalities9,14.
Magnetic resonance imaging (MRI) is highly sensitive to detect knee structural abnormalities15 and is able to measure small amounts of intraarticular effusion16,17. Ideally, effusion should be distinguished from synovitis by deploying contrast-enhanced (CE) MRI assessment. Because of the associated cost and potential side effects of contrast agents, non-CE MRI was more widely used in clinical research. Therefore, the phrase “effusion synovitis” has been proposed for the combined measurement of effusion and synovitis18,19. Previous studies have assessed knee synovitis in multiple sites within the whole joint cavity14,20, but not for effusion synovitis on non-CE images. Based on the complex anatomical knee structures and the occurrence and distribution of intraarticular fluid21,22, the synovial lining space of the joint can be divided into 4 subregions: central portion, suprapatellar pouch, posterior femoral recess, and subpopliteal recess23,24. The majority of the effusion is accumulated in the suprapatellar pouch, but it can also be found between femoral and tibial condyles around cruciate ligaments in the central portion, and less commonly in the posterior femoral recess and subpopliteal recess23. So far, the contribution of effusion synovitis in the different subregions to knee pain is unknown. It has been suggested that the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) cannot reflect different pain phenotypes. The weight-bearing items would reflect the pain source from mechanical overload, and nonweight-bearing items may represent biochemical or inflammatory pain25. Thus, a better strategy would be to further investigate specific pain phenotypes. The aim of our study was, therefore, to describe the cross-sectional and longitudinal associations between effusion synovitis and knee pain in older adults.
MATERIALS AND METHODS
Subjects
The Tasmania Older Adult Cohort study is an ongoing prospective, population-based cohort study aimed to identify factors related to the development and progression of OA in older adults. Subjects between the ages of 50 and 80 years were randomly selected from the roll of electors in southern Tasmania (population 229,000), with equal sex proportion. Participants were excluded if they had contraindications to MRI. Baseline data (Phase 1) were collected from February 2002 to September 2004 in 1100 subjects. Followup data (Phase 2) were collected on average 2.6 years (range 1.3–4.8 yrs) later. Those who had self-reported rheumatoid arthritis (RA) were excluded for analyses. Our study was approved by the Southern Tasmania Health and Medical Human Research Ethics Committee, and written informed consent was obtained from all participants.
Anthropometrics and questionnaire
Height and weight were measured according to the protocol described previously26, and BMI was calculated using height and weight (kg/m2).
Knee pain assessment
Self-reported knee pain (walking on flat surface, going up/down stairs, at night in the bed, sitting/lying, and stand upright) was assessed by the knee-specific WOMAC, with a 10-point pain scale from 0 (no pain) to 9 (most severe pain)27. Total pain score (0–45) was created by summing all the subscale scores.
The 5 WOMAC pain subscales were clinically categorized into weight-bearing pain (including pain on flat surface, on stairs, and standing) and nonweight-bearing pain (including pain at night and sitting) as suggested by a previous study25.
Presence of knee pain was defined as a pain score of 1 or greater. Change in knee pain score was calculated as followup value – baseline value, with a change in score of ≥ 1 indicating increased knee pain28. We have calculated the smallest statistically significant difference for the change in total WOMAC knee pain score to be 0.8 for our population, so we defined an increase in pain as a change in score of 1 or greater29.
Radiograph assessment
Knee radiograph was taken on the right knee at baseline. All images were scored by 2 musculoskeletal clinicians (with clinical experience of over 10 yrs) who were blinded to the patients’ information. Each knee joint was scored for osteophytes and joint space narrowing (JSN), on a scale of 0–3 (0 = normal, 3 = severe) according to the Osteoarthritis Research Society International atlas30. The osteophytes and JSN scores were summed to produce a knee total radiographic OA (ROA) score. A total ROA score of 1 or greater is defined as presence of ROA. Interobserver repeatability (weighted κ) was 0.61 for osteophyte and 0.64 for JSN.
