

Abstract
Objective. Multimorbidity, the coexistence of 2 or more conditions in an individual, is associated with morbidity and mortality in the general population. This study aims to describe the prevalence of multimorbidity in axial spondyloarthropathy (axSpA) and assess its association with disease outcome measures.
Methods. This cross-sectional study was conducted within the Ankylosing Spondylitis Registry of Ireland (ASRI) cohort. Structured standardized assessment was performed. Multimorbidity was considered as the presence of at least 1 physician-diagnosed chronic condition (excluding extraarticular manifestations) in addition to axSpA. Validated outcome measures were collected: Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), Bath AS Functional Index (BASFI), Health Assessment Questionnaire (HAQ), AS Quality of Life (ASQoL), and Bath AS Metrology Index (BASMI). Adjusted multiple regression was performed to investigate the association between multimorbidity and disease outcomes.
Results. A total of 734 patients from 12 centers were included: 77% male, mean (SD) age 45 (12) years. Of the cohort, 55% (n = 403) were multimorbid. Multimorbid patients were significantly (p < 0.01) older than axSpA-only patients [50 (12) vs 40 (11) yrs]. Obesity was the most prevalent chronic condition, affecting 27%. Multimorbid patients had more severe disease than patients with axSpA only. After adjusting for confounders, multimorbidity was associated with higher BASDAI (ß 0.7, 95% CI 0.34–1.05), BASMI (ß 0.45, 95% CI 0.09–0.80), BASFI (ß 0.5, 95% CI 0.23–0.78), HAQ (ß 0.07, 95% CI 0.00–0.13), and ASQoL (ß 0.87, 95% CI 0.28–1.46).
Conclusion. Multimorbidity is prevalent in axSpA and is associated with more severe disease.
The dramatic increase in life expectancy of modern times is an important accomplishment1,2. Population growth has been accompanied by many challenges3,4, including projected increases in age-related expenditure and associated economic burden. A simple aspiration to live longer is no longer the goal. A delayed onset of morbidity and functional decline, termed compression of morbidity5, is now the ambition, where people live longer but with less chronic disease. Unfortunately, it appears that old age is instead accompanied by a greater disease burden6, in particular noncommunicable diseases, which are now the biggest threats to mortality worldwide7.
To cope with aging populations, health systems must adapt3. Current clinical practice guidelines focus on individual comorbidities, without giving adequate guidance on managing patients with multiple chronic conditions8. However, with pressure to delay the onset of functional decline and to allow people to remain effective members of society for longer, swapping the concept of comorbidity for multimorbidity is needed8. Multimorbidity shifts our focus from a narrow view of considering each condition in isolation to a more holistic approach, whereby the patient is considered as the center of care and all aspects of their condition are considered together8,9.
Although the definition can vary, multimorbidity is widely accepted as the presence of 2 or more chronic conditions in 1 individual, without specifying the index disease10. Multimorbidity estimates range from 13% to 95%, with prevalence increasing with age11,12. Multimorbid patients have increased mortality, more disability, worse quality of life, and greater use of healthcare resources13,14,15; in some cases, 25% of the population accounts for more than 50% of healthcare use15. Musculoskeletal disease (MSD) is common in multimorbidity patterns16 and serves to intensify the effect17,18.
In rheumatoid arthritis (RA), 62–65% of patients are multimorbid19,20. Multimorbid patients with RA have worse physical function9 and lower rates of disease control21.
A growing body of work has examined the burden of comorbidities in axial spondyloarthritis (axSpA)22,23,24,25,26. Mortality is known to be increased in axSpA patients compared to age- and sex-matched controls25,26,27. The Assessment of Spondyloarthritis international Society-COMOrbidities in SPondyloArthritis (ASAS-COMOSPA) study23 has outlined the comorbidity profile of patients with axSpA, particularly highlighting the frequency of osteoporosis and peptic ulcer disease. Cardiovascular-related comorbidity is also more prevalent in AS28,29. Comorbidity adds to the burden of disease in patients with SpA, reducing physical function and quality of life24. ASAS/European League Against Rheumatism recommendations for management of axSpA suggest that treatment should be tailored to take comorbidities into consideration30, but no specific guidelines are available. However, little is known about the burden of multimorbidity in axSpA, despite recognition that better knowledge of multimorbidity is crucial to allow sustainable models of care to be established8. In modern society, increasing emphasis is being placed on compression of morbidity; therefore, it is important to understand the effect of multimorbidity in patients with axSpA. To our knowledge, there is no literature looking at the prevalence of multimorbidity and associated relationships in patients with axSpA.
