

Abstract
Objective. Maternal anti-SSA/Ro or anti-SSB/La antibodies are associated with neonatal lupus erythematosus syndrome (NLES), especially congenital heart block (CHB), which may be associated with severe endocardial fibroelastosis (EFE) and dilated cardiomyopathy (DCM). A few reports have described severe EFE without CHB associated with anti-SSA/Ro antibodies, with a poor prognosis. EFE has also been observed in biopsies of DCM that had been considered idiopathic. These points, considered in association with 5 unusual cases of mild EFE, led us to consider the relationship between underrecognized cases of isolated autoantibody-associated EFE and DCM that had been considered idiopathic.
Methods. We analyzed 5 cases of EFE diagnosed in utero (n = 4) or after birth (n = 1). In 3 cases, maternal antibody status was discovered because of the EFE diagnosis.
Results. Endomyocardial hyperechogenicity predominated in the left atrium (n = 3) and mitral annulus (n = 3). No left-heart dysfunction was observed. Two mothers were treated with betamethasone. One mother chose to have a therapeutic abortion, and EFE was confirmed at autopsy. Electrocardiograms at birth (n = 4) did not show CHB. Other manifestations of NLES were present in all cases. One child had right ventricular hypoplasia and underwent a partial cavopulmonary anastomosis. At last followup (4–7 yrs), the other 3 children had normal heart function, and echocardiography showed a normal heart (n = 2) or mild persistent EFE (n = 1).
Conclusion. Middle-term prognosis of isolated autoantibody-associated EFE may be better than previously reported, although the longterm prognosis remains unknown. We hypothesize that a fetal insult can lead to DCM.
- ENDOCARDIAL FIBROELASTOSIS
- PREGNANCY
- ANTI-SSA/Ro ANTIBODIES
- CONGENITAL HEART BLOCK
- NEONATAL LUPUS ERYTHEMATOSUS SYNDROME
Mothers known to have anti-SSA/Ro or anti-SSB/La antibodies are at risk of delivering babies with neonatal lupus erythematosus syndrome (NLES), characterized by some combination of transient lupus dermatitis, hepatic and hematologic abnormalities, and congenital heart block (CHB)1. Rash, hepatitis, and thrombocytopenia generally resolve without sequelae. By contrast, CHB is permanent and often requires pacemaker implantation. Other cardiac manifestations include transient fetal first-degree heart block, sinus bradycardia, late-onset dilated cardiomyopathy (DCM), endocardial fibroelastosis (EFE), and minor cardiac malformations2,3,4.
The association of EFE with autoantibody-associated CHB was first reported by Hogg in 19575. In 2002, Nield, et al6 described 13 children with complete CHB, associated with EFE predominantly involving the left ventricle. Severe ventricular dysfunction was present in all cases and led to death in 9 and cardiac transplantation in 2. The same year, those authors also reported 3 cases of severe EFE, mainly ventricular, in children without CHB born to mothers with anti-SSA/Ro antibodies7.
DCM is the most common cardiomyopathy in children. Most cases are idiopathic. Endomyocardial biopsy shows EFE in some cases8.
We describe 5 cases of isolated EFE that were substantially less severe than in these reports. Such cases may easily be underrecognized; this could explain later apparently idiopathic DCM.
MATERIALS AND METHODS
Patients
In 4 cases, the fetal cardiac abnormalities were discovered during the second fetal ultrasound, usually performed in France between 20 and 22 weeks of gestation. The mothers were then referred to experienced pediatric cardiologists, who performed fetal echocardiography.
Autoantibody determination
Anti-SSA/Ro and anti-SSB/La antibodies were determined with INNO-LIA ANA Update (Innogenetics, InGen, Chilly-Mazarin, France), a semiquantitative line immunoassay for detection of antibodies against SSA 52 kDa, SSA 60 kDa, and SSB 48 kDa.