Knee MRI measurements
Right knee MRI was performed in the sagittal plane on a 1.5T whole-body magnetic resonance unit (Picker International) using a commercial transmit/receive extremity coil. The MRI sequence protocol included a T1-weighted fat-suppression 3-D gradient-recalled acquisition in the steady state, flip angle 30°, repetition time 31 ms, echo time 6.71 ms, field of view 16 cm, 60 partitions, 512 × 512 pixel matrix, acquisition time 5 min 58 s, 1 acquisition; sagittal images were obtained at a partition thickness of 1.5 mm without a between-slice gap. The MRI also included a T2-weighted fat-suppressed fast spin echo, flip angle 90°, repetition time 3067 ms, echo time 112 ms, field of view 16 cm, 15 partitions, 228 × 256 pixel matrix; sagittal images were obtained at a slice thickness of 4 mm with an interslice gap of 0.5 mm to 1.0 mm26.
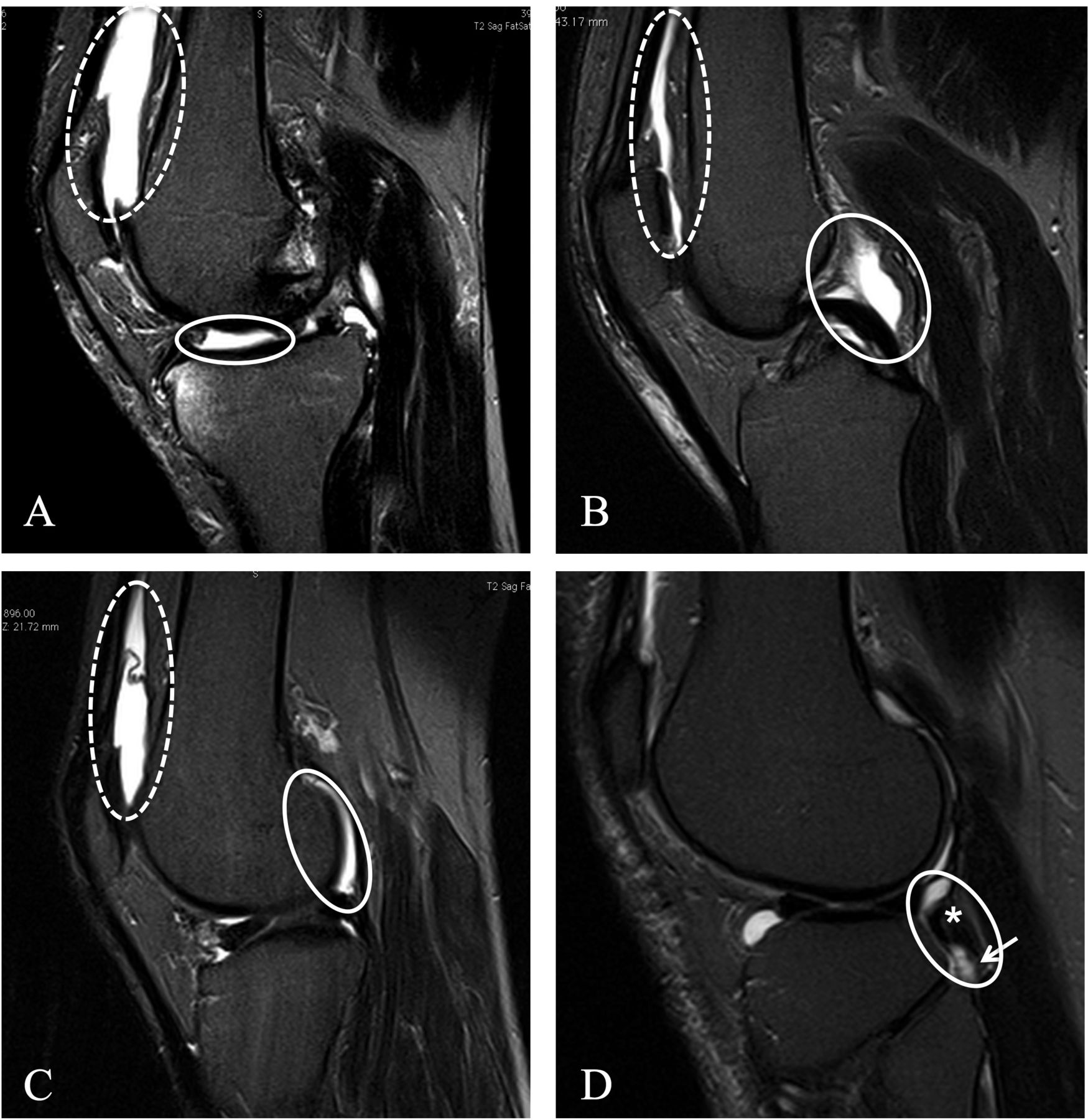
Knee effusion synovitis was assessed as the amount of intraarticular fluid-equivalent signal on T2-weighted MRI (Figure 1) and was scored 0–3 according to the maximum estimated distension of the synovial cavity19. We distinguished knee effusion synovitis in 4 different subregions according to the anatomy of the joint synovial cavity23. They were the suprapatellar pouch: a large pouch formed between the posterior suprapatellar fat pad (quadriceps femoris tendon) and the anterior surface of the femur; central portion: between the central femoral and tibial condyles, around the ligaments and menisci; posterior femoral recess: behind the posterior portion of each femoral condyle and the deep surface of the lateral and medial heads of the gastrocnemius; and subpopliteal recess: lies posteriorly between the lateral meniscus and