

Abstract
Objective. To evaluate the rate of inactive disease in children with juvenile idiopathic arthritis (JIA) treated with etanercept, and to identify clinical characteristics associated with attainment of inactive disease.
Methods. Clinical charts of patients who were given etanercept between January 2002 and January 2011 were evaluated retrospectively. For each patient, all visits from initiation of etanercept to the last followup evaluation in which the patient was still receiving etanercept were examined to establish whether the patient had reached the state of inactive disease and to identify the first visit in which inactive disease was documented. Clinical characteristics associated with achievement of inactive disease were determined through univariate analyses and Cox regression procedures.
Results. A total of 173 patients who received etanercept for a median of 2.2 years (range 0.5–10.5 yrs) were studied. Eighty-seven patients (50.3%) achieved inactive disease after a median of 0.6 years (range 0.1–2.5 yrs) of therapy. At last followup evaluation, 85 patients (49.1%) still had inactive disease and 70 (40.5%) were in clinical remission on medication. The probability of achievement of inactive disease after 6, 12, and 24 months of therapy was 24%, 46% and 57%, respectively. On Cox regression analysis, the attainment of inactive disease was associated with lack of wrist involvement and an age at disease onset < 3.6 years.
Conclusion. Around half of our patients with JIA treated with etanercept achieved a state of inactive disease. Children who lacked wrist involvement and were younger at disease onset had a greater likelihood of achieving inactive disease.
The advent of new therapies for juvenile idiopathic arthritis (JIA), particularly the introduction of biologic medications, has increased considerably the potential for treatment benefit, with clinical remission being now a realistic goal for a substantial proportion of patients1,2,3,4. These advances have led to a shift in the aim of therapy increasingly toward the attainment of complete disease quiescence5,6,7,8,9,10. Further, they have led to the view that in chronic arthritis clinical trials, it is important not only to know the magnitude of clinical improvement from baseline, but also to understand whether the therapeutic agent under study is able to achieve more pronounced levels of improvement, including a state of inactive disease8,10.
However, none of the registration trials of biologic agents in JIA to date has included inactive disease as primary endpoint. The preliminary definition of inactive disease in JIA5,6 has been used as a primary outcome measure in a randomized, double-blind, placebo-controlled trial of 2 aggressive treatment strategies in children with early JIA11. Nevertheless, to gain further insight into the therapeutic efficacy of biologic medications there is a need to obtain information about their potential to induce clinical remission in standard clinical practice. Further, it would be desirable to identify factors associated with therapeutic response or nonresponse, to optimize the current therapeutic approaches.
Etanercept, a tumor necrosis factor-α (TNF-α) antagonist, has been the first biologic agent registered for use in children with JIA. The efficacy and safety of this medication have been established in a randomized placebo-controlled withdrawal trial in patients with a polyarticular disease course who were refractory or intolerant to methotrexate12. Longterm extension studies of the original trial cohort and several national registries have subsequently confirmed the sustained clinical benefit and acceptable safety profile of the drug13,14,15. The evidence for the effectiveness of etanercept in JIA has been expanded by the observation that its administration may be associated with improvement of functional ability and quality of life16,17, recovery of growth velocity and bone status18,19, and reduction in the progression of radiographic joint damage20. However, the potential of etanercept to induce disease remission and the clinical features associated with treatment effectiveness have seldom been investigated21,22.
The primary objective of our study was 2-fold: first, to evaluate the proportion of children with JIA treated with etanercept who reached the state of inactive disease; and second, to identify clinical characteristics associated with attainment of inactive disease.
MATERIALS AND METHODS
Study design and patient selection
All consecutive patients who met the International League for Associations of Rheumatology (ILAR) criteria for JIA23 who were given etanercept at the study center between January 2002 and January 2011, and who had a minimum followup of 6 months after start of etanercept, were included in the study. The analysis was conducted through retrospective review of patient clinical charts and data stored in clinical databases. Patient information was collected by means of standardized case report forms and was entered in a specialized database. The study protocol was approved by the medical ethics committee at the Istituto G. Gaslini, Genoa, Italy.
