

Abstract
Objective. To determine the rate of temporomandibular joint (TMJ) involvement and find factors associated with TMJ arthritis in a single-center cohort of patients with juvenile idiopathic arthritis (JIA).
Methods. Retrospective analysis of all patients with JIA visiting the rheumatology clinic between January 1, 2005, and December 31, 2006. Followup information was included until August 2008. A diagnosis of TMJ arthritis was based on clinical rheumatological and/or radiological findings.
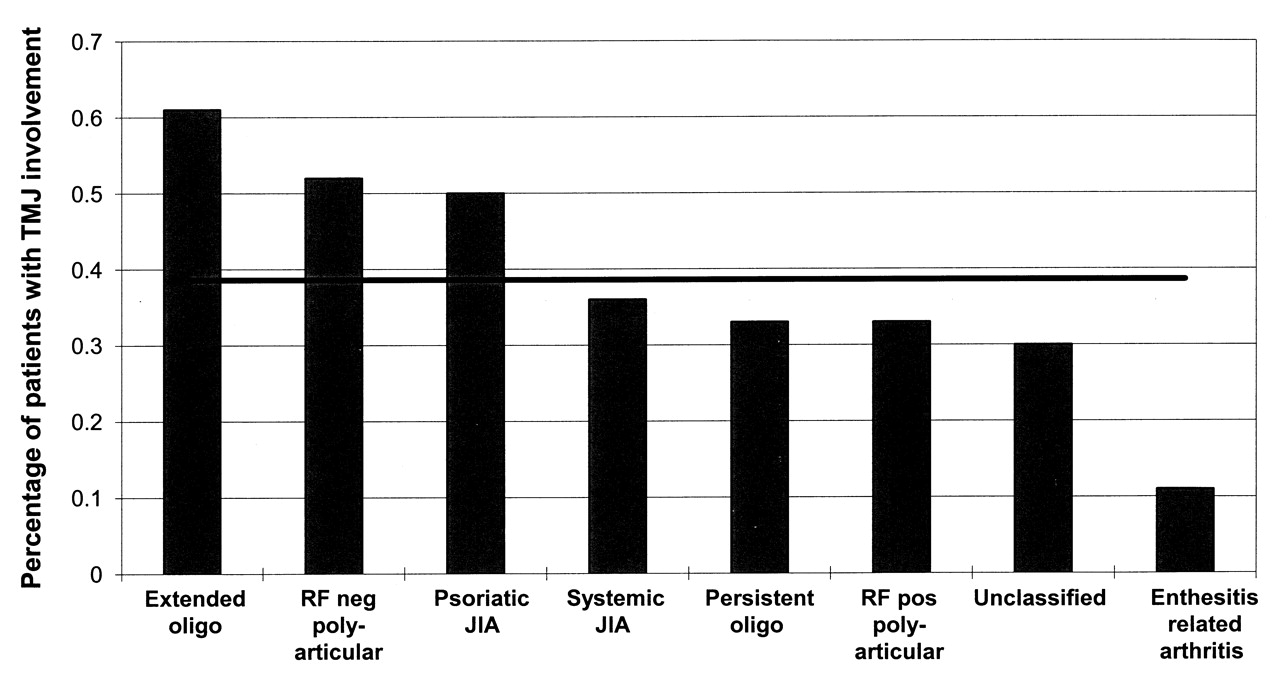
Results. After a mean followup time for JIA of 4.6 years (range 0.08–14.17), 86/223 patients (38.6%) had developed TMJ arthritis. The rate of TMJ involvement differed significantly among JIA subtypes (p = 0.0016), with 61% in extended oligoarticular, 52% in polyarticular rheumatoid factor (RF)-negative, 50% in psoriatic, 36% in systemic, 33% in polyarticular RF-positive, 33% in persistent oligoarticular, 30% in unclassified JIA, and 11% in enthesitis-related arthritis. The rate of TMJ involvement in our cohort was statistically significantly lower for patients who were HLA-B27-positive (p = 0.0002). In a multivariate analysis, the association of the following factors was confirmed: JIA subtype (p = 0.0001), a higher erythrocyte sedimentation rate (ESR) at diagnosis (p = 0.0038), involvement of joints of the upper extremity (p = 0.011), the absence of HLA-B27 (p = 0.023), and younger age at onset of JIA (p = 0.050).
Conclusion. In our cohort of children with JIA, the overall rate of TMJ involvement was 38.6%. Patients with certain JIA subtypes, a higher ESR at disease onset, involvement of upper extremity joints, and younger age at diagnosis were more likely to develop TMJ arthritis. The presence of HLA-B27 seemed to be protective.