Definition of CHB and EFE
First-degree heart block was described as prolongation of the PR interval (> 150 ms in utero)9. Echographies were performed with a Hewlett Packard 5500 for Cases 1 and 3, a General Electric Vivid 7 for Cases 2 and 4, and an Acuson for the last one, using an ultrasound probe of 5 MHz in all cases. EFE was identified as marked areas of endocardial echogenicity, bright and white, with clearly defined margins. Localization of fibrosis should be on the surface of the right ventricle, left ventricle, left atrium, right atrium, or mitral valve. It was confirmed histologically in 1 case. Severity was evaluated according to the extent and the thickness of myocardial involvement as mild, moderate, or severe. All neonates had a 12-lead electrocardiograph (ECG), and the findings were compared with the normal values for age collected by Davignon, et al10. All patients had echocardiography. DCM was defined as left ventricular end-diastolic diameter > 97th percentile, associated with a shortening fraction < 25%.
RESULTS
Case 1
In 2004, a 32-year-old patient was referred to a pediatric cardiologist at 22 weeks of gestation for suspected cardiopathy of her fetus, first observed at the ultrasound performed that week. She had previously given birth to a healthy girl and was symptom-free except for Raynaud’s phenomenon.
The fetal heart was hyperechogenic, with thickening of the left atrium, mainly on the mitral annulus and the left atrial appendage (Figure 1). The aortic annulus and the endocardial region of the right ventricular lateral wall were also mildly hyperechogenic. No heart dysfunction or CHB was noted. Because this was very similar to the appearance of EFE encountered in some fetuses with autoantibody-associated CHB, the pediatric cardiologist requested that the mother be tested for anti-SSA/Ro and anti-SSB/La antibodies. She had antinuclear antibodies (titer of 1/1280) and antibodies to 52 kDa SSA/Ro, 60 kDa SSA/Ro, and 48 kDa SSB/La ribonucleoproteins. Results for antibodies to dsDNA and antiphospholipids were negative.

Case 1 at 22 weeks. Hyperechogenicity of the fetal heart with thickening of the left atrium, predominantly on the left atrial appendage and the mitral annulus (arrows).
In view of the absence of CHB and of heart dysfunction and given the mainly atrial hyperechogenicity, close monitoring was implemented, but no treatment given. The echocardiography remained unchanged during pregnancy, except for PR interval, which was measured weekly from Week 22 to Week 30 and ranged from 150 to 180 ms. It was not measured thereafter.
At 39 weeks, she delivered a healthy boy weighing 3200 g. At birth, the 12-lead ECG showed normal atrioventricular conduction with a fetal heart rate of 120 bpm. Atrial EFE was mild and the echocardiography was otherwise normal. The right ventricular hyperechogenicity disappeared. A 24-hour ECG at 2 months was normal.
The child had cutaneous lesions of neonatal lupus from the age of 3 weeks to 5 months. Additionally, although normal at birth (50th percentile), head circumference exceeded the 97th percentile at 3 months, and magnetic resonance imaging (MRI) showed hydrocephalus, maximal at 6 months. By the age of 1 year, both head circumference and MRI had returned to normal.
Regular cardiologic followup through the age of 4 years showed only mild hyperechogenicity of the left atrium, mainly on the mitral annulus. Echocardiography was otherwise normal.
At 4 years of followup, the child was healthy and developing normally and the mother remained symptom-free (except for Raynaud’s phenomenon).
Case 2
In 2004, a primiparous 31-year-old was seen at 22 weeks for scheduled fetal ultrasound. Her history of systemic lupus erythematosus (SLE) dated from 1998 and included arthritis, skin involvement, and anti-dsDNA, anti-SSA/Ro 60 kDa, and anticardiolipin antibodies. She was treated during pregnancy with hydroxychloroquine (HCQ) 400 mg/day, prednisone 10 mg/day, preventive low molecular weight heparin (LMWH), and aspirin 100 mg/day. The pregnancy was otherwise uneventful.
