

Abstract
Objective. To study the clinical phenotypes of centromeric proteins (CENP)-A- and CENP-B-positive patients with systemic sclerosis (SSc) and to compare them to anticentromere antibody (ACA)-positive and negative SSc patients.
Methods. Sera samples were collected from 802 patients with SSc enrolled in a multicenter cohort study. Antibodies to CENP-A and B were detected by ELISA, and ACA by indirect immunofluorescence. Associations with clinical and other serological manifestations of SSc were investigated.
Results. CENP-A antibodies were detected in 276 (34%), CENP-B in 286 (36%), and ACA in 279 (35%) patients. Patients having ACA, CENP-A, and/or CENP-B resembled each other and differed from the remainder of the cohort in the following respects: older chronologically and at disease onset; more commonly women; more likely to have limited disease and lower skin scores; less likely to have finger ulcers, digital tuft resorption, or finger contractures; more likely to have pulmonary hypertension; less likely to have interstitial lung disease, scleroderma renal crisis, inflammatory arthritis, and inflammatory myositis; and having lower overall disease severity. CENP-A and/or B status was predictive of the extent of skin involvement over time. Patients with limited disease who were CENP-A-negative at baseline were more likely to progress to diffuse disease compared to CENP-A-positive patients (OR 2.55, 95% CI 1.37, 4.85, p = 0.004).
Conclusion. Clinical immunology laboratories are increasingly using high-throughput ELISA tests for CENP antibodies, with or without ACA detected by indirect immunofluorescence. The phenotype of CENP-A and/or B-positive patients is generally similar to that associated with ACA.
Autoantibodies are seen in more than 95% of patients with systemic sclerosis (SSc)1 and include several highly specific SSc-related autoantibodies, in particular anticentromere (ACA), topoisomerase I, and RNA polymerase III antibodies1,2. Interestingly, expression of these autoantibodies tends to be mutually exclusive2,3 and associated with specific demographic, clinical, genetic, and prognostic features2,4. Thus, SSc autoantibodies are highly valuable for the diagnosis and prognosis of the disease. In addition, growing knowledge of SSc autoantibodies is increasing understanding of the pathogenesis of the disease5,6,7.
ACA, one of the hallmark autoantibodies of SSc, has a sensitivity in the range of 20%–40% and specificity > 90%1,2. ACA are typically associated with limited cutaneous disease and/or CREST manifestations (calcinosis, Raynaud’s phenomenon, esophageal dysmotility, sclerodactyly, and telangiectasias)4. ACA have been reported to antedate the full clinical expression of disease8 and patients with ACA have also been reported to be at higher risk for pulmonary hypertension and lower risk of interstitial lung disease (ILD) and scleroderma renal crisis4,9,10,11.
In the clinical setting, ACA have traditionally been identified by indirect immunofluorescence (IIF), which identifies autoantibodies that bind to centromeric proteins (CENP), major constituents of the primary constriction of metaphase chromosomes. CENP autoantigens identified to date include CENP-A (17 kDa), CENP-B (80 kDa), CENP-C (140 kDa), CENP-D (50 kDa), CENP-E (312 kDa), CENP-F (400 kDa), CENP-G (95 kDa), and CENP-O (38 kDa)12. While this list continues to expand, most clinical attention has focused on CENP-A and CENP-B, which for the most part are the antigens detected by IIF in SSc and other sera13.
With the availability of commercially prepared and highly purified CENP, other immunoassays such as the ELISA, line immunoassay, and addressable laser bead immunoassays have been developed and are increasingly used in diagnostic laboratories. While a few studies have examined the prevalence of CENP-A and -B in SSc14,15, little has been published on the clinical correlates of the individual CENP-A or CENP-B autoantibodies. Because of the wider use of these CENP ELISA and limited clinical studies, we set out to study and identify the clinical phenotypes of CENP-A and B-positive patients with SSc and to compare them to ACA-positive and negative SSc patients. For clarity in this report, ACA will be used to refer to anticentromere antibodies detected by IIF on HEp-2 substrate.
MATERIALS AND METHODS
Study subjects
The Canadian Scleroderma Research Group (CSRG) is a consortium of clinical and basic science researchers who follow a cohort of patients with SSc recruited from 15 centers across Canada. Patients in the registry must have a diagnosis of SSc confirmed by a rheumatologist, be > 18 years of age, and be fluent in either English or French. Patients have been recruited since 2004 and are seen at baseline and thereafter yearly. For this study, subjects with complete serological data for ACA as detected by IIF, CENP-A and CENP-B detected by ELISA, and anti-topoisomerase I and RNA polymerase III were included.