the popliteal tendon. There was an obvious distention of the synovial cavity when effusion synovitis of Grade 2 was present, so pathological effusion synovitis was defined as any score of ≥ 231. Total effusion synovitis of the whole joint was defined as a score of ≥ 2 in any subregion. Two independent observers who scored all images were blinded to the patients’ information. The intraclass reliability assessed as weighted κ in 50 randomly selected images were 0.63–0.75 in different subregions, and the interclass reliability were 0.65–0.79.
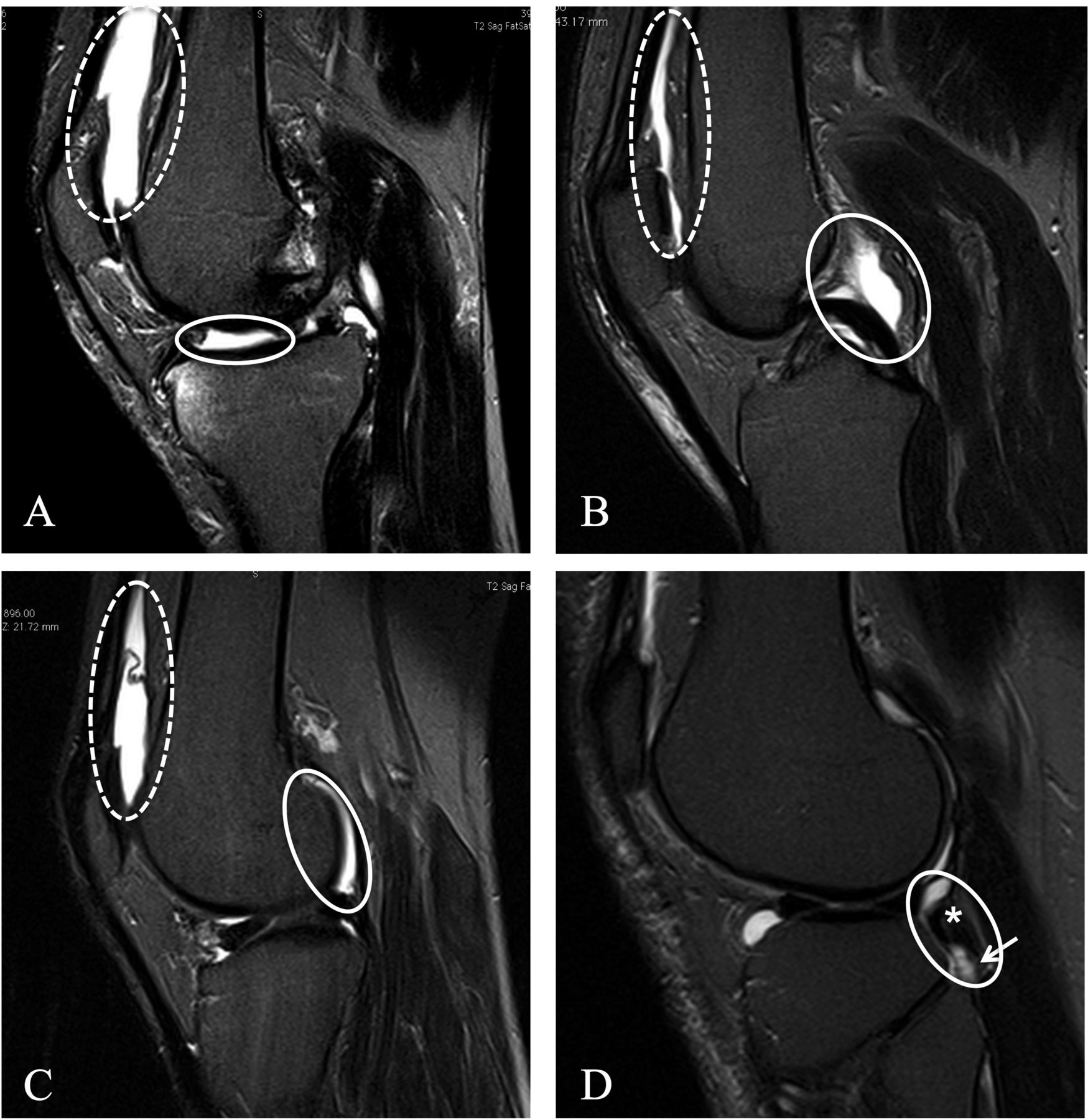
Typical T2-weighted fat-saturation fast spin echo sagittal images for effusion synovitis in different subregions. A. Grade 3 effusion synovitis in the medial suprapatellar pouch (dash circle) and Grade 2 central portion effusion synovitis (solid circle). B. Grade 1 midline suprapatellar pouch effusion synovitis (dash circle) and Grade 2 central effusion synovitis around posterior cruciate ligament (solid circle). C. Grade 2 effusions in the lateral posterior femoral recess (solid circle) and suprapatellar pouch (dash circle). D. Grade 2 subpopliteal effusion synovitis (solid circle) around the popliteal tendon (asterisk), extending to the popliteal bursa (arrow).
Cartilage defects at medial tibial, medial femoral, lateral tibial, lateral femoral, and patellar sites were assessed at baseline on the T1-weighted MR images as follows: Grade 0 = normal cartilage, Grade 1 = focal blistering and intracartilaginous low-signal intensity area with an intact surface, Grade 2 = irregularities on the surface or bottom and loss of thickness < 50%, Grade 3 = deep ulceration with loss of thickness > 50%, and Grade 4 = full-thickness chondral wear