Therefore, the aims of our study are to determine (1) the prevalence of multimorbidity within a well-characterized real-life axSpA cohort, and (2) relationships between multimorbidity and disease outcomes.
MATERIALS AND METHODS
Ankylosing Spondylitis Registry of Ireland (ASRI) study design and patient recruitment
This study was conducted within the framework of the ASRI cohort. ASRI is a large observational cross-sectional multicenter cohort study, which is ongoing. It was established in 2013, with the primary objective to measure the burden of axSpA disease in the Irish population and identify predictors of poor disease outcome.
Consecutive patients are invited to partake in ASRI if they have a clinical diagnosis of axSpA, made by a rheumatologist, and have attended secondary or tertiary care in the preceding 3 years. Patients are excluded if they have cognitive or other impairment that prohibits informed consent. Each center has a designated subinvestigator with responsibility for local oversight. Accuracy of the data collected is monitored quarterly by (author) PG. The primary investigator (author FOS) has responsibility for overall oversight of the database. To date, 12 centers in Ireland have recruited patients and contributed data to ASRI.
Written informed consent was obtained from all patients. Ethical approval was originally obtained from the Tallaght University Hospital/St. James’s Hospital Joint Research Ethics Committee (REC reference: 2013/21/06) and was subsequently approved in each participating center.
Data collection
A trained study investigator collected data according to a standard protocol in a structured face-to-face visit. The medical record was reviewed as required to obtain information not available directly from the patient. The following data were entered into an electronic centralized report form:
Demographics: age, sex, ethnicity, marital status, employment status, alcohol intake, smoking status (current/past/never), family history of SpA (AS, axSpA, psoriasis, or psoriatic arthritis).
Disease characteristics: age of symptom onset, duration of disease, delay to diagnosis, history of extraarticular manifestations [EAM; uveitis, psoriasis, inflammatory bowel disease (IBD)], other SpA features (enthesitis, dactylitis, peripheral arthritis), current and previous treatment (nonsteroidal antiinflammatories, methotrexate, sulfasalazine, biologics), HLA-B27 status, highest recorded erythrocyte sedimentation rate (ESR), current ESR (measured on the day), highest recorded C-reactive protein (CRP), current CRP (measured on the day).
Morbidities: considered present if patient had history of physician diagnosis of any of the following conditions known to be prevalent in SpA23: ischemic heart disease (IHD), cerebrovascular disease, hypertension (HTN), hyperlipidemia, diabetes mellitus, peptic ulcer disease, tuberculosis, osteoporosis, depression, cancer (melanoma, nonmelanoma skin cancer, lung, breast, gastrointestinal, genitourinary, lymphoma, hematological, other). Additionally, obesity and alcohol excess were noted. Obesity was recorded as a body mass index > 30 mg/kg2, as per the World Health Organization (WHO) criteria, based on the weight and height measurements taken by the investigator during the assessment. Alcohol excess was considered as alcohol consumption > 21 units/week in men and 14 units/week in women, as per national guidelines31, and based on the patient’s self-report of alcohol consumption. Patient medical records were used as required to confirm the presence or absence of each of these comorbidities. EAM were not considered as additional morbidities.
Physical examination: tragus-to-wall, cervical rotation, chest expansion, modified Schober test, lumbar side flexion, intermalleolar distance — all performed according to standardized technique32; current blood pressure, height (measured in cm), weight (measured in kg), waist circumference (measured in cm).
Dual-energy x-ray absorptiometry (DEXA): most recent DEXA result was obtained (if performed) and osteoporosis defined according to WHO33.
Outcome measures
The following validated patient-reported outcomes were collected:
Bath Ankylosing Spondylitis Disease Activity Index (BASDAI): measured on a scale of 0–10; higher scores indicate more severe disease34.
Bath AS Functional Index (BASFI): measured on a scale of 0–10; higher scores indicate worse function35.
Health Assessment Questionnaire (HAQ): assessed on a scale of 0–3; 0 indicates no disability and 3 indicates large burden of disability36.
AS Quality of Life (ASQoL): assessed on a scale of 0–18; higher scores indicate worse QOL37.