Patients recruited into the CSRG registry undergo an extensive standardized evaluation. Serum samples are collected at baseline and yearly according to a standardized operating protocol and shipped to the University of Calgary (Calgary, AB, Canada) where they are aliquoted and stored at −70°C until used. Ethics committee approval for the CSRG data collection and study protocols was obtained at McGill University (Montreal, QC, Canada) and at all participating study sites. All subjects provided informed written consent to participate.
Autoantibody assays
IIF was performed on HEp-2 substrate (HEp-2000; ImmunoConcepts, Sacramento, CA, USA) that included fluorescein-conjugated goat antibodies to human IgG (H+L) in Calgary (Mitogen Advanced Diagnostics). IIF patterns were detected at serum dilutions of 1:160 and 1:640 on a Zeiss Axioskop 2 plus (Carl Zeiss, Jena, Germany) fitted with a 100-watt Ushio super-high-pressure mercury lamp (Ushio, Steinhöring, Germany) by 2 experienced technologists, who had no knowledge of the CENP-A or CENP-B ELISA results.
CENP-B ELISA (Dr. Fooke Laboratorien GmbH, Neuss, Germany) with recombinant full-length CENP-B expressed in insect cells was performed according to the manufacturer’s instructions. The CENP-A ELISA (Dr. Fooke Laboratorien GmbH), a CE-certified peptide-based assay, was performed according to the manufacturer’s instructions as described14. The optical density of each well was read and recorded on a Biomek1000 (Beckman Instruments, Palo Alto, CA, USA).
Samples were also tested for topoisomerase I by Quanta Plex™ SLE8 (Inova Diagnostics Inc., San Diego, CA, USA) and RNA Pol III by Quanta Lite® RNA Pol III (Inova Diagnostics Inc.) as described16.
Clinical assessments
Extensive medical evaluation was done, with standardized collection of clinical, laboratory, and radiologic data. Demographic variables were self-reported by the patients. Disease duration was recorded by the study physician and determined from the onset of the first non-Raynaud’s disease manifestation. Skin involvement was assessed using the modified Rodnan skin score17, a widely used clinical assessment where the examining rheumatologist records the degree of skin thickening ranging from 0 (no involvement) to 3 (severe thickening) in 17 areas (total score range 0–51), and patients were classified into limited and diffuse cutaneous subsets, based on the definition of LeRoy, et al18. Study physicians recorded the presence of Raynaud’s phenomenon, calcinosis, esophageal dysmotility, sclerodactyly, clinically visible mat-like telangiectasias on the face, limbs, chest or abdomen, active or healed fingertip ulcers, digital tuft resorption, and current medications. A history of scleroderma renal crisis, inflammatory polyarthritis, inflammatory myositis, malabsorption, and/or pseudoobstruction according to the study physician was also recorded. The presence of finger contractures was assessed with the fingertip-to-palm (FTP) distance recorded from the tip of the third finger to the distal palmar crease using the more severely affected hand. FTP distance has been recommended as a measure of finger contracture severity in SSc19 and has been used in previous studies20,21,22.
To further assess gastrointestinal involvement, patients answered yes/no to a series of 14 questions concerning appetite loss, difficulty swallowing, regurgitation of acid, nocturnal choking, heartburn, early satiety, abdominal bloating, nausea and vomiting, constipation, diarrhea, need for antibiotics for diarrhea, greasy stools, fecal incontinence, and need for parenteral nutrition. Patients also reported the severity of their gastrointestinal symptoms on a numerical rating scale ranging from 0, representing no disease, to 10, representing very severe disease.
Cardiopulmonary involvement was determined by symptoms, physical examination, chest radiograph, high-resolution computed tomographic (HRCT) scans of the chest, pulmonary function tests, and cardiac echocardiography. New York Heart Association functional class I–IV and the presence of typical “Velcro-like crackles” indicative of ILD on lung auscultation was determined by the study physician. Chest radiographs were reviewed by radiologists and the presence of increased interstitial markings (not thought to be due to congestive heart failure) or fibrosis was recorded. HRCT scans of the chest were also reviewed by radiologists and the presence of ground-glass, interstitial disease, or honeycombing was recorded. Pulmonary function testing was performed in laboratories working in accordance with American Thoracic Society standards. Data were extracted concerning forced vital capacity, total lung capacity, and carbon monoxide diffusing lung capacity using the single-breath method, and are expressed as a percentage of predicted. Pulmonary artery pressure (PAP) was measured by cardiologists using the Doppler flow measurement of the tricuspid regurgitant jet on echocardiography.