Ultrasound examination of the fetal heart showed hyperechogenicity of the interventricular septum, the mitral and aortic annuli, and the emerging aortic and pulmonary vessels. The fetal heart rate was 147 bpm and atrioventricular conduction was normal. No treatment was added. No changes were seen at 30 weeks.
She delivered a healthy 1750 g girl at 35 weeks. The ECG at birth was normal, as was the echocardiography at 15 days. Cutaneous neonatal lupus lesions were present at birth and disappeared around 1 year with mild sequelae on the eyelids. Regular cardiologic followup through the age of 4 years showed normal ECG with a completely normal heart on echocardiography.
The mother, who continued treatment with HCQ 400 mg/day, prednisone 10 mg/day, and aspirin 100 mg/day, had a second child in 2007. This baby had cutaneous neonatal lupus but no cardiac involvement.
Case 3
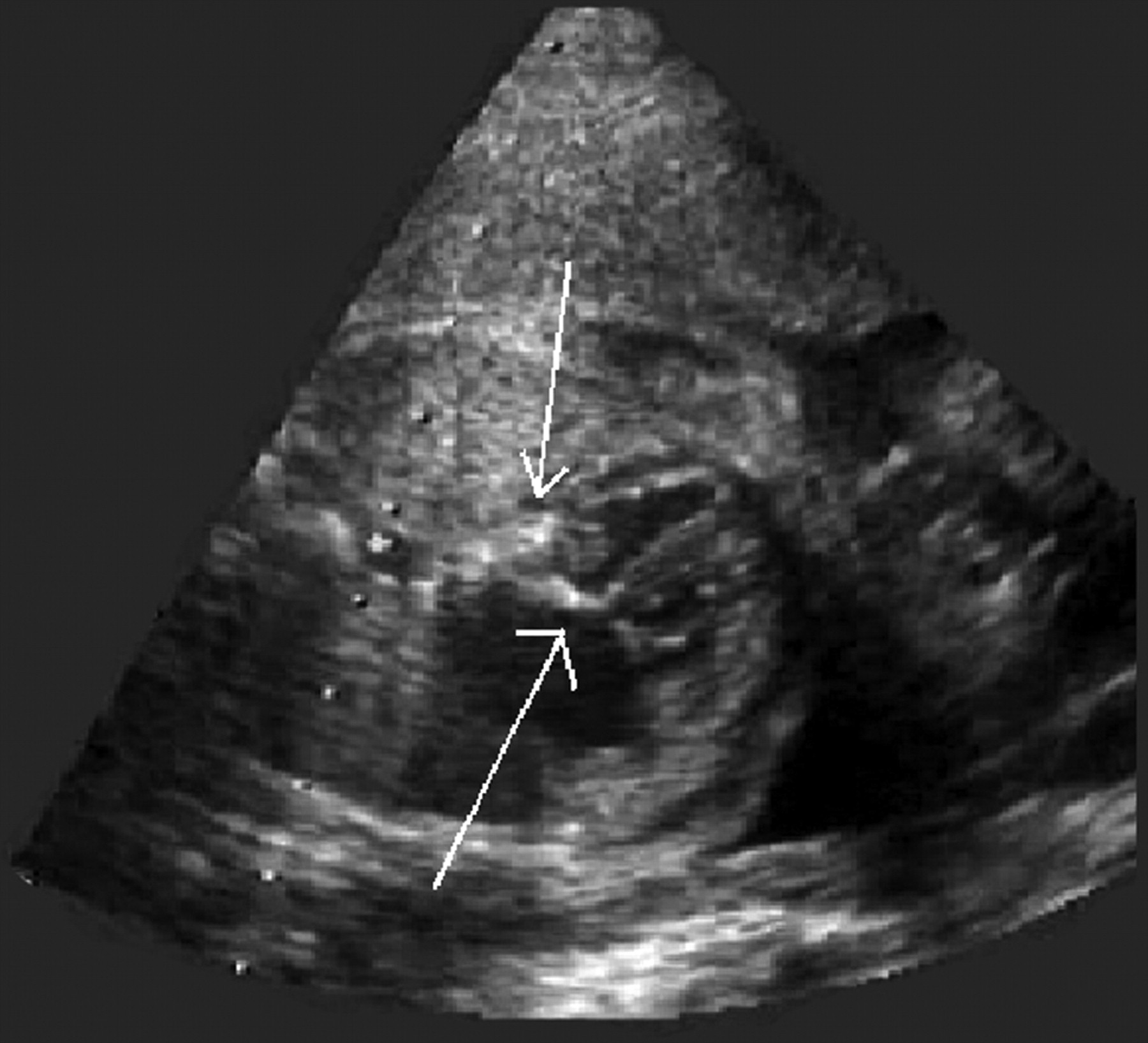
In 2005, a healthy 30-year-old hospital nurse who had previously given birth to a healthy boy was referred at 27 weeks for suspected cardiopathy of her fetus after the routine 22-week ultrasound. Echocardiography (Figure 2) of the fetal heart showed left atrial hyperechogenicity and thickening, especially of the mitral annulus. Cardiac