Bath AS Metrology Index (BASMI) assessed spinal mobility on a scale of 0–10; higher scores indicate worse spinal mobility32.
Multimorbidity
Morbidity is defined as the presence of a chronic condition in a patient. We defined multimorbidity as the presence of at least 2 chronic conditions in 1 person10,38. Severity of multimorbidity was assessed by counting the number of chronic conditions in addition to axSpA present in an individual20,39. Of note, EAM were not considered a separate morbidity.
Statistical analysis
Descriptive statistics are presented as mean with SD, median with 25th and 75th percentiles, or frequencies with percentage as appropriate. Independent 2-tailed t tests, Mann-Whitney U test, or ANOVA were performed on continuous data as indicated to examine differences between groups. Chi-square tests compared categorical variables. The Tukey honestly significant difference test controlled for multiple comparisons.
We developed separate models determining the association between (1) being multimorbid, and (2) worsening multimorbidity, defined by number of additional chronic conditions, and disease outcome measures. BASDAI, BASMI, BASFI, ASQoL, and HAQ were individually treated as dependent variables. Initially we investigated univariable demographic, treatment, and disease-related characteristics associated with each outcome. To control for the effects of these characteristics, we built a model using all variables with a p value < 0.1 in univariable analysis and performed hierarchical regression, entering variables in blocks of demographics, treatment, and disease-related variables prior to assessing the effect of multimorbidity. Age and sex were controlled for in every model. Adjusted R2 was used to determine the additional variation explained by each block of variables entered. The final models retained variables that significantly improved the fit.
The appropriate assumptions for each statistical test were met. A p value < 0.05 was considered statistically significant. Statistical analyses were performed using IBM SPSS Statistics version 24 (IBM Corp.).