with exposure of subchondral bone32,33. Subchondral BML were scored 0–3 as described33. BML was defined as a score of ≥ 1 at any site. The meniscal lesions (tears and extrusion) were scored separately (yes/no) at the anterior horn, body, and posterior horn of medial and lateral menisci. A total meniscal lesion score was summed and the value ranged from 0 to 18 (0–6 for tears, 0–6 for partial extrusions, and 0–6 for full extrusions)34.
Data analysis
Student t tests or chi-square tests were used to compare differences in means or proportions as appropriate. In observational studies, the OR can overestimate prevalence ratio (PR) or relative risk (RR)35. Therefore, univariable and multivariable logistic regression analysis and generalized linear analysis were used to estimate PR or RR for the associations between knee effusion synovitis (0–3) and presence or increases in knee pain36. The analyses evaluated total WOMAC pain, the individual items of the pain scale, and the weight-bearing and nonweight-bearing items. Sensitivity analyses were performed to examine the associations with highest baseline knee pain scores (highest quartile of all pain variables vs other quartiles). We also used alternative thresholds to define a change of ≥ 2 or 3 as an increase in pain in sensitivity analyses. Age, sex, BMI, and ROA were used for adjustment in the multivariable analyses. Structural factors including cartilage defects, BML, and meniscal lesions were further added into the model to determine whether the associations were independent of other structural factors.
A p value < 0.05 (2-tailed) or a 95% CI not including 1 was considered as statistical significance. All analyses were performed on Stata V.12.0 (StataCorp.).