function was normal. Mild pericardial effusion was present. The fetus also had sinus bradycardia, with a heart rate between 90 and 120 bpm, and 1:1 atrioventricular conduction. Testing for anti-SSA/Ro 60 kDa, 52 kDa, anti-SSB/La antibodies, and antinuclear antibodies (1/1280) was positive, while anti-dsDNA antibodies were negative. Antiphospholipid tests were negative except for IgM anti-ß2-glycoprotein I antibodies (0.260 MPL units, normal < 0.200). Due to the abnormal heart rate, betamethasone was started at 27 weeks (4 mg/day), and the echocardiography findings remained stable.

Case 3 at 27 weeks. Hyperechogenicity predominantly on the left atrium and especially on the mitral annulus (solid arrows). The left atrium was thickened. Mild pericardial effusion was present (broken arrow).
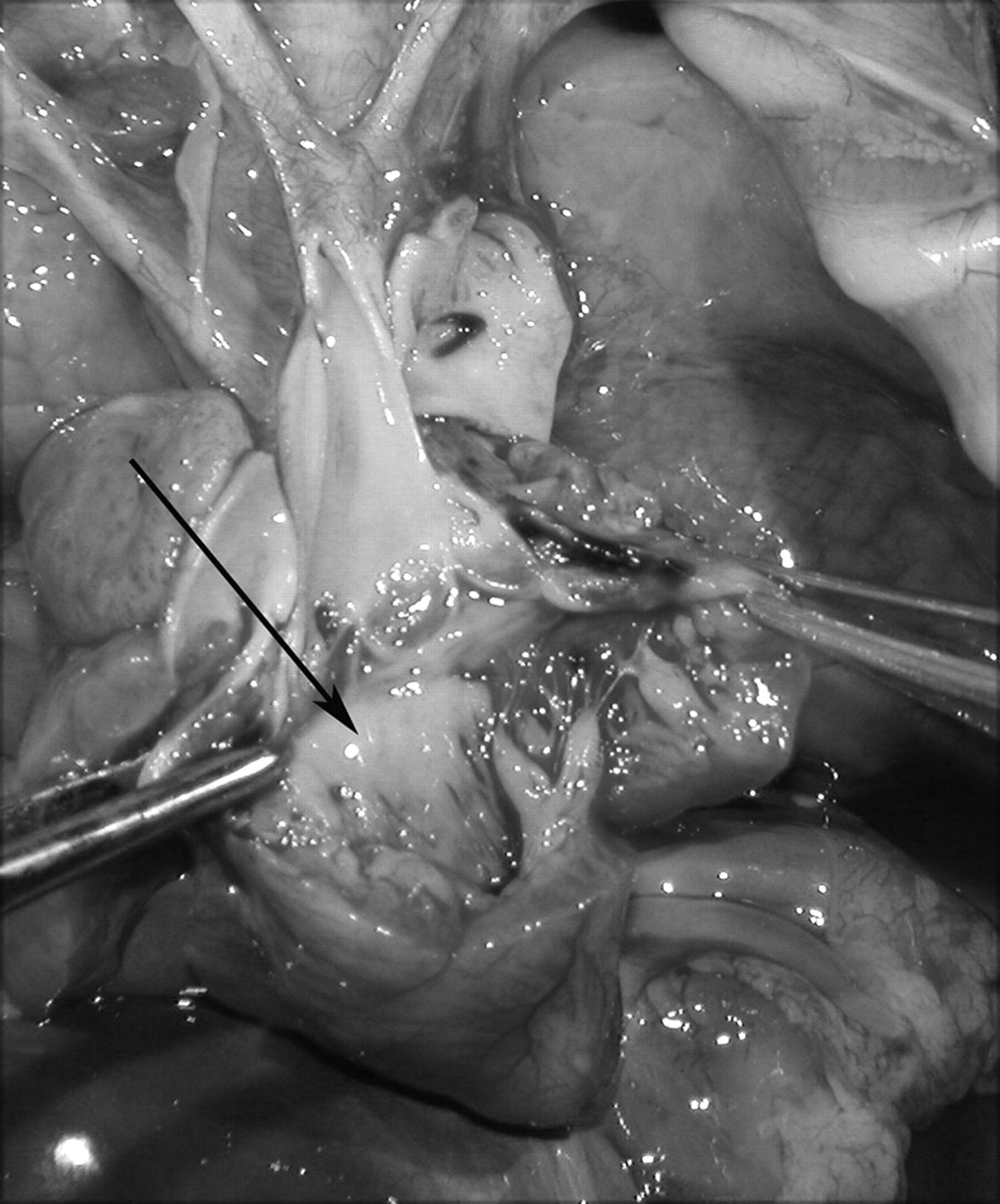
The nurse, who worked in an adult cardiologic unit, was very concerned about the risk of late DCM and requested a medical abortion. The ethics committee agreed, and the pregnancy was terminated at 30 weeks. Postmortem examination of the dead male fetus, weighing 1730 g, confirmed EFE localized on the left atrium and in the interventricular septum (Figures 3 and 4).