Protocol of etanercept administration
All patients received etanercept subcutaneously at a dose of 0.8 mg/kg/week (maximum 50 mg). In the earlier years, the weekly dose was fractioned in 2 weekly administrations of 0.4 mg/kg (maximum 25 mg) in all patients. More recently, the weekly dose was mostly delivered in a single administration, using 25 or 50 mg vials, depending on child’s weight. During etanercept therapy, patients were evaluated clinically every 3 to 6 months. Laboratory monitoring was carried out every 8–12 weeks.
Assessment of inactive disease
For each patient, all visits from the start of etanercept therapy to the last followup evaluation in which the patient was still receiving etanercept were examined to establish whether the patient had achieved the state of inactive disease. In case the attending physician had started to decrease the weekly dosage or space dosing further apart before the last followup visit because of achievement of inactive disease, the last observation in which the patient was still receiving the standard dose of 0.8 mg/kg/week was retained as the last followup visit. In patients who achieved inactive disease, the first visit in which inactive disease was documented was identified. The state of inactive disease was defined, according to Wallace criteria5, as no joint with active arthritis, no systemic manifestations attributable to JIA, no active uveitis, normal acute-phase reactants, and physician’s global assessment of disease activity indicating no disease activity (defined as score of 0 on a 0–10 visual analog scale). The state of clinical remission on medication was assessed in all patients with inactive disease at last followup visit and was defined as a period of 6 continuous months of inactive disease while the patient was still receiving etanercept5.
Assessment of predictive factors
The following independent (predictor) variables were recorded: sex, age at disease onset, age and disease duration at treatment baseline, interval between first observation at study center and start of etanercept, ILAR category, antinuclear antibody (ANA) status (defined as reported24), JIA outcome measures at start of etanercept (Table 1), joints affected before start of etanercept, and medications administered before start of etanercept and administered concomitantly during etanercept therapy, including intraarticular corticosteroid injections.
Demographic, clinical, and therapeutic characteristics of patients with juvenile idiopathic arthritis treated with etanercept. Data are numbers (percentages) unless otherwise indicated.
Statistics
Descriptive statistics were reported as medians and interquartile ranges for continuous variables and as absolute frequencies and percentages for categorical variables. Comparisons between patients who did or did not achieve inactive disease were by Mann-Whitney U test in case of quantitative data and chi-square test or Fisher’s exact test, as appropriate, for categorical data.
Predictive factors were tested for association with the achievement of inactive disease during the time of observation. For each category of predictive factor tested, the number of patients with inactive disease, the time of observation (person-years), and the incidence rate of inactive disease per 100 person-years were calculated and compared by means of bivariate analyses. Factors significantly associated with inactive disease were then tested in a Cox proportional hazards regression model. The log-rank test was used for comparisons. Survival analysis, with the state of inactive disease as the event of interest, was conducted by Kaplan-Meier method25. Survival curves were compared by the log-rank test.
The statistical packages used were Statistica (version 9.0, StatSoft Corp.) for bivariate analyses and Stata (release 7, Stata Corp.) for multivariate analyses.
RESULTS
Patient characteristics
A total of 187 patients were treated with etanercept in the study period. Fourteen patients were excluded from the analysis because the clinical chart could not be retrieved or the followup period after start of etanercept was shorter than 6 months. The main demographic and clinical features of the remaining 173 patients are presented in Table 1. Patients had on average a longer disease duration (median 5 yrs), although the median time interval between first observation and etanercept start was 3 years. The total duration of etanercept therapy was 458.8 patient-years, with a median treatment duration of 2.2 years per patient. The total number of clinic visits during etanercept therapy was 1142, with a median of 5 visits per patient. The most frequent ILAR category was extended oligoarthritis, followed by rheumatoid factor-negative polyarthritis; 15.6% of patients had systemic arthritis. Around two-thirds of patients were ANA-positive. The median number of active joints at start of etanercept was 5. The knee and ankle were the most frequently affected joints, followed by the hand and wrist joints.
Before start of etanercept, almost all patients had received methotrexate, 72.3% of patients had undergone intraarticular corticosteroid injections, and 40.5% of patients had received systemic corticosteroids. Concomitant medications administered during etanercept therapy included methotrexate in 67.1% of patients, intraarticular corticosteroids in 22%, and systemic corticosteroids in 13.9%.