RESULTS
Baseline characteristics
At the time of database extraction in February 2018, the ASRI cohort contained 734 patients, from 12 rheumatology centers representing all geographical regions of Ireland. Seventy-seven percent (n = 536) of the patients in ASRI are male, with a mean (SD) age of 45 (12) years, and a median (interquartile range) disease duration of 16 (9–27) years. The baseline demographic and clinical characteristics of the ASRI cohort are outlined in Table 1.
Baseline demographic and clinical characteristics of the cohort according to multimorbidity status.
Multimorbidity profile of ASRI cohort
Fifty-five percent of the cohort (n = 403) are multimorbid (i.e., at least 1 chronic condition in addition to axSpA): 25% (n = 180) have 1 additional chronic condition, 16% (n = 118) have 2 additional chronic conditions, 8% (n = 57) have 3 additional chronic conditions, and 7% (n = 48) have 4 or more additional chronic conditions.
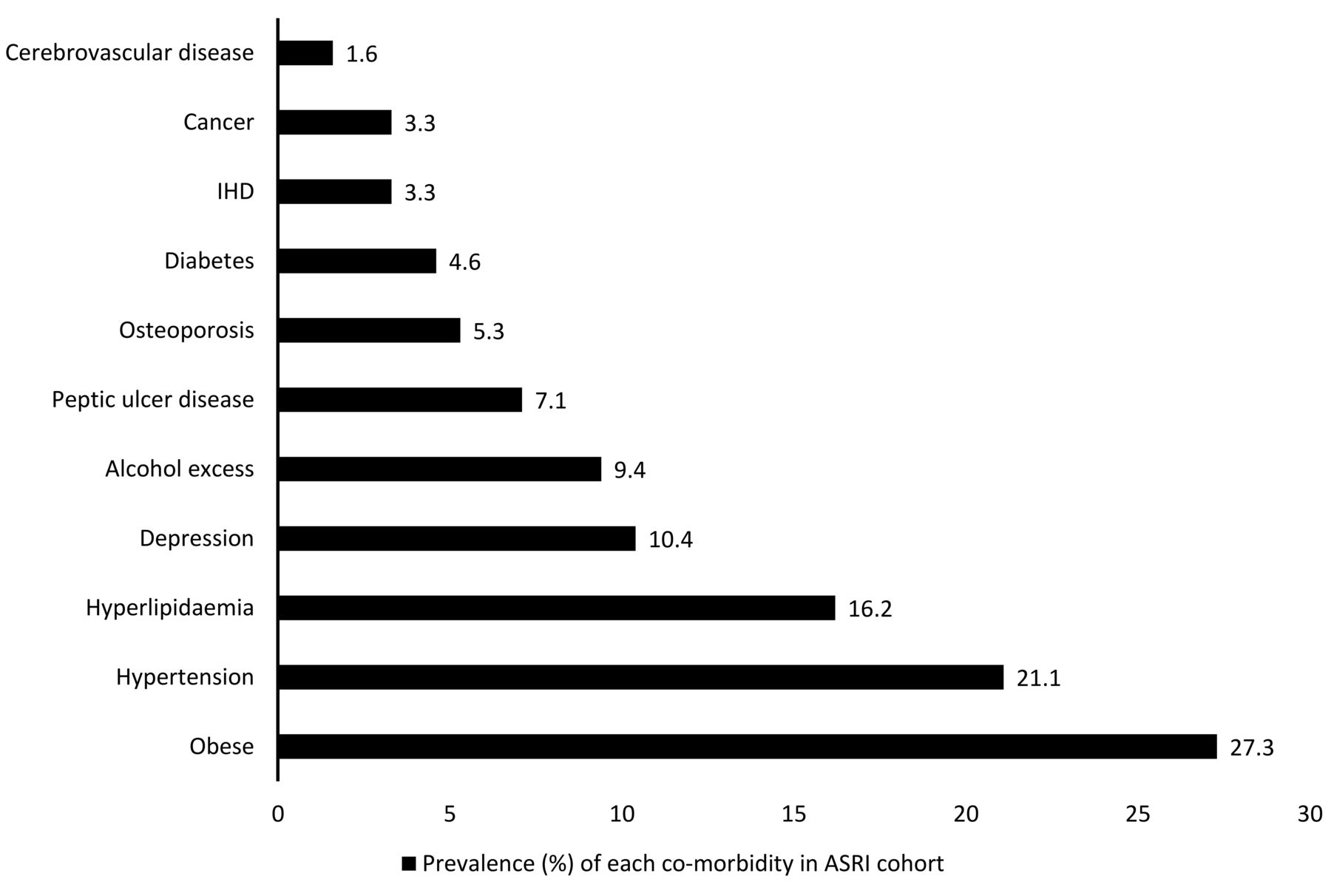
The most prevalent chronic condition is obesity, affecting 27% (n = 192) of the population, followed by HTN (n = 155, 21%), hyperlipidemia (n = 119, 16%), and depression (n = 76, 10%). Thirty percent (n = 222) of patients have cardiovascular comorbidity (i.e., at least 1 of IHD, cerebrovascular disease, HTN, or hypercholesterolemia). Remaining conditions are outlined in Figure 1.
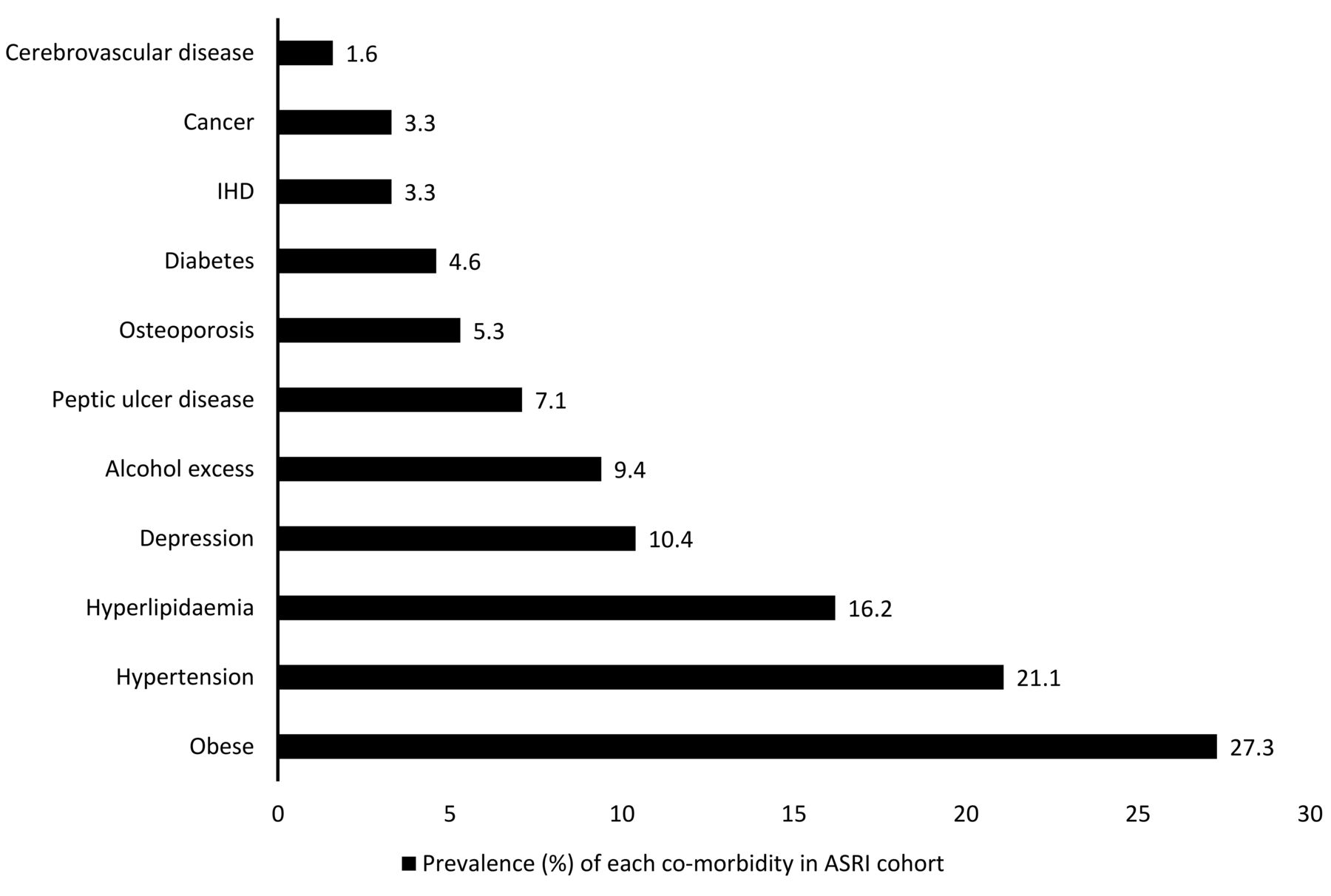
Prevalence of comorbidities in the Ankylosing Spondylitis Registry of Ireland (ASRI), ranked from least to most common. IHD: ischemic heart disease.
Thirty-nine patients (5.3%) report a prior diagnosis or had a diagnosis recorded in the medical record of osteoporosis. Only 19.5% (n = 143) had previously had a DEXA, of which 95 hip and 94 spine DEXA results were available (results of DEXA performed in private facilities or primary care were not universally available): 58% had low bone mineral density (BMD) at the hip (43% osteopenia, 15% osteoporosis), and 50% had low BMD at the spine (33% osteopenia, 17% osteoporosis).