Case 3. Macroscopic study of the heart. After opening of the small left ventricle and the aortic arch, endocardial fibroelastosis was seen in the mitral annulus and corresponded to the thickened and bleached area (arrow).

Case 3. Histopathologic examination of the interventricular septum (H&E stain, original magnification ×200). The subendocardial layer was thickened by a homogeneous organizing fibrosis with area of hyalinization. Fibrosis contained abnormal angiogenesis and diffuse microcalcifications (arrow).
Subsequently the mother was treated with prednisone 10 mg/day and aspirin 100 mg/day, and she gave birth to a healthy boy in 2006. She finally developed arthritis in August 2007 and now requires treatment with HCQ and prednisone.
Case 4
In 2001, a 35-year-old patient was referred at 23.5 weeks. She was first diagnosed with SLE in 1999, with arthritis, skin involvement, positive antinuclear antibodies (1/1280), and anti-dsDNA, anti-RNP, and anti-Sm antibodies. She had sicca syndrome and antibodies to 52 kDa SSA/Ro, 60 kDa SSA/Ro, and 48 kDa SSB/La ribonucleoproteins. She also had antiphospholipid syndrome, defined by a fetal death with anticardiolipin and anti-ß2-glycoprotein I antibodies. She had previously given birth to 3 children including the one described as Case 5.