Frequency of achievement of inactive disease
Eighty-seven patients (50.3%) achieved inactive disease a median of 0.6 years (range 0.1–2.5 yrs) after initiation of etanercept therapy. The rate of inactive disease was much lower in children with systemic arthritis than in those with nonsystemic categories altogether (29.6% vs 54.1%, respectively). At last followup visit, 0.5 to 10.5 years after etanercept start (median 2.2 yrs), 85 patients (49.1%) still had inactive disease and 70 (40.5%) met the criteria for clinical remission on medication. The probability of achievement of inactive disease after 6, 12, and 24 months of therapy was 24%, 46%, and 57%, respectively.
Comparison of clinical characteristics between patients with and without inactive disease
Characteristics of patients who achieved or did not achieve inactive disease are compared in Table 1. Patients with inactive disease belonged more frequently to the extended oligoarthritis and enthesitis-related arthritis categories and less frequently to the systemic arthritis category than did patients without inactive disease. Further, patients with inactive disease had a lower frequency of wrist involvement at the start of etanercept, had less often received systemic corticosteroids before starting etanercept, and had more frequently undergone intraarticular corticosteroid injections during etanercept administration than did patients without inactive disease. The same comparison was made after the exclusion of the 27 children with systemic arthritis. In this analysis, the differences regarding ILAR category, corticosteroid therapy before start of etanercept, and intraarticular corticosteroid injections during etanercept administration were no longer detected, whereas patients with inactive disease still had a lower frequency of wrist involvement at start of etanercept than patients without inactive disease (30.4% and 50.7%, respectively; p = 0.012). Unlike the observations from the entire sample, patients with inactive disease had a younger