RESULTS
Participants who did not have a knee MRI scan at Phase 1 or who had RA were excluded (n = 220) because our further study aimed to measure structural factors in OA. There were 880 subjects (50% women) included in our study. The average age at baseline was 62 years. There were no significant differences in terms of demographic characteristics between study cohort and those who were excluded (data not shown). Prevalence of knee joint effusion synovitis (≥ 2) was 67% overall (43% in suprapatellar pouch, 49% in central portion, 10% in posterior femoral recess, and 14% in subpopliteal recess). There were 110 individuals (11%) who had effusion synovitis in more than 2 regions. There was 44% of central portion effusion synovitis (≥ 2), 25% of posterior femoral recess effusion synovitis, and 36% of subpopliteal recess effusion synovitis that did not coexist with suprapatellar pouch effusion synovitis.
Characteristics of the subjects are presented in Table 1. Prevalence of knee pain (total score ≥ 1) was 52% at baseline. Subjects with and without baseline knee pain were similar in terms of age, female sex, knee ROA, and meniscal lesions; however, the subjects with baseline knee pain had greater BMI, cartilage defects, and BML, and had greater scores of joint effusion synovitis in all subregions except central portion.
Characteristics of the study sample at baseline. Two-tailed Student t tests are used for differences between means. Chi-square tests are used for percentages. All data presented were from baseline. Values are mean (SD) or percentages unless otherwise specified.
Over 2.6 years, 100 subjects were lost to followup: 28 died, 20 moved, 15 had joint replacement, 28 were physically unable to continue, and others refused or gave no reason. There were no significant differences in baseline characteristics, including age, sex, and disease status, between participants who remained in our study and those who dropped out (data not shown). Subjects experiencing increased (incident or worsening) knee pain (22%) had greater scores of baseline joint effusion synovitis in suprapatellar pouch, posterior femoral recess, and subpopliteal recess, and had higher prevalence of joint effusion synovitis in any subregions (Table 1).
Total knee pain and subscales in cross-sectional associations
Most subregions of effusion synovitis were not significantly associated with the presence of total knee pain (≥ 1; Supplementary Table 1, available from the authors on request); however, subjects with higher effusion synovitis grades in the whole knee, suprapatellar pouch, and subpopliteal recess had a greater total knee pain score of ≥ 5 (highest quartile) in unadjusted analyses (Figure 2A). The associations remained significant after adjusting for age, sex, BMI (but only significant for suprapatellar pouch effusion synovitis after further adjustment for ROA), and structural factors (Table 2). Suprapatellar pouch effusion synovitis was associated with pain on flat surface and at night after adjustment for covariates including structural factors (Table 2). Joint effusion synovitis in central portion and posterior femoral recess were not significantly associated with total knee pain and pain subscales in adjusted analyses (Figure 2A, Table 2).

A. Associations between knee effusion synovitis in different subregions and total knee pain of ≥ 5 at baseline. B. Associations between knee effusion synovitis in different subregions and increases in total knee pain over 2.6 years. Whole effusion synovitis grade (0–3) was defined using the maximal score of subregions. One-way ANOVA were used to test the trend. P values denoting statistical significance at α = 0.05 are in bold face. SP: suprapatellar pouch; CP: central portion; PFR: posterior femoral recess; SPR: subpopliteal recess.
Cross-sectional associations between knee joint effusion synovitis and knee pain at baseline. Dependent variables: knee pain (yes vs no for each pain subscale, total score ≥ 5 vs < 5 for total pain); independent variables: knee joint effusion synovitis (0–3). Values are PR (95% CI).