For the purposes of this study, ILD was considered present if a HRCT scan of the lungs showed ground-glass, interstitial disease, or honeycombing. In the case where no HRCT was available, ILD was considered present if either a chest radiograph was reported as showing either increased interstitial markings (not thought to be due to congestive heart failure) or fibrosis, and/or if a study physician reported findings indicative of ILD on physical examination. Pulmonary hypertension was defined as an estimated systolic PAP > 45 mm Hg (an estimate that correlates strongly with right heart catheter studies23).
Finally, physicians and patients completed global assessments of disease severity, using an 11-point numerical rating scale ranging from 0, representing no disease, to 10, representing very severe disease.
Statistical evaluation
Descriptive statistics were used to summarize the baseline characteristics of the cohort and to compare ACA, CENP-A, and CENP-B-positive and negative patients. Receiver-operation characteristic (ROC) curves were used to determine the optimal cutoffs for the CENP-A and CENP-B assays to identify patients classified as having limited or diffuse cutaneous disease. Two-by-two tables were constructed to determine whether CENP-A and CENP-B-positive/negative status could predict limited/diffuse disease subsets. Positive and negative predictive values of CENP-A and CENP-B antibodies were examined at various antibody cutoffs. All statistical analyses were performed using SAS 9.2 (SAS Institute, Chicago, IL, USA) and R: A Language and Environment for Statistical Computing, v.2.10.0 (R Foundation, Vienna, Austria; http://www.R-project.org).
RESULTS
Our study included 802 patients with SSc with complete serological profiles. The mean age (± SD) was 56 (± 12) years, 86% were women, 85% were white, mean disease duration was 11 (± 9) years, and 38% had diffuse disease (Table 1). ACA detected by IIF on HEp-2 substrate were identified in 279 patients (35%). In addition, topoisomerase I antibodies were identified in 128 (16%) and RNA polymerase III antibodies in 144 patients (19%).
Baseline characteristics of the study cohort as a whole and for those positive for ACA*, CENP-A, and CENP-B.
Cutoffs for CENP-A and CENP-B