During pregnancy, she was treated with prednisone 10 mg/day, LMWH, and aspirin 160 mg/day. She was referred to a pediatric cardiologist for suspected fetal cardiopathy, first seen at 22 weeks during the routine ultrasound examination. The endocardial surface of the left atrial area and the mitral, tricuspid, and aortic annuli were the predominant areas of increased echogenicity. Mild pericardial effusion was seen. The fetal heart rate was 145 bpm, with normal atrioventricular conduction, but a transient supraventricular tachycardia was observed, with a heart rate of 280 bpm.
Maternal treatment with amiodarone (800 mg/day and then 400 mg/day after 1 week) and betamethasone (8 mg/day) was instituted at 24 weeks. At 28 weeks, those treatments were stopped and replaced by digoxin and prednisone (10 mg/day). Close monitoring continued. The echocardiography did not change during pregnancy (Figure 5).

Case 4 at 28 weeks. Increased echogenicity was predominantly seen in the left atrial area, especially on the mitral (solid arrow) and tricuspid annuli (arrowhead). Mild pericardial effusion was seen (hatched arrow).
She gave birth at 33 weeks to a 1655-g girl. The ECG performed at birth was normal. Recurrence of the transient supraventricular tachycardia was treated with amiodarone until the baby reached the age of 8 months, with no relapse. At birth, cutaneous neonatal lupus lesions, mainly on the face, were associated with thrombocytopenia (27/mm3) and neutropenia (160/mm3). The hematological abnormalities resolved at 1 month and the cutaneous lesions were gone by 6 months.
Regular cardiologic followup through the age of 7 years showed a normal ECG. Echocardiography showed mild hyperechogenicity of the mitral annulus, but the lesions were so mild that they were seen only inconsistently during the first years. Left ventricular function always remained normal. At 7 years, the echocardiogram was considered normal.
In 2006, the mother developed a nephritic syndrome related to class IV lupus glomerulonephritis. She was treated with steroids and intravenous cyclophosphamide.
Case 5 (older sister of Case 4)
The mother of Case 4 had had 3 children before her SLE diagnosis. The third (Case 5) was a girl born in 1992. At that time, the mother was symptom-free and the diagnosis of EFE for Case 5 was made retrospectively, when Case 4 was diagnosed with EFE.
Apparently, no cardiac abnormalities had been diagnosed in utero (no data were retrospectively available). The baby was born at a gestational age of 36.5 weeks, weighed 2120 g (between the third and tenth percentiles), and had a right-to-left atrial shunt due to right ventricular abnormalities: the right ventricle was small, with a bright endocardium, especially on the tricuspid annulus; the right ventricular apex was filled, and the tricuspid annulus was small. The pulmonary annulus was also small, with a thickened pulmonary valve. EFE was identified on the mitral annulus. Left ventricular dimensions and function were normal. ECG showed a normal sinus rhythm. She had required mechanical ventilation for the first 3 days of life. Under treatment with ß-blockers, her clinical status improved somewhat. She developed cutaneous lesions that retrospectively were concordant with NLES. Because of her low exercise tolerance with low saturation, she underwent surgery at 6 years for partial cavopulmonary anastomosis with closure of the atrial defect. At the age of 17 years, ultrasound showed hyperechogenicity only on the right ventricle, which remained abnormal, with less contractility and thin walls. Mild tricuspid regurgitation was observed on right atrial dilatation.
Summary: Four mothers had 5 fetuses/children with EFE but not CHB. All mothers had anti-SSA/Ro antibodies, and 3 had anti-SSB/La antibodies. Two mothers had SLE and 2 were symptom-free.
The main EFE sites were the left atrium (especially the mitral annulus), and the aortic and tricuspid annuli.
Echocardiography indicated that only Case 2 had left ventricular involvement (mild hyperechogenicity of the interventricular septum). Postmortem examination of Case 3 also showed EFE in the interventricular septum. No left-heart dysfunction was seen. Pericardial effusion was present in 2 cases.