age at disease onset than patients without inactive disease (median ages 2.8 yrs and 4.5 yrs, respectively; p = 0.046). Among the 27 patients with systemic arthritis, those with inactive disease (n = 8) had a longer disease duration than those without inactive disease (n = 19), with median disease durations of 6.6 years and 2.1 years, respectively (p = 0.003), and they were older at etanercept initiation, with median ages of 11.8 years and 7.3 years, respectively (p = 0.029).
Factors associated with achievement of inactive disease
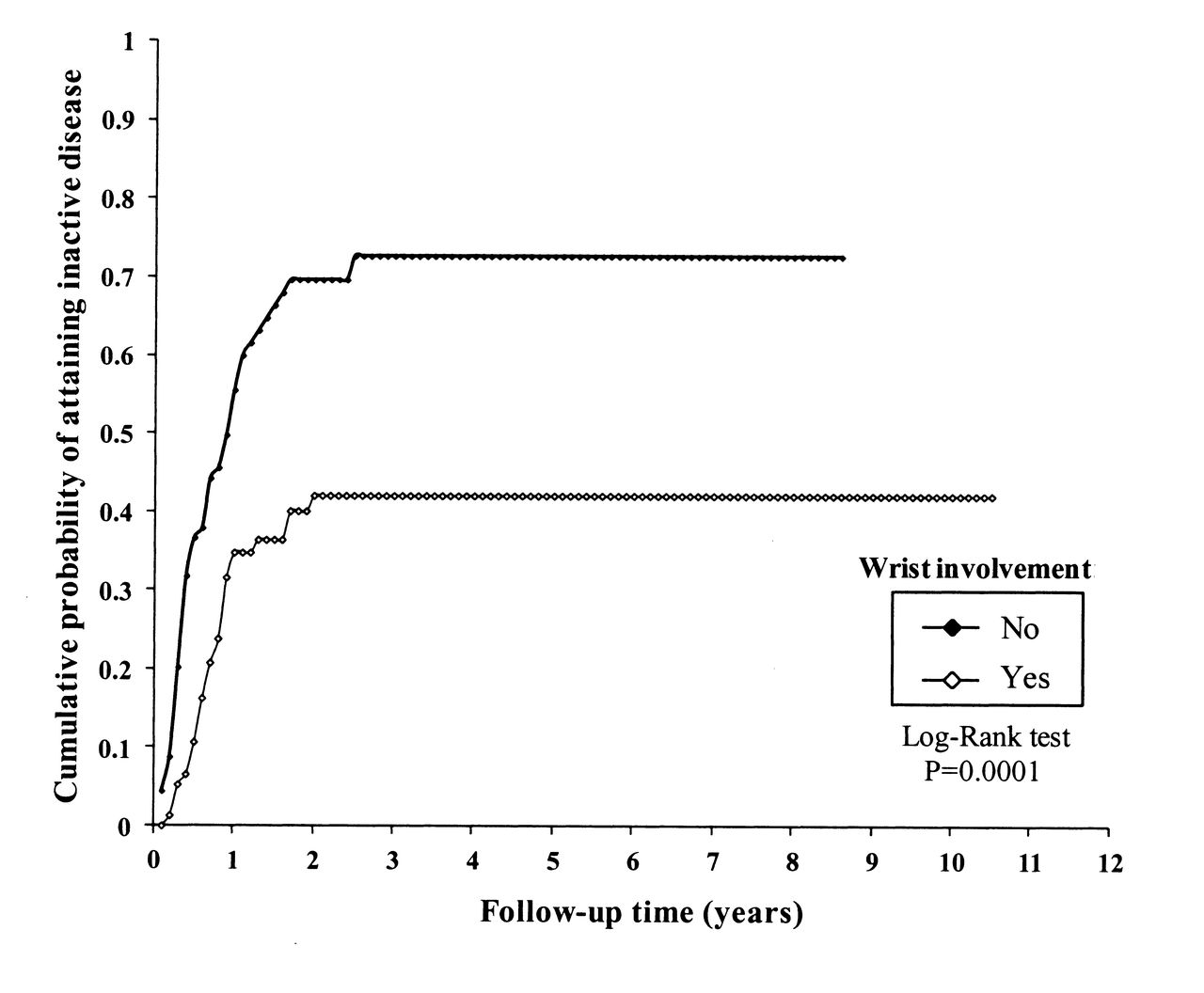
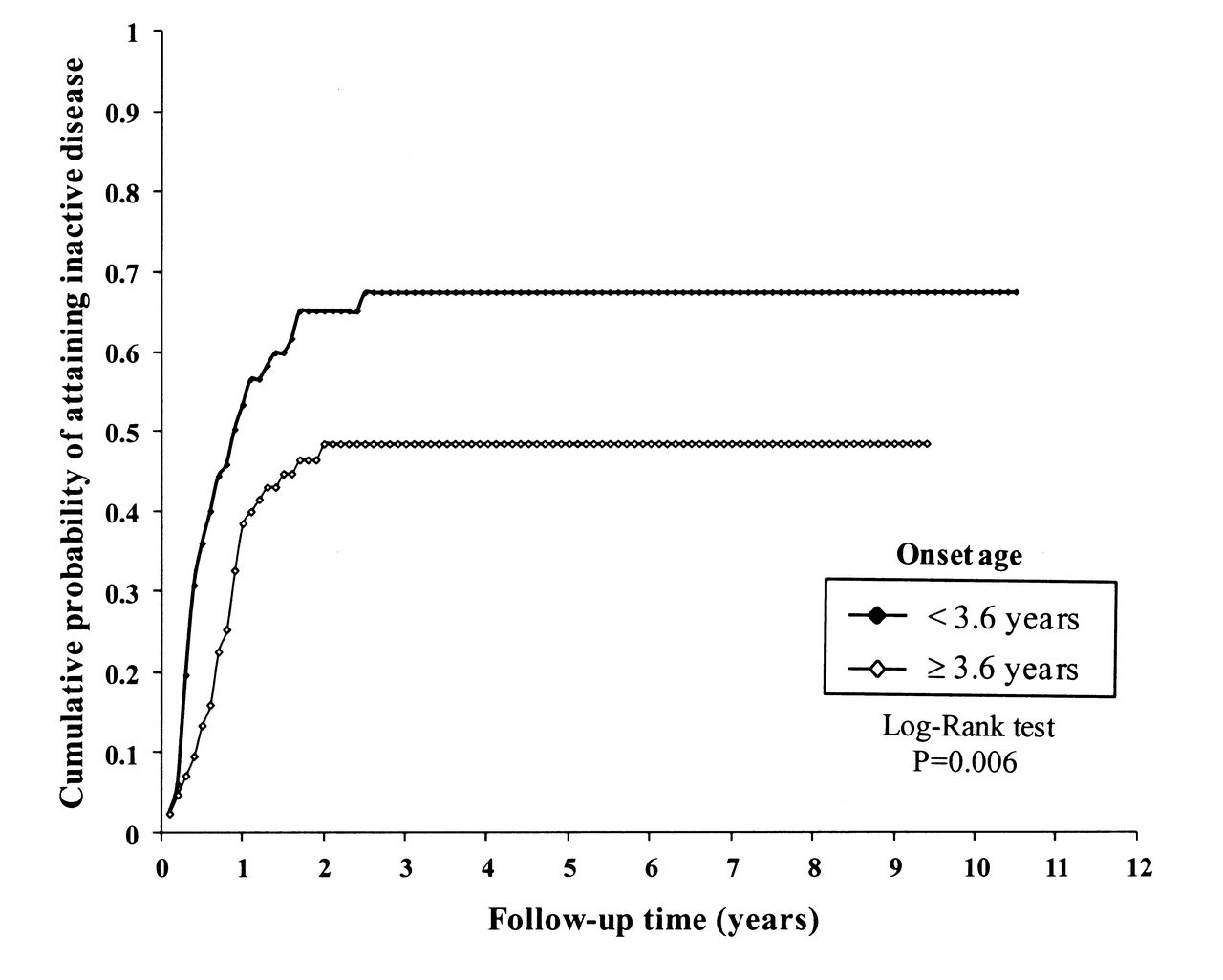
For each patient and category of predictive factors tested for their association with inactive disease, Table 2 presents the number of patients in the predictive factor category out of the total number of patients with inactive disease, the time to inactive disease expressed in terms of person-years, and the incidence rate of inactive disease. Factors associated with achievement of inactive disease were age at disease onset younger than 3.6 years, a physician global rating < 6, the absence of wrist disease, the lack of use of systemic corticosteroids before the start of etanercept, and the lack of administration of intraarticular corticosteroids during etanercept therapy. When all these variables were included in a Cox proportional hazards regression model, the age at disease onset younger than 3.6 years and the absence of wrist disease were the only variables associated with the attainment of inactive disease (Table 3). A secondary analysis after the exclusion of the 27 children with systemic arthritis identified the same predictors (Table 3).
Patient and disease characteristics tested for association with achievement of inactive disease state.
Best-fitting model obtained through Cox proportional hazards regression procedures in all patients and in patients who did not have systemic arthritis. Achievement of inactive disease status was the dependent variable.