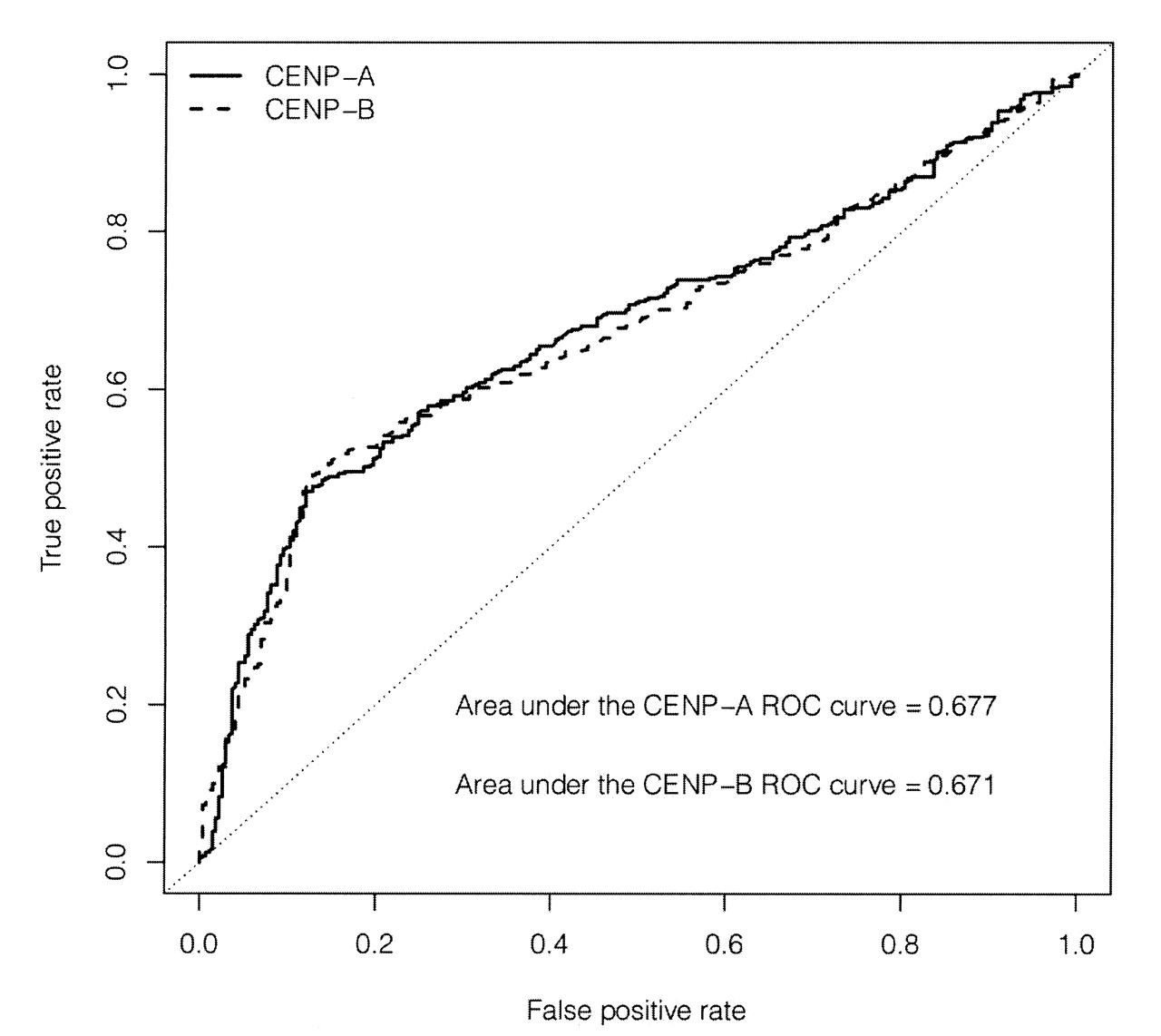
When the ELISA cutoff values of 1.5 calculated units (CU) recommended by the manufacturers were used initially, the clinical associations (e.g., disease phenotypes) of CENP-A and CENP-B antibodies were less distinct than those of ACA as detected by IIF. Therefore, we first undertook to determine the optimal cutoffs for “positive” values for CENP-A and CENP-B. To do this, we made the assumption that, as for ACA by IIF, both CENP-A and CENP-B would be associated with limited cutaneous disease. Using ROC curves and maximizing the weighted averages of the sensitivities and specificities for the respective antibody, we found that the optimal cutoff for CENP-A was 3.58 CU and for CENP-B 2.17 CU (Figure 1). Using these cutoffs, ELISA-based assays detected CENP-A antibodies in 276 (34%) sera and CENP-B antibodies in 286 (36%) sera. For CENP-A, the optimized cutoff yielded a sensitivity of 47% and a specificity of 88%, compared to a sensitivity of 49% and a specificity of 87% for CENP-B, for the detection of limited versus diffuse cutaneous disease. The area under the curve (AUC) was 0.677 for CENP-A and 0.671 for CENP-B. Note that an AUC of 0.7 is generally regarded as “reasonable” and our results are slightly below that, likely because of relatively higher specificity (low number of diffuse patients who are classified as positive) but lower sensitivity (high number of limited patients who were not positive).

Receiver-operation characteristic (ROC) curves for CENP-A and CENP-B to identify SSc patients with either limited or diffuse skin involvement.
Similarities among CENP-A, CENP-B, and ACA-positive patients
As expected, using the cutoffs for CENP-A and CENP-B described above, there was considerable overlap among ACA, CENP-A, and CENP-B-positive patients (Figure 2). Of the 301 patients positive for any 1 of those 3 antibodies, 260 (86%) were positive for all 3. ACA identified 279 patients (92%), CENP-A identified 276 patients (92%), and CENP-B identified 286 patients (95%). The overlap among topoisomerase I and ACA, CENP-A, and CENP-B was low, in the order of 1% (Figure 3A). This was also the case for the overlap of RNA polymerase III and ACA, CENP-A, and CENP-B (Figure 3B).