Comparison of multimorbid and non-multimorbid patients: demographics/clinical characteristics
Multimorbid patients are older, with longer disease duration and longer delay to diagnosis than axSpA-only patients (Table 1). Multimorbid patients have similar CRP and ESR to the axSpA-only cohort. Sex and HLA-B27 status have no effect on the presence or absence of multimorbidity. The prevalence of psoriasis is higher in multimorbid patients than in axSpA-only patients (21% vs 15%, p = 0.02). Uveitis and IBD are equally prevalent in both groups.
Effect of multimorbidity on disease outcomes
Across all disease outcome measures, multimorbid patients have more severe disease than patients with axSpA only (Table 1). Disease outcome measures also correlate with the burden of multimorbidity, which is measured by the number of additional chronic conditions: as the burden of multimorbidity increases, BASDAI scores worsen (see Table 2 for all outcome measures).
Relationship between increasing multimorbidity and disease outcome measures.
The cohort was subsequently compared in 3 groups: (1) axSpA only; (2) multimorbid with 1 additional chronic condition; and (3) multimorbid with 2 or more additional chronic conditions. Disease outcome measures were all significantly higher in patients with multimorbidity compared to patients with axSpA only, regardless of the number of chronic conditions (Table 3). However, when comparing within the patients with multimorbidity, only BASMI, BASFI, and HAQ were significantly higher in patients with 2 or more additional conditions compared to patients with 1 additional condition. There was no difference in BASDAI and ASQoL scores between the multimorbid cohort with 2 or more additional conditions and 1 additional condition (Table 3; ANOVA analysis presented in Supplementary Table 1, available from the authors on request).