Weight-bearing and nonweight-bearing knee pain
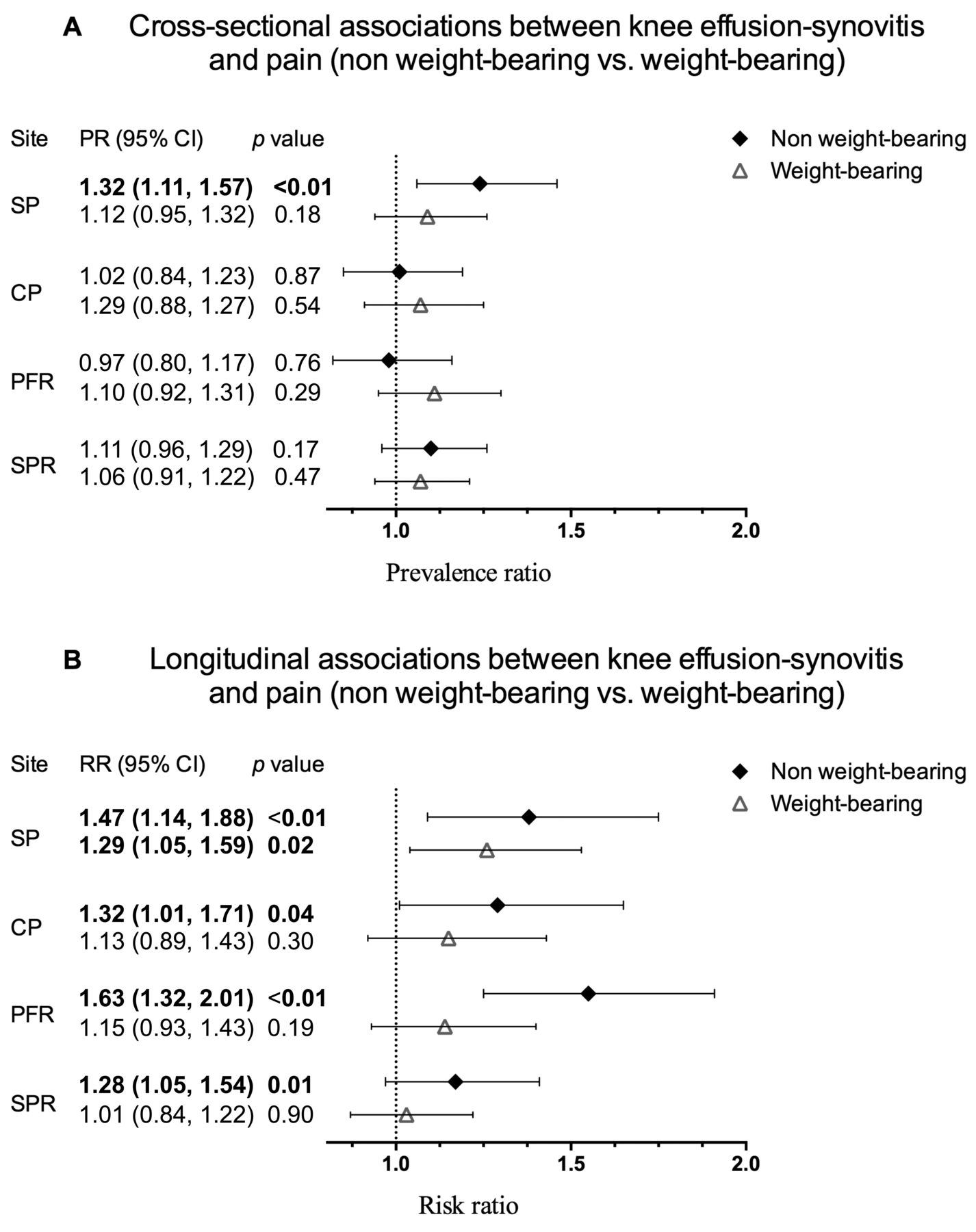
In multivariable analyses, suprapatellar pouch effusion synovitis was not associated with weight-bearing knee pain (Supplementary Table 1 is available from the authors on request), but significantly associated with nonweight-bearing pain of ≥ 1 (PR 1.32, 95% CI 1.11–1.57) and of ≥ 3 (highest quartile; Figure 3A). Every grade increase in the suprapatellar pouch effusion synovitis was associated with 1.32-fold greater PR of nonweight-bearing knee pain of ≥ 3. Effusion synovitis in other locations was not associated with these 2 pain subtypes.

A. Prevalence ratio for associations between knee effusion synovitis in different subregions and weight-bearing/nonweight-bearing pain at baseline. B. Risk ratio for associations between knee effusion synovitis in different subregions and weight-bearing/non-weight-bearing pain over 2.6 years. Adjusted for age, sex, body mass index, radiographic osteoarthritis, bone marrow lesions, cartilage defects, and meniscal lesion. Bars denote 95% CI. Weight-bearing pain was categorized as ≥ 3 and < 3, and nonweight-bearing pain as ≥ 2 and < 2. SP: suprapatellar pouch; CP: central portion; PFR: posterior femoral recess; SPR: subpopliteal recess.