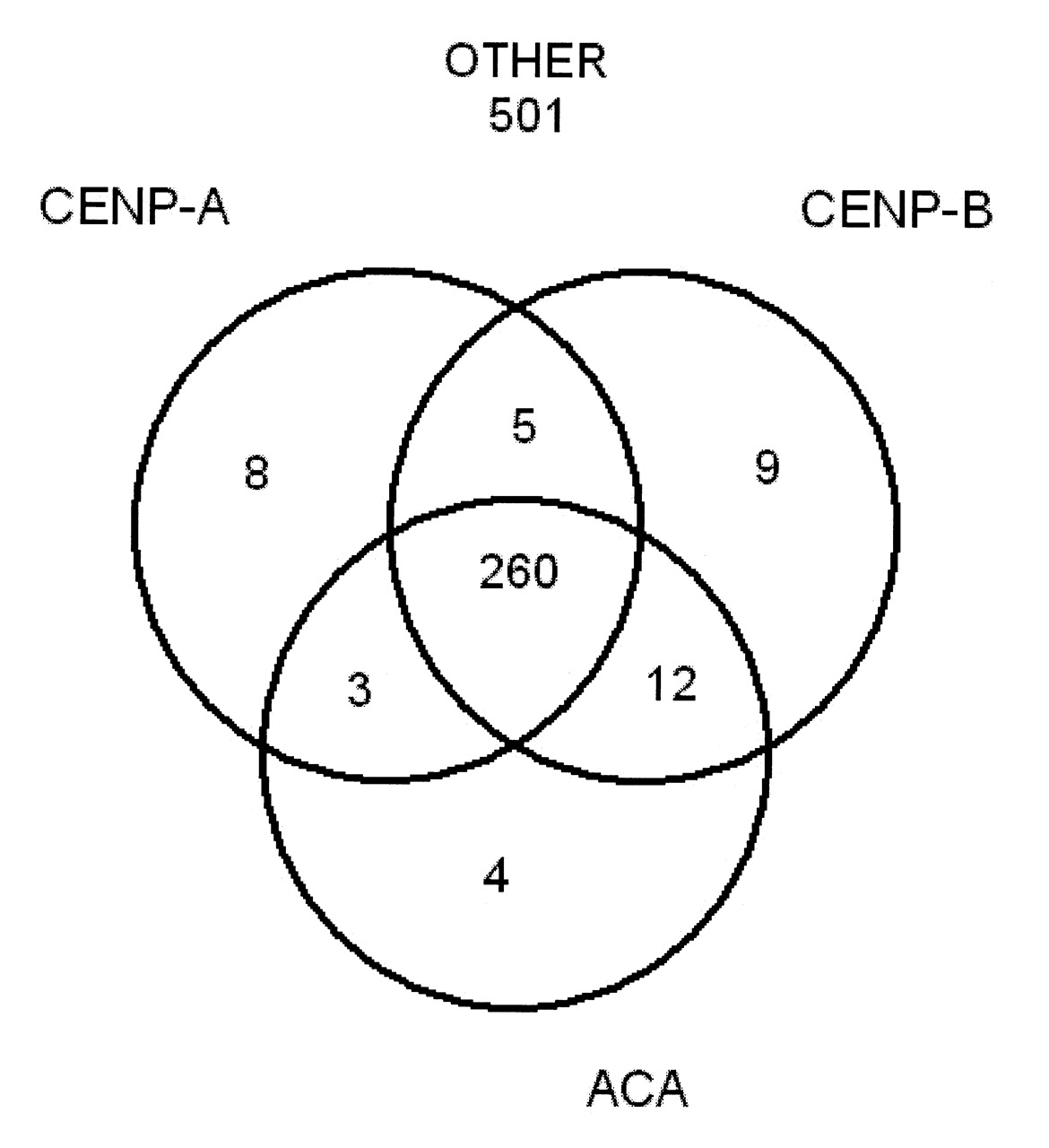
The overlap of anticentromere antibodies (ACA), CENP-A, and CENP-B-positive patients.

The overlap of anticentromere antibodies (ACA), CENP-A, CENP-B, and (A) topoisomerase I (topo I) and (B) RNA polymerase III (RNA pol III)-positive patients.
When we compared their characteristics, the overall characteristics of ACA, CENP-A, and CENP-B-positive patients were very similar to each other but different from the remainder of the CSRG cohort (Table 1). Among other things, ACA, CENP-A, and/or CENP-B patients resembled each other and differed from the remainder of the cohort in the following respects: older chronologically and at disease onset; more commonly women; more likely to have limited disease and lower skin scores; less likely to have finger ulcers, digital tuft resorption, or finger contractures; more likely to have pulmonary hypertension; less likely to have ILD, scleroderma renal crisis, inflammatory arthritis, and inflammatory myositis; and lower overall disease severity. Note that it is not meaningful to compare the various groups using p values because the groups are not mutually exclusive (i.e., there are many patients who are positive for ACA, CENP-A, and CENP-B). Thus, these results should be interpreted by looking at whether the groups are similar or different in clinically meaningful ways.