Comparison of disease outcome scores for patients with axSpA only, multimorbid patients with 1 additional condition, and multimorbid patients with 2 or more conditions.
Regression analysis: multimorbid versus non-multimorbid
In adjusted analyses (Table 4A), when compared to patients with axSpA only, being multimorbid is associated with a higher BASDAI of 0.7 (95% CI 0.34–1.05), BASMI of 0.45 (95% CI 0.09–0.80), BASFI of 0.5 (95% CI 0.23–0.78), HAQ of 0.07 (95% CI 0.00–0.13), and ASQoL of 0.87 (95% CI 0.28–1.46).
Adjusted analyses of association between disease outcome measures, and presence of multimorbidity.
Adjusted analyses of association between disease outcome measures and severity of multimorbidity.
Severity of multimorbidity
In separate models investigating the association between severity of multimorbidity and outcomes (Table 4B), the presence of each additional condition was associated with a higher BASDAI of 0.23 (95% CI 0.09–0.37), BASMI of 0.20 (95% CI 0.05–0.34), ASQoL of 0.25 (95% CI 0.02–0.49), HAQ of 0.03 (95% CI 0.01–0.06), and BASFI of 0.21 (95% CI 0.10–0.32).
DISCUSSION
There is growing interest in multimorbidity. Multimorbid patients have complex needs, requiring cohesive individualized patient-centered strategies rather than the traditional disease-focused model of care, to meet the needs of a rapidly expanding population8. The negative consequences of multimorbidity are well outlined in the general population12,13,15, but much less is known about its effect in patients with axSpA. Our study found multimorbidity is common in patients with axSpA, affecting over half (55%) of this large well-characterized cohort. Additionally, multimorbidity is associated with worse disease outcomes than in those with axSpA alone.
The prevalence in our cohort is higher than in the general population, where the prevalence of multimorbidity is around 23%12, although estimates vary from 13% to 95%11,39 depending on age group and definition of multimorbidity used. Prevalence of multimorbidity is also higher in primary care populations than the general population40. MSD is common in patients with multimorbidity16 and multimorbidity is equally prevalent in RA, affecting over 60% of patients20; therefore, it is unsurprising that multimorbidity is common in patients with axSpA.
In our study, we defined the differences between multimorbid and axSpA-only patients. Multimorbid patients with axSpA have longer disease duration, longer delay to diagnosis, and are on average 10 years older than patients with axSpA only, a similar trend to other populations where multimorbidity increases with age12,41. However, with multimorbid axSpA patients averaging 50 years, younger than those seen in primary care practice populations and in RA12,19, multimorbidity is not exclusive to the elderly in axSpA.
A systematic review of the general population found an association between women and multimorbidity11. However, the literature is conflicting in RA, where both no sex effect19 and a predominance of women in the multimorbid group42 have been shown. Males and females are equally affected by multimorbidity in our study.
Obesity is the most common morbidity, affecting 26% of our cohort. The prevalences of HTN (21%) and hypercholesterolemia (16%) are lower in our study than in ASAS-COMOSPA, but frequencies of IHD (3%) and cerebrovascular disease (2%) are similarly low23. Cardiovascular morbidity is common (30%) in multimorbid patients in our study, reflecting international trends7. Depression is prevalent in our study, affecting 10% of patients, as is alcohol excess (9%).
Obesity is not always included in multimorbidity scores; it is counted as a chronic condition in only 5 of 39 multimorbidity counts in a systematic review in 201143. However, obesity was not officially recognized as a disease until 201344. Because it clearly increases mortality45 and represents a growing public health challenge, it is worthy of being considered in a multimorbidity count41, so we decided to include it.
In ASAS-COMOSPA, osteoporosis was the most frequent comorbidity, affecting 13% of the cohort23. The prevalence of self-reported osteoporosis in our study is 5.3%. However, systematic screening is not feasible in the context of a registry study. Using the DEXA data available in a minority of the cohort, 17% have osteoporosis. However, this may be an overestimation of the population prevalence, because patients referred for DEXA assessment likely had risk factors making a diagnosis of osteoporosis more probable, thus the true prevalence is expected to fall between 5 and 17%, closer to that reported in ASAS-COMOSPA.