Total knee pain and subscales in longitudinal associations
Joint effusion synovitis scores in the whole knee, suprapatellar pouch, posterior femoral recess, and subpopliteal recess were dose-dependently and significantly associated with an increase in total knee pain over 2.6 years in unadjusted analyses (Figure 2B). These associations remained significant (except for subpopliteal recess) after adjustment for covariates including structural factors (Table 3). Suprapatellar pouch effusion synovitis was significantly associated with most pain subscales (except for pain at night) after adjustment for age, sex, and BMI, and remained significant for pain on flat surface, on stairs, and when sitting after further adjustment for covariates including knee structures (Table 3). Posterior femoral recess effusion synovitis was not significantly associated with pain subscales in the first model, but its associations with pain at night and pain when sitting became significant after further adjustment (Table 3). Central portion effusion synovitis was not significantly associated with increases in total knee pain and knee pain subscales (Figure 2B, Table 3). We also defined change of pain (≥ 2 vs < 2 or ≥ 3 vs < 3) as an increase in knee pain, and found that magnitudes of associations were similar, but the significance decreased because of reduced sample size in those with knee pain (Supplementary Table 2, Supplementary Table 3, available from the authors on request).
Longitudinal associations between knee joint effusion synovitis and knee pain. Dependent variables: knee pain (change of 0 vs ≥ 1 for pain); and independent variables: knee joint effusion synovitis (0–3). Values are RR (95% CI).
Weight-bearing and nonweight-bearing knee pain
In multivariable analyses (Figure 3B), suprapatellar pouch effusion synovitis was significantly associated with both increased nonweight-bearing and weight-bearing pain. Every grade increase in suprapatellar pouch effusion synovitis was associated with 1.47 and 1.29 greater risk, respectively, of increase in nonweight-bearing and weight-bearing knee pain over time. Central portion and posterior femoral recess effusion synovitis were only significantly associated with nonweight-bearing pain. No significant association was found for subpopliteal recess.
DISCUSSION
To the best of our knowledge, our study is the first to examine the cross-sectional and longitudinal associations between knee effusion synovitis at different sites and knee pain in older adults. We found that suprapatellar pouch effusion synovitis had the most consistent association with knee pain, followed by posterior femoral recess effusion synovitis. In contrast, central portion and subpopliteal recess effusion synovitis were not consistently associated with knee pain. Moreover, knee effusion synovitis was more consistently associated with nonweight-bearing than weight-bearing knee pain.
Usually, knee joint effusion synovitis was only assessed in the suprapatellar pouch. It can be evaluated by radiograph by measuring the widest anterior-posterior diameter of the lateral suprapatellar pouch37, which is the largest recess of the joint with a great degree of stretch38. However, only a moderate amount of suprapatellar effusion synovitis can be diagnosed by radiographs39, and MRI is a more accurate modality that can delineate all compartmental effusion synovitis. In our study, we found that joint effusion synovitis was more common in the central portion and suprapatellar pouch than posterior femoral recess and subpopliteal recess, which is consistent with previous reports23. Although these synovial spaces were interconnected, we found that 25% to 44% of the effusion synovitis in other sites was independent of suprapatellar effusion synovitis, suggesting that these regional effusion synovitis sites can be missed if we only assess the suprapatellar pouch in traditional clinical examinations.
Previous cross-sectional studies reported that prevalence of effusion synovitis was significantly greater in patients with symptomatic knee OA8,40,41,42. Besides, abnormal effusion synovitis was more frequently observed in OA with the knee pain group than without pain in middle-aged women43, but nonsignificant association between joint effusion synovitis and knee pain were found in patients with OA44. A recent study reported that synovitis at 7 sites (mainly medial parapatellar involvement), but not other sites (mainly site adjacent to the anterior cruciate ligament, loose bodies), was associated with increased knee pain45. A longitudinal study reported that change of effusion was not associated with change in knee pain over 30 months12. Knee joint effusion synovitis was not associated with frequent knee pain, but significant association was found between change in effusion synovitis severity and knee pain fluctuation in patients with ROA15. The reasons underlying these discrepancies are unclear, but they may exist because of the variations in study design, sample size, study populations, and/or durations of followup. In our current study with both cross-sectional and longitudinal designs, we found consistent association between joint effusion synovitis in the suprapatellar pouch and knee pain, supporting the clinical relevance of effusion synovitis in this compartment. Effusion synovitis per grade in the suprapatellar pouch was associated with 33% increased prevalence (≥ 5) and 26% progression of total knee pain, which are quite evident considering that the overall prevalence of knee pain ≥ 5 was 24% and the increase of knee pain was 22% in this sample. This may indicate that the effusion synovitis from MRI is an indicator of clinical OA severity.