The survival analysis, with the state of inactive disease as the event of interest, in the entire patient sample and in patients who did or did not have the 2 risk factors that were significantly associated with inactive disease in the Cox regression model is presented in Figures 1, 2, and 3, respectively.

Cumulative probability of attaining state of inactive disease in the entire patient sample; Kaplan-Meier method.

Cumulative probability of attaining state of inactive disease by absence or presence of wrist involvement; Kaplan-Meier method.

Cumulative probability of attaining state of inactive disease by age at onset < 3.6 or ≥ 3.6 years; Kaplan-Meier method.
Drug discontinuation and adverse events
After the last followup evaluation, 137 patients were maintained on etanercept therapy, whereas 36 patients were discontinued. The reasons for discontinuation were inefficacy (14 patients), remission (11), side effects (10), and lack of compliance (1 patient). Adverse events observed during etanercept administration included new-onset iridocyclitis (6 patients), leukopenia (3), thrombocytopenia (1), injection-site reactions (2), urticaria/angioedema (3), and papilledema (1 patient). Serious infections included varicella complicated by bronchopneumonia (1 patient) and tuberculosis (1 patient); 1 patient died of a streptococcal sepsis.
DISCUSSION
We evaluated the frequency of achievement of inactive disease in 173 children with JIA treated with etanercept in standard clinical care. We found that 50.3% of patients achieved inactive disease a median of 0.6 years after the initiation of etanercept therapy. At last followup visit, after a median of 2.2 years from start of etanercept, 49.1% of patients still had inactive disease and 40.5% met the criteria for clinical remission on medication (i.e., they had been in the state of inactive disease for at least 6 months while taking etanercept). The probability of achieving the inactive disease state after 6, 12, and 24 months of therapy was 24%, 46%, and 57%, respectively.