Positive and negative predictive values of CENP-A and B
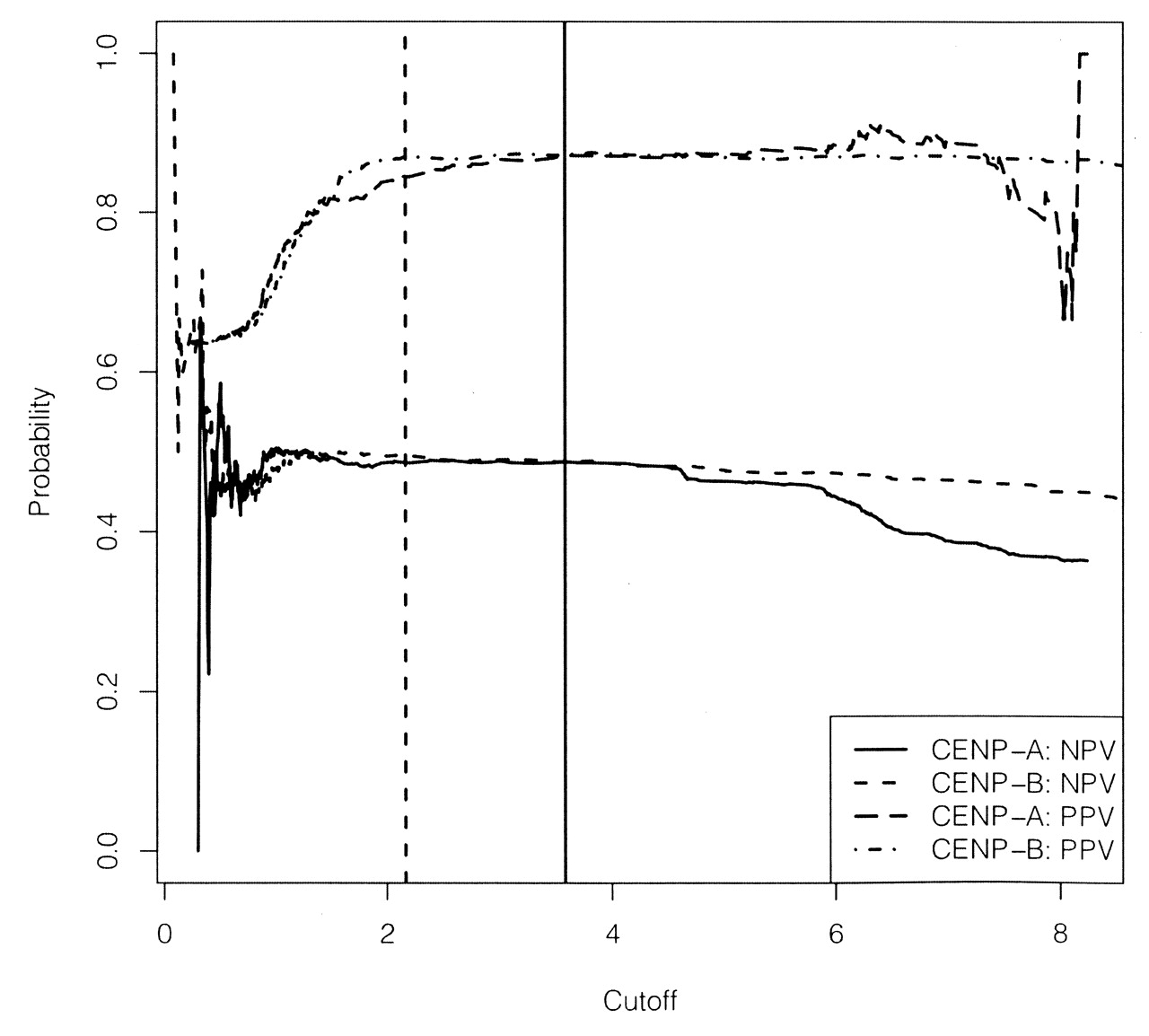
An alternative way to think about the characteristics of CENP-A and B is to consider their positive (PPV) and negative (NPV) predictive values, which was the proportion of CENP-A (or CENP-B) positive patients who are limited and the proportion of CENP-A (or CENP-B) negative patients who are diffuse. We examined the PPV and NPV of CENP-A and CENP-B over the range of possible cutoffs for those assays (Figure 4); interestingly, the PPV was much higher than the NPV. In other words, the proportion of CENP-positive patients who are limited was quite high (over 85%). However, the NPV was much lower. Thus, again, CENP positivity was predictive of the limited cutaneous phenotype, whereas negativity was associated with much greater uncertainty about whether the patients had either limited or diffuse disease. It is worthwhile to note that PPV and NPV were also maximized at cutoffs similar to those identified by the ROC curves described above.