Juvenile idiopathic arthritis (JIA) is the most common rheumatic disease in childhood1. It affects synovial joints and can involve the temporomandibular joint (TMJ)2,3,4,5. TMJ involvement in patients with JIA is a well recognized feature of the disease. Depending on the examination methods used and the population studied, the rate of TMJ involvement in patients with JIA varies from 17% to 87%3,5,6,7. Most studies found a higher rate of TMJ involvement2,4,8,9 in JIA subgroups with polyarticular joint involvement, although in one study TMJ involvement occurred irrespective of JIA subtype5. More recently there is evidence that the TMJ may also be the initial or even the only joint affected10,11. Because of the special ontogenesis and anatomy of the TMJ and its cartilage, the risk for growth disturbances is especially high in cases of TMJ arthritis10,12,13. It may result in considerable mandibular dysfunction and dysmorphic facial features such as micrognathia, retrognathism, and mandibular asymmetry, and therefore is of special concern in the pediatric age group5,8,14,15,16. Involvement of the TMJ is often asymptomatic and occurs without clinically detectable signs and symptoms, and the diagnosis is often delayed17,18. When lower jaw asymmetry or retrognathism become obvious, irreversible condylar damage is already established4,19,20. In a previous study we were able to show that magnetic resonance imaging (MRI) is the only method to diagnose TMJ arthritis early, before structural changes have developed21. Because MRI is expensive and small children will need sedation to lie sufficiently still during the examination, better knowledge of factors associated with TMJ arthritis will help to focus screening examinations on patients at risk. The aim of this study was to determine the rate of TMJ involvement with clinical and radiological signs of TMJ arthritis and find factors associated with TMJ arthritis in a single-center cohort of patients with all JIA subtypes.
MATERIALS AND METHODS
Patients
The charts of all patients with JIA visiting the pediatric rheumatology outpatient clinic between January 1, 2005, and December 31, 2006, were reviewed retrospectively for TMJ involvement. Followup information was included until August 2008.
The following data were collected: date of birth, sex, age at onset of JIA, type of JIA, antinuclear antibody (ANA) and rheumatoid factor (RF) status, presence of HLA-B27 (if applicable), date of diagnosis of uveitis (if applicable), and date of diagnosis of TMJ involvement, number and exact location of active joints at each visit, systemic and local medications used during the disease course, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP; at the first visit and at every following visit if available), and blood cell counts (at the first visit).
The study was approved by the Institutional and Cantonal Ethics Review Board.
Methods
For the definition of JIA we used the ILAR Criteria, Edmonton Revision 200122. A diagnosis of TMJ arthritis was based on clinical rheumatological examination and/or radiological examination (contrast-enhanced MRI).
The clinical diagnosis of TMJ arthritis was based on any one of the following findings on rheumatologic examination: (1) the presence of mandibular growth disturbance, i.e., mandibular asymmetry (visible asymmetry of the condylar ramus height in slightly retroflexed head position) or retrognathism (convex appearance of the facial profile on lateral view); (2) reduced maximal mouth opening (< 40 mm maximal interdental distance); and (3) asymmetric mouth opening.
We did not include any pain symptoms as criteria for TMJ arthritis because in our previous study, pain was an unreliable manifestation of active TMJ arthritis21. We chose 40 mm as a cutoff for the maximal mouth opening for all ages as the mouth opening capacity appears to differ much more interindividually than between children of different ages4. A maximal interdental distance of 40 mm was chosen because it is below the mean maximal mouth opening for all age categories23 and has been proposed as a cutoff before6.
The radiological diagnosis of TMJ arthritis was based on any one of the following findings: (1) contrast enhancement of synovial membrane and/or mandibular head on MRI; (2) increased amount of intraarticular fluid on MRI; and (3) destructive changes of the mandibular head.
If a patient fulfilled these criteria in a TMJ at any time during the course of the disease, he/she was deemed to have TMJ involvement for the purpose of this study.
Disease activity
The following variables were calculated based on the findings at each visit and served as substitute markers for JIA disease activity over time: (1) the mean number of active joints present on examination was noted for each visit. The mean number of active joints during the disease course was then calculated by dividing the sum of active joint counts by the number of visits; (2) the mean ESR: the ESR result at each visit (if available) was noted. The mean ESR was then calculated by dividing the sum of ESR results by the number of ESR measurements; and (3) the mean CRP: the CRP result at each visit (if available) was noted. The mean CRP was then calculated by dividing the sum of CRP results by the number of CRP measurements.