The second aim of this study is to determine the association between multimorbidity and disease outcomes in axSpA. We demonstrate an association between multimorbid patients and worse disease outcomes, using both subjective and objective outcome measures. As the severity of multimorbidity increases, so too do disease outcome scores. Our results reflect the general population, where multimorbidity is associated with impaired function and worse QOL, particularly if a rheumatic disease is involved46, and RA, where multimorbid patients have more severe disease and more fatigue than patients with RA only19,47. Nikiphorou, et al24 similarly demonstrated that a rising comorbidity burden is associated with worse QOL in patients with SpA.
However, what differentiates our study from those that focus on comorbidity is we demonstrate that simply being multimorbid (i.e., having any additional condition to axSpA) is associated with worse outcomes compared to patients with axSpA alone. The difference in outcomes between axSpA-only and being multimorbid is more marked than the difference for each additional condition thereafter. This has potential to be a clinically useful finding, which could provide physicians with a simple method to identify patients at risk of poor outcomes.
We acknowledge some limitations. First, the cross-sectional design of this registry study prohibits comment on causality; therefore, we can merely observe the association between multimorbidity and severe disease. Second, the absence of information on comorbidities not collected within the framework of ASRI represents a potential limitation. However, our study reports the comorbidities known to occur most commonly in SpA, as outlined in ASAS-COMOSPA23, with the exception of infections (hepatitis B prevalence of 3.5% in SpA worldwide). In Ireland the prevalence of hepatitis B is known to be very low (< 0.1%)48; therefore, it is unlikely to have influenced the results. Additionally, pulmonary disease is not collected in ASRI. However, although abnormalities on high-resolution computed tomography imaging of the thorax are common49, the clinical significance of these is unknown50; therefore, we are confident that not including a measure of the prevalence of pulmonary disease is unlikely to have significantly affected the prevalence of multimorbidity. Third, alcohol intake is based on the patient’s own report. It has been well established that patients tend to underestimate their alcohol consumption. All efforts were made to establish an accurate alcohol intake, but it is possible that intake was underreported, thus underestimating the prevalence of alcohol excess. Fourth, our population is overwhelmingly white; therefore, extrapolating the results of our study to other ethnicities is not possible.
Our study has many strengths. It is a large study, with a well-characterized cohort. The homogeneous characteristics of our patients reduces variation that could be introduced from diverse backgrounds. Additionally, it contains real-life data, providing clinicians with relevant and clinically useful information. It is also novel, as the first study to examine prevalence estimates of multimorbidity in axSpA, to our knowledge. To date, studies have primarily focused on individual comorbidities in axSpA, along with their effect on disease outcomes/management. Focusing on individual conditions takes the focus away from the patient; different conditions are considered the index disease by different clinicians, all aiming for best control of their disease of interest, without necessarily considering its effect on other diseases, potentially leading to fragmented care8,9. Multimorbidity brings the focus back to the patient, not the disease. Further research is needed to further delineate the effect of multimorbidity in our patients. Specifically, prospective longitudinal studies are needed to investigate the development of multimorbidity in axSpA and its effect on disease outcomes over time.
We have demonstrated that multimorbidity is prevalent in patients with axSpA and that the presence of multimorbidity is associated with worse disease outcomes.
Acknowledgment
This study was conducted on behalf of the steering committee of the ASRI. We thank all the patients for participating in this study. We also thank all the personnel in the centers who so willingly and enthusiastically contributed, and continue to contribute, data to ASRI: Blackrock Clinic, Cork University Hospital, Galway University Hospitals, Midland Regional Hospital Tullamore, Our Lady’s Hospital Manorhamilton, Our Lady’s Hospital Navan, St. James’s Hospital, St. Vincent’s University Hospital, Tallaght University Hospital, University Hospital Kerry, University Hospital Limerick, and University Hospital Waterford.
Footnotes
The Ankylosing Spondylitis Registry of Ireland (ASRI) is supported by an unrestricted grant from Pfizer Pharmaceuticals and AbbVie Pharmaceuticals. GF is a recipient of the Bresnihan-Molloy Scholarship from the Royal College of Physicians of Ireland, funded by AbbVie. The funders had no role in the design of the study, collection of the data, analysis, and interpretation of the data, or any part of manuscript preparation.
- Accepted for publication May 6, 2019.








{kind=link}