Positive (PPV) and negative (NPV) predictive values of CENP-A and CENP-B to identify patients with limited or diffuse skin involvement at various assay cutoff values. Vertical lines represent the “optimal” cutoffs for CENP-A (solid line) and CENP-B (broken line).
Predictive ability of CENP-A and B
To illustrate that the CENP-A and CENP-B phenotypes are similar to ACA, we considered that ACA positivity is usually predictive of limited skin involvement. We wished to determine whether CENP positivity was also predictive of the extent of skin involvement over time. We therefore looked at patients who were identified as having limited skin disease at baseline and then examined their limited/diffuse status over time. We included only patients who had 4 or more yearly visits (i.e., 3 after baseline). There were 209 limited patients at baseline with at least 3 visits after baseline. Limited patients who were CENP-A-negative at baseline were more than twice as likely to progress to diffuse disease compared to patients who were CENP-A-positive (OR 2.55, 95% CI 1.37, 4.85; p = 0.004; Table 2). The results were similar for CENP-B (data not shown). Thus, CENP-A and/or B status was predictive of the extent of skin involvement over time.
Association between CENP-A positive and negative status and limited and diffuse skin involvement during followup in patients with limited skin disease at baseline and at least 3 years of followup (n = 209).
DISCUSSION
In this large cohort of Canadian patients with SSc with well-defined clinical phenotypes, ACA, CENP-A, and CENP-B antibodies identified virtually all of the same patients. Not surprisingly, then, the clinical correlates of ACA-positive antibodies were highly similar to those of CENP-A and CENP-B-positive antibodies. This information is of considerable clinical importance because clinical immunology laboratories are increasingly using high-throughput ELISA tests for CENP antibodies, with or without ACA detected by IIF. Accordingly, it is imperative that clinicians should be informed that the phenotype that they generally associate with ACA in SSc is similar to that which they should associate with CENP-A and/or B-positive antibodies.
Two previous studies examined the clinical associations of CENP-A and B antibodies in SSc. Mahler, et al14 evaluated the sensitivity and specificity of the CENP-A in 90 SSc sera samples using the same ELISA kit used in our study and showed that it was a sensitive and specific marker for SSc. Indeed, because ACA are occasionally found in other autoimmune diseases such as systemic lupus erythematosus, it was suggested that the CENP-A assay was more specific for SSc. Moreover, consistent with our findings, their preliminary analysis of clinical correlates of the 90 patients with SSc showed that, overall, CENP-A-positive patients had lower modified Rodnan skin scores than CENP-A-negative patients. Hanke, et al15 recently published a study examining the clinical correlates of CENP-A and CENP-B antibodies, albeit measured with a different assay (Euroimmun), in 280 patients. They showed good sensitivity (37%) and high concordance (94%) of their CENP-A/CENP-B assays in patients with SSc. Also, consistent with our findings, antibodies to both CENP-A and B were associated with similar clinical manifestations and identified patients with limited disease phenotypes.
Interestingly, consistent with the findings reported by Hanke, et al15, we found that ACA, CENP-A, and CENP-B overlapped considerably with each other. However, in SSc in general, and in our cohort in particular, autoantibodies to CENP, topoisomerase I, and RNA polymerase tended to be mutually exclusive2,3. This supports the notion that endogenous macromolecular complexes (e.g., centromeric chromatin) rather than molecular mimicry of exogenous antigens are what drive the B cell response in SSc24,25. However, CENP-A and CENP-B antibodies, although distinct proteins14, share a cross-reactive epitope motif that has been shown to mediate epitope spreading. It is possible that, for this reason, most SSc patients with 1 antibody may have antibodies to both centromere antigens26,27. Of note, unlike topoisomerase I and certain other nuclear antigens, CENP are not cleaved during Fas-mediated apoptosis28, suggesting that the antigens involved may induce B cell reactivity by other pathways.