Statistical analysis
Statistical analysis was performed using the JMP IN 5.1 software (SAS Institute Inc., Cary, NC, USA). Univariate analysis was performed using 1-way ANOVA or chi-square. Factors significantly associated with TMJ involvement in the univariate analysis were then entered into a multivariate stepwise regression and logistic regression model. A p value ≤ 0.05 was considered to indicate a statistically significant difference.
RESULTS
We found 223 children with the diagnosis of JIA. Patient characteristics are described in Table 1. The sex ratio was 1.6:1 girls:boys (138 girls and 85 boys), the median age at the time of JIA diagnosis was 5.2 years (range 0.6–17.6), and the median disease duration was 6.95 years (range 0.82–16.3). In 102/223 patients (45.7%), at least 1 MRI examination of the TMJ was available.
Patient characteristics.
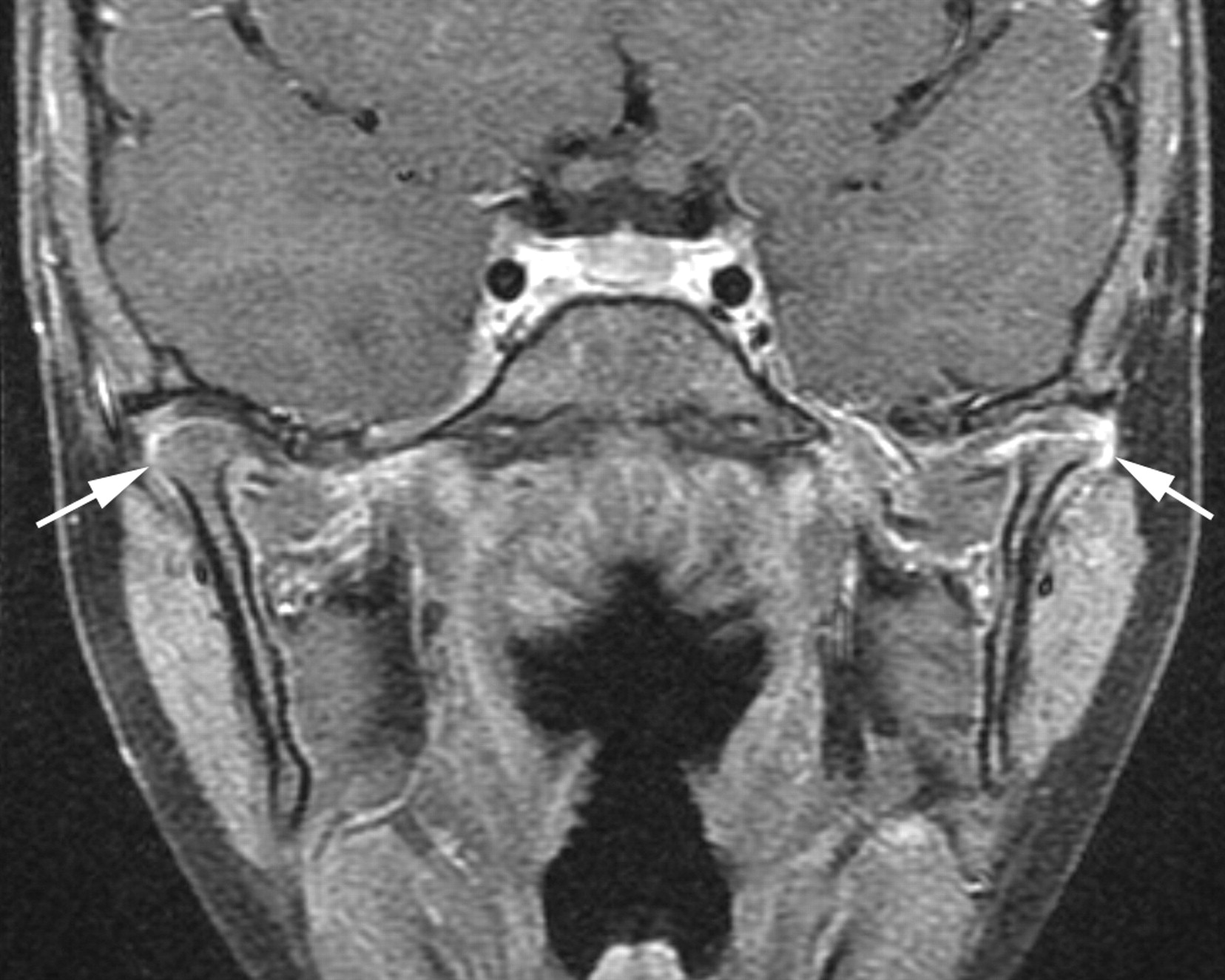
In a total of 86 patients (38.6%), a diagnosis of TMJ arthritis was made after a mean followup time for JIA of 4.6 years (range 0.08–14.17). The sex ratio in this group was 2.4:1 girls:boys (61 girls and 25 boys). Characteristics of the patients with TMJ arthritis are listed in Table 1. Most patients with TMJ pathology (61/86) met both clinical and radiological criteria. Sixty-one patients had contrast-enhanced MRI with signs of inflammation and/or destruction of the mandibular head (Figure 2). Fourteen patients met the radio logical criteria for TMJ involvement and 11 children had clinical signs for TMJ pathology, but no MRI had been performed. Details about the criteria met for the diagnosis of TMJ pathology are listed in Table 2.