The appearance of EFE on fetal echocardiography remained stable, regardless of treatment (betamethasone in 2 cases). One pregnancy was medically aborted at 30 weeks (Case 3). The remaining 4 fetuses (3 girls and 1 boy) were delivered between 33 and 39 weeks. All 4 children had NLES, including cutaneous (n = 4), hematological (n = 1), and neurological (n = 1) involvement11.
ECG at birth excluded CHB in all cases. In Case 1, the PR interval was transiently prolonged in utero, probably corresponding to transient fetal first-degree heart block. Despite the absence of maternal treatment, ECG was normal at birth. Supraventricular tachycardia was seen in 1 fetus and disappeared during followup (Case 4). Sinus bradycardia was observed in Case 3 at 27 weeks. The evolution was not known because medical abortion was requested. Case 5, who had the most severe EFE with significant right ventricular involvement, required surgery at the age of 6. At last followup at a mean of 5 years, the remaining 3 children were doing well. Echocardiography was considered normal in 2 and showed only mild EFE in 1. These data are summarized in Table 1, which also includes 2 previous case reports12,13.
Demographic data and followup of 4 mothers and 5 fetuses and review of literature of cases with good prognosis. No fetuses or children had severe left ventricular dysfunction.
Of note, this echocardiographic appearance, involving predominantly the mitral and aortic annuli, appears quite specific since neither of the pediatric cardiologists has observed other fetuses with a similar appearance in cases without anti-SSA or anti-SSB antibodies.
DISCUSSION
We describe a series of 5 cases with mild antibody-associated EFE without CHB. Their presentation contrasts with previous reports about the severity of EFE: No extensive ventricular localization and no left-heart dysfunction were seen in any of our patients. EFE was not confirmed by endomyocardial biopsy because of its mild severity, except in Case 3, in which postmortem examination found it more diffuse than the echocardiogram had indicated. Followup showed satisfactory development in the remaining 3 children.
It is highly probable that EFE was related to NLES since maternal antibodies were present in all cases and all infants had NLES cutaneous manifestations. Additionally, Case 1 had reversible macrocephaly with hydrocephalus, which has been recognized as a neurological manifestation of NLES11, and Case 4 probably had hematological involvement14.
We found only 2 similar cases in the literature. The first was reported by Raboisson, et al12. Multiple areas of hyperechogenicity in the 2 ventricles and the 2 atrioventricular annuli, consistent with EFE, were observed at 29 weeks, without CHB. The mother received dexamethasone, and the followup showed a progressive decrease in hyperechogenicity, so that only mild hyperechogenicity of the tricuspid annulus was still visible at birth. The ultrasound at 3 months of age was considered normal. The second case was reported by Pises, et al13. At 25 weeks, EFE involving the right ventricle was observed, associated with mild pericardial effusion and tricuspid regurgitation. No CHB was seen. The mother was treated with intravenous immunoglobulin and dexamethasone. Echocardiography of the baby at 4 months of age showed brightness of the tricuspid alone, with trace tricuspid regurgitation. EFE is a rare disease that involves the endomyocardium, and usually leads to endstage heart failure or death in early infancy6. Hyperechogenicity can involve the 4 cavities, the mitral valve, and the papillary muscles6 but most frequently the 2 ventricles6,7. The diagnosis is definitively established only by pathological analysis of the heart, which typically shows collagen and elastin deposition, ventricular hypertrophy, and diffuse endocardial thickening. Known causes include viral infections, primary carnitine deficiency, metabolic disorders, and hereditary transmission. Recently, Nield, et al6 pointed out a link to anti-SSA/Ro antibodies in their report of 13 children with complete CHB and EFE predominantly involving the left ventricle. Diagnosis was confirmed on autopsy or by echocardiography. EFE was diffuse, and severe ventricular dysfunction was present in all cases, leading to death (n = 9) or cardiac transplantation (n = 2). Immunohistochemical staining demonstrated significant deposition of both IgG and IgM, with T cells present in 3 of the 4 cases that studied them. This suggests that a fetal factor is involved in the immune process leading to EFE. Others have confirmed the severe prognosis of CHB associated with EFE15.