In a longitudinal study of a patient with SSc26, it was shown that anti-CENP-A reactivity could be induced by intra- and intermolecular epitope spreading from histone H3 and that antibodies to CENP-A peptides could temporally precede autoreactivity to recombinant CENP-B. The CENP-A peptide ELISA used in this study was based on the same peptide epitope as the ELISA used in our study. In that context it is of high interest that patients who reacted with CENP-A but not CENP-B had significantly shorter disease duration than patients positive for CENP-B alone.
In this study, the prevalences of ACA, CENP-A, and CENP-B were almost identical (35%, 34%, and 36%, respectively). The prevalence of CENP-A and/or CENP-B increased to 37%. This suggests that an ELISA for CENP-A and/or CENP-B could possibly replace IIF for ACA. This is especially important given the greater resources and expertise required for IIF, compared to ELISA testing.
In the absence of a “gold standard,” choosing normal cutoffs for a test can be challenging. One approach is to set an arbitrary cutoff based on the distributional properties of the test (e.g., simply taking 2 SD from the general population mean). Another, more objective approach, is to use ROC curves to optimally classify patients according to an independent clinical characteristic. In our study, after optimizing the cutoffs for CENP-A and B based on their ability to differentiate between limited and diffuse cutaneous disease, we found that the clinical profiles of ACA, CENP-A, and CENP-B-positive patients were all very similar. There is circularity in this reasoning and to an extent the results are as expected. Nevertheless, by increasing the predictive ability of the test, ROC curve analysis enables identification of a “best cutoff” for clinical purposes.
SSc is characterized by a wide spectrum of clinical phenotypes and most attempts to create subsets of this disease to date, including the limited and diffuse subsets used in our study, rely on the extent of cutaneous involvement29. On the other hand, our data clearly show that about 20% of patients with the limited phenotype are negative for ACA, CENP-A, and/or CENP-B, and that 15% of patients with diffuse disease are positive for 1 or more of those antibodies. Thus, understanding of the relationship between limited cutaneous disease and ACA is far from perfect. With this is mind, some investigators have advocated basing the subsets of the disease on antibody profiles, rather than clinical phenotypes10,30. Among other things, this may influence how we manage and follow patients clinically, improve our prognostic abilities, and direct genetic and basic science research, as well as serving as useful criteria for inclusion in clinical trials.
Our study contributes significantly to knowledge concerning the clinical significance of CENP-A and B in SSc. This is the largest and most detailed published analysis of the clinical correlates of CENP-A and B in SSc. The clinical phenotypes of CENP-A and/or B patients are generally consistent with that associated with ACA-positive patients. The data from this and previous studies14,15 indicate that CENP-A and CENP-B assays can be used (1) to identify patients with SSc with high sensitivity and specificity; and (2) to identify the same clinical phenotypes as are known for ACA, using optimized cutoff values. Finally, many laboratories are moving to ELISA and other assays to screen and test for specific autoantibodies. Thus, it is important to appreciate that the clinical correlations of high-throughput assays, such as ELISA, are consistent with the time-honored ACA IIF assay.
APPENDIX
List of study collaborators. Investigators of the Canadian Scleroderma Research Group: J. Markland, Saskatoon, Saskatchewan; D. Robinson, Winnipeg, Manitoba; N. Jones, Edmonton, Alberta; N. Khalidi, Hamilton, Ontario; P. Docherty, Moncton, New Brunswick; E. Kaminska, Hamilton, Ontario; A. Masetto, Sherbrooke, Quebec; E. Sutton, Halifax, Nova Scotia; J-P. Mathieu, Montreal, Quebec; S. Ligier, Montreal, Quebec; T. Grodzicky, Montreal, Quebec; C. Thorne, Newmarket, Ontario; S. LeClercq, Calgary, Alberta.
Footnotes
-
Supported in part by the Canadian Institutes of Health Research, the Scleroderma Society of Canada and educational grants from Actelion Pharmaceuticals and Pfizer Inc. Autoantibody diagnostic kits were a gift of Inova Diagnostics Inc. (San Diego, CA, USA), ImmunoConcepts (Sacramento, CA, USA), and Dr. Fooke Laboratorien GmbH (Neuss, Germany). Dr. Hudson is a New Investigator supported by the Canadian Institutes of Health Research and the Fonds de la recherche en Santé du Québec, and Dr. Fritzler holds the Arthritis Society Research Chair at the University of Calgary.
- Accepted for publication November 10, 2011.








{kind=link}
{kind=link}
{kind=link}
{kind=link}