The percentage of patients with temporomandibular joint (TMJ) involvement according to juvenile idiopathic arthritis (JIA) subtype. Solid horizontal line depicts the overall rate of TMJ involvement (38.6%) in the cohort.

Magnetic resonance image of temporomandibular region of a 5-year-old girl 2 years after diagnosis of polyarticular RF-negative JIA. With no previous symptoms of TMJ arthritis, she was found to have mandibular asymmetry with growth delay on the left side. MRI revealed severe destruction of the left condylar head and bilateral synovial contrast enhancement (arrows).
Criteria fulfilled for the diagnosis of TMJ involvement.
The rate of TMJ involvement differed significantly among JIA subtypes (p = 0.016, chi-square for difference between the groups), with a maximum of 61% of TMJ involvement in extended oligoarticular JIA and a minimum of 11% in enthesitis-related arthritis (ERA; Figure 1).
Systemic medication used at any time during the disease course included nonsteroidal antiinflammatory drugs (NSAID), systemic corticosteroids, methotrexate (MTX), tumor necrosis factor-α (TNF-α) antagonists, leflunomide, hydroxychloroquine, sulfasalazine, and cyclosporine (Table 1). Nearly 90% of the patients with TMJ involvement had MTX as systemic medication, among them 20 patients of the oligoarticular JIA subtype. The reasons for the systemic medication with MTX in this subtype of JIA were uveitis in 4 patients and in the others, and persistence of arthritis despite several local corticosteroid injections.
Factors associated with TMJ arthritis
In the univariate analysis, the development of TMJ arthritis was associated with the JIA subtypes extended oligoarthritis, RF-negative polyarthritis, and psoriatic arthritis, while ERA was associated with a low risk for TMJ involvement (p = 0.006 for the difference between the subtypes). Other associations included younger age at onset of JIA (p = 0.0008), higher mean number of active joints at each visit (p = 0.005), involvement of joints of the upper extremity (p < 0.0001), polyarticular joint involvement (p = 0.0026), involvement of the cervical spine (p = 0.003), higher ESR at diagnosis (p = 0.03), and longer duration of JIA (p < 0.0001). In addition, girls (61/138) were more likely to develop TMJ arthritis than boys (25/85; p = 0.02).
HLA-B27 was positive in 24/145 patients tested (16.5%) of the total cohort and in 2/62 (3.2%) patients with TMJ arthritis. There was a statistically significant inverse correlation between the presence of HLA-B27 and TMJ involvement in our cohort (p = 0.0002).
Factors not associated with TMJ arthritis were a diagnosis of uveitis, ANA or RF positivity, CRP at onset, or mean ESR and mean CRP during disease course.
In the multivariate analysis, the following factors were independently significantly associated with TMJ involvement: (1) JIA subtype [likelihood ratio (LR) chi-square 14.8, p = 0.0001]; (2) higher ESR at diagnosis (LR 8.8, p = 0.003); (3) involvement of upper extremity joints (LR 6.4, p = 0.0113); (4) negative test for HLA-B27 (LR 5.2, p = 0.0224); and (5) younger age at diagnosis of JIA (LR 3.8, p = 0.050).