Additionally, Nield, et al7 reported 1 fetus and 2 children with severe EFE associated with anti-SSA/Ro antibodies and without CHB. One fetus and 1 child aged 3 months died; the third child received a cardiac transplant in infancy. Our patients’ prognoses were less severe: left ventricle involvement was present in only 1 fetus and was moderate.
All our cases but 1 were diagnosed prenatally. Remarkably, the echocardiogram did not change in any case during the in utero period. Moreover, EFE improved after delivery and even disappeared in 2 cases, followed closely by experienced pediatric cardiologists with serial echocardiograms. This was observed regardless of maternal treatment during pregnancy. Nield, et al6 also noticed that echocardiography tends to overestimate the severity of EFE among fetal cases and underestimate it in postnatal cases. We hypothesize that this is due to better visibility of the heart, especially the atria, during the in utero period when there is no air in the lungs. The point is important because improvements after birth may be inaccurately attributed to maternal treatment.
Treatment of such cases remains highly questionable. Fluorinated steroids (dexamethasone or betamethasone) have been shown to improve myocarditis in some fetuses with CHB, although their effects on complete heart block remain disappointing6,16,17. In Nield’s series of 3 patients, 1 mother received dexamethasone on diagnosis, but ventricular dysfunction led to the baby’s death 1 week later7. In the series of 13 EFE cases with complete block, 6 cases were diagnosed prenatally: 5 of them had hydrops fetalis and all died in utero, despite maternal dexamethasone treatment in 3 cases. The mother of the only case with no hydrops and with mild EFE was treated with dexamethasone. The child survived but no information was available about the efficacy of dexamethasone on EFE6. In the PRIDE study (PR Interval and Dexamethasone Evaluation), Friedman, et al reported the outcome of 98 prospective pregnancies in 95 women with anti-SSA/Ro and/or anti-SSB/La antibodies in order to search for early markers for third-degree CHB9. Atrial hyperechogenicity was diagnosed at 22 weeks in 1 case with normal PR interval. Third-degree CHB appeared after the diagnosis of EFE, at 23 weeks. Despite introduction of dexamethasone, fetal death occurred at 24 weeks, related to severe hydrops9. The 2 other case reports of mild EFE without CHB12,13 seemed to show that maternal treatment had a favorable effect, but this must be interpreted cautiously in view of the spontaneous “improvement” we observed in echocardiograms after birth. Our short series does not suggest that the use of betamethasone affected the outcome. The efficacy of fluorinated steroids on EFE remains essentially unclear, and these treatments may be associated with hydrops, stillbirth, and intrauterine growth restriction, all adverse obstetric outcomes similar to those observed in Cushing syndrome16,18.
DCM represents a heterogeneous group of diseases with multiple etiologies. Although specific causes can be identified in some cases, such as congenital heart disease or metabolic disease, most cases are idiopathic, and EFE can be found in such cases, as reported by Matitiau, et al8. No DCM occurred during the followup of our patients. In view of the close relationship between EFE and DCM and because the potential for mild EFE and the possibility of symptom-free mothers render diagnosis difficult, we believe that a search for antibodies should be done whenever possible in mothers of children with EFE or idiopathic DCM.
The main limitations of our study include its small size and the absence of histological confirmation in 4 cases. However, areas of echogenicity were unquestionably unusual. They were associated with an uncommon atrial and annular stiffness, which is never seen in a normal fetal heart, and echography has been considered sufficient for diagnosis of EFE6.
Finally, 2 reasons make it important to call attention to these cases. First, mild isolated fetal EFE is probably under-recognized. Second, these cases require longterm followup. Only through such followup can we answer the ultimate question of the longterm prognosis of these children, especially their risk of late-onset cardiomyopathy or of idiopathic DCM in adulthood.
- Accepted for publication September 17, 2010.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}