The prevalence of inactive disease in JIA patients treated with etanercept was evaluated in 2 previous studies, both based on national registries. In the German registry, 47.6% and 26.6% of 787 patients reached the criteria for inactive disease or clinical remission on medication, respectively21. Among 262 patients included in the Dutch registry, the frequency of excellent response, defined as fulfillment of adapted inactive disease criteria, was 32% after 15 months of therapy. This rate increased to 37%–49% in a secondary longer-term followup analysis, 4 to 7 years after initiation of etanercept22. Together, the results reported in national registries and those from our study indicate that around half of children with JIA who are treated with etanercept in real-life clinical settings are able to attain complete disease quiescence.
In our study, the lack of involvement of the wrist joint was the clinical characteristic most strongly associated with achievement of inactive disease in Cox regression analysis. This observation implies that wrist disease is a marker of poorer therapeutic outcome in children with JIA treated with etanercept. Previous studies have shown that JIA patients with wrist disease are at high risk of developing structural joint damage26,27,28, a more severe course of arthritis29,30, or a poorer functional outcome31, and have a lesser likelihood of experiencing a therapeutic response to methotrexate32,33. Thus, the presence of arthritis in the wrist joint might identify a subgroup of patients with JIA who deserve earlier introduction of etanercept during their disease course or administration of etanercept in combination with methotrexate. Horneff, et al34 reported a greater frequency of therapeutic response in patients treated with etanercept and methotrexate in combination than in patients who received etanercept monotherapy. Unlike that study, we did not find an association between achievement of inactive disease and concomitant methotrexate administration. However, this observation should be regarded with caution as it was made in the context of a retrospective analysis. The role of methotrexate in enhancing etanercept’s effectiveness needs to be examined in a controlled trial.
The only other factor that was associated with inactive disease in Cox regression procedures was an age at disease onset younger than 3.6 years. Younger age at disease presentation was also associated with excellent response to etanercept in the Dutch registry22, but was not among the determinants of inactive disease in the German registry21. This discrepancy may depend, at least in part, on disparities in patient characteristics, including demographic features, level of disease activity, and distribution of JIA categories. Notably, our patient population had a much younger age at disease onset and included a greater percentage of children with positive ANA status and extended oligoarthritis than the patient samples in the German and Dutch registries.
Several studies, including the 2 registry reports, have shown that anti-TNF agents are less effective in the systemic subset of JIA13,14,21,22,35,36,37,38. This phenomenon has been attributed to interleukin 1 (IL-1) and IL-6 playing a greater pathogenetic role than TNF-α in systemic arthritis39,40. In accord with these observations, the rate of inactive disease was much lower in our children with systemic arthritis than in those with nonsystemic categories altogether (29.6% vs 54.1%).
We recognize the limitations of the retrospective and noncontrolled design of our study. A retrospective analysis is subject to missing possibly erroneous data. We also acknowledge that the lack of data regarding parent-reported outcomes, namely overall well-being, pain, and functional ability assessments, in a number patients precluded a meaningful analysis of their predictive value. The state of inactive disease was not confirmed with imaging studies. Recently, synovial pathology detected by magnetic resonance imaging or ultrasound, possibly reflecting continuing active disease, has been found in a sizable percentage of children with clinically defined inactive disease41,42,43. We did not investigate the rate of disease relapse after discontinuation of etanercept. It is our current policy to continue etanercept at standard dose for 1 year after the occurrence of inactive disease and then to taper it gradually until discontinuation in another year.
Around half of our JIA patients treated with etanercept in standard clinical care were able to achieve the state of inactive disease. Children who lacked wrist involvement and had a younger age at disease onset had a greater likelihood of achieving inactive disease during etanercept administration. Thus, the presence of wrist disease and older age at disease presentation may constitute an indication for earlier introduction of etanercept or its administration in combination with methotrexate.
Footnotes
-
Supported in part by an educational grant from Pfizer (formerly Wyeth).
- Accepted for publication October 9, 2012.








{kind=link}
{kind=link}
{kind=link}