DISCUSSION
In our retrospective study we evaluated the rate of TMJ involvement in an inception cohort of 223 patients with JIA followed at a single center. Special emphasis was placed on the search for factors associated with TMJ arthritis that could help to focus screening examinations on patients at risk. In addition to the clinical examination, MRI of the TMJ had been performed in nearly half of our patients. This is important because MRI examination is assumed to be the gold standard for the diagnosis of TMJ arthritis, especially in the early phases of the disease before growth disturbances have developed6,21,24,25,26,27,28,29. We found that patients with the JIA subtypes extended oligoarthritis, RF-negative polyarthritis, and psoriatic arthritis, and patients with a higher ESR at diagnosis, with involvement of upper extremity joints and a younger age at disease onset, had an increased rate of TMJ arthritis, while the presence of HLA-B27 seemed to be protective.
The overall rate of TMJ involvement in our cohort was 38.6%. The frequency of TMJ arthritis in patients with JIA reported in the literature varies from 17% to 87%3,5,6,7,28,29. A possible reason for this wide range is the different methods used to diagnose TMJ arthritis. Many studies used orthopantomogram changes of the mandibular condyle for the diagnosis4,5, a sign occurring rather late in the course of TMJ arthritis. In contrast, studies using MRI found a surprisingly high number of joints with inflammatory signs, especially in recently diagnosed patients26. Also, most studies did not include all patients with JIA seen at a center but chose a smaller group of patients. This may have resulted in a higher probability of patients with more active disease or who had clinical symptoms participating in the study, leading to a higher rate of TMJ arthritis. Thus, compared with other recent studies, our rate of TMJ involvement seems to be low. At our institution, MRI is performed whenever the result may influence treatment decisions, irrespective of the age of a patient. Despite the relatively high number of MRI in our cohort, possible TMJ involvement in patients without obvious clinical signs may have been missed in those who did not undergo MRI.
Some studies have reported a higher rate for TMJ involvement in certain JIA subtypes2,4,12,30, while others5 found similar frequencies. Our study showed a significant difference of TMJ involvement among the different JIA subtypes, with the highest rate in extended oligoarticular and RF-negative polyarticular JIA. This is in keeping with the results of other studies, where factors such as polyarticular disease, younger age at onset of JIA, and a longer disease duration were associated with TMJ arthritis4,8,17,30. In contrast, we did not find an association with ANA positivity, as others did2. A surprising result that to our knowledge has not been reported earlier was the association with involvement of joints of the upper extremity and a higher ESR at onset. On the other hand, involvement of the cervical spine has been reported to be associated with TMJ involvement31. In our study, the association between cervical spine involvement and TMJ arthritis found in the univariate analysis was not confirmed to be an independent factor in the multivariate model.
Pedersen, et al2 found that patients with JIA who were HLA-B27-positive had no signs of TMJ involvement, neither in the clinical findings nor in orthopantomograms. In Kuseler, et al28 the only patient with a positive HLA-B27 was also the only patient with virtually no TMJ abnormalities on MRI over time. In our study, the presence of HLA-B27 was associated with a significantly reduced rate of TMJ involvement. A possible confounder could be the fact that HLA-B27-positive patients tend to have a later age of JIA onset compared to HLA-B27-negative patients. Also, HLA-B27 positivity is associated with ERA, the JIA subtype with the lowest rate of TMJ involvement in our cohort. However, in our study population, HLA-B27 was independently associated with a reduced rate of TMJ involvement and it also had a stronger association than age at onset of JIA.
Our study is limited because of its retrospective design, the relatively small number of patients, and the fact that MRI was performed in only about half of the patients. Because of these factors, we may have underestimated the number of patients with TMJ involvement and we may also have missed factors with weaker association.
The development of TMJ arthritis in our cohort was strongly associated with JIA subtype, high ESR at disease onset, involvement of upper extremity joints, and a younger age at onset of JIA. The presence of HLA-B27 was protective.
Early recognition of TMJ arthritis is important for rheumatologic and orthodontic diagnosis and treatment planning. We propose to perform contrast-enhanced MRI of the TMJ in every patient with JIA, particularly in patients with extended oligoarticular, psoriatic, or RF-negative polyarticular JIA, with a high ESR, upper extremity involvement, negative HLA-B27, and young age at onset of JIA. We consider contrast enhancement essential for the diagnosis of synovial inflammation on MRI; however, because of reports of nephrogenic systemic fibrosis associated with gadolinium in patients with renal impairment32, the use of gadolinium-based contrast agents should be limited to patients with normal renal function. Prospective studies are needed to find further factors associated with TMJ involvement and to develop a feasible screening method for the early diagnosis of TMJ arthritis in patients with JIA.
- Accepted for publication October 13, 2010.








{kind=link}
{kind=link}