While Lo, et al reported that the effusion synovitis score was associated with weight-bearing knee pain but not nonweight-bearing pain9, we found that suprapatellar pouch effusion synovitis was associated with both nonweight-bearing and weight-bearing knee pain, and posterior femoral recess effusion synovitis was only associated with nonweight-bearing knee pain. Central portion effusion synovitis was weakly but significantly associated with an increase in nonweight-bearing knee pain. These suggest that the suprapatellar effusion synovitis may induce knee pain through both mechanical and inflammatory mechanisms. Because of the limited spaces in other subregions, the location-specific effusion synovitis may cause nonweight-bearing knee pain through the inflamed synovium rather than mechanical stretching by excessive synovial effusion. Further, all these associations were independent of ROA, and other abnormal knee structural changes. In contrast, the significant association between subpopliteal recess effusion synovitis and knee pain was not independent of ROA and other abnormal knee structural changes. Our results indicate that effusion synovitis in posterior femoral recess and central portion may also have clinical use in predicting symptomatic OA.
We found a dose-response relationship between effusion synovitis score and increase in total knee pain, particularly for total joint and suprapatellar pouch. Previous studies tried to set thresholds of joint effusion by measuring the diameter or depth of suprapatellar pouch effusion on lateral knee radiograph39, sagittal plane of MRI46, or ultrasound47; however, these thresholds were arbitrary and only single dimensional distance was measured in 1 location of knee joint (mainly the suprapatellar pouch). It is very difficult to define a threshold between “physiological” and “pathological” using semiquantitative approaches. In fact, there was a very small number of participants whose effusion synovitis scores were 0 in our cohort (3 in total joint, 20 in suprapatellar pouch, and 31 in central portion). For this reason, it seems appropriate to use a more conservative definition for disease or pathology than we have in our current study. Besides, we found that an effusion synovitis score of 2 and greater was associated with more increases in knee pain, suggesting that it may be pathological. Our current study establishes the groundwork for further quantitative measurement of knee joint effusion synovitis in multiple subregions.
The strength of our study is that we performed both cross-sectional and longitudinal analyses in a community-based population with a large sample size. There are potential limitations in our study. First, the response rate at baseline was 57%, but there were no significant differences in baseline characteristics between those who responded and those who did not. Second, traumatic injury and other reasons such as infection, crystal-induced arthropathies, and tumor can also cause effusion and pain, but those are rare situations in our population-based cohort. Third, we did not assess synovitis at some sites (e.g., Hoffa’s fat pad) that may be associated with knee pain. Lastly, we only had a standing anterior-posterior semiflexed view of the right knee, so we were unable to detect the diameter of joint effusion in the suprapatellar pouch from radiographs.
Knee joint effusion synovitis has independent contributions to knee pain in older adults. While suprapatellar pouch effusion synovitis is associated with both nonweight-bearing and weight-bearing knee pain, posterior femoral recess and central portion effusion synovitis are only associated with nonweight-bearing knee pain.
Acknowledgment
We especially thank the participants who made our study possible, and we gratefully acknowledge the role of the Tasmania Older Adult Cohort staff and volunteers in collecting the data, particularly research nurses Catrina Boon and Pip Boon. We also thank Dr. Velandai Srikanth and Dr. Helen Cooley for assessing the radiographs.
Footnotes
Funded by the National Health and Medical Research Council of Australia (302204), the Tasmanian Community Fund (D0015018), the Arthritis Foundation of Australia (MRI06161), and the University of Tasmania Grant-Institutional Research Scheme (D0015019).
- Accepted for publication August 27, 2015.








{kind=link}
{kind=link}
{kind=link}