

Abstract
At the 2008 meeting of GRAPPA (Group for Research and Assessment of Psoriasis and Psoriatic Arthritis), the primary focus of the imaging session was the enthesis. Presentations from Dennis McGonagle (Leeds, UK), Richard Hodgson (Leeds, UK), and Paolo Gisondi (Verona, Italy) elaborated on this theme and prepared the meeting attendees for group discussions of further work in this area. Imaging, notably magnetic resonance imaging (MRI) and ultrasonography, provides evidence of pathological change at the enthesis in psoriatic arthritis (PsA). Further, imaging abnormalities are found at sites that are asymptomatic in both PsA and psoriasis. The role of newer imaging modalities, such as ultra-short echo time (UTE) MRI, is promising but remains to be fully elucidated. The implication of these findings in relation to subclinical and predisease status is intriguing and requires further study in longitudinal studies. Further work is also required to examine the proposed common biomechanical basis between joint and skin, the mechanism of the resulting inflammation, and how these mechanisms differ from those seen in rheumatoid arthritis.
The first of 3 plenary sessions held at the GRAPPA (Group for Research and Assessment of Psoriasis and Psoriatic Arthritis) 2008 Conference in Leeds, United Kingdom, was on imaging, chaired by Philip Helliwell and Paolo Gisondi. Laura Coates gave a brief summary of the imaging session from the 2007 GRAPPA meeting in Boston, MA, USA, which was followed by the 3 major speakers: Dennis McGonagle, Richard Hodgson, and Paolo Gisondi; Arthur Kavanaugh also made a brief supplementary presentation. These primary presentations were followed by breakout group discussions and a final plenary discussion involving all attendees.
The synovio-entheseal complex: Dennis McGonagle
Dr. McGonagle introduced concepts related to the “enthesis organ” and the “synovio-entheseal complex”1–3. Using elegant detailed imaging and cadaveric histology, he elaborated on the proposed common biomechanical basis between joint and skin and on the proposed mechanism of inflammation that demarcates psoriatic arthritis (PsA) from other forms of inflammatory arthritis such as rheumatoid arthritis (RA; Figure 1). Microdamage and microinflammation in the synovio-entheseal complex may be the forerunner of frank enthesitis and entheseal erosion and, subsequently, inflammation in adjacent synovial structures. Some of the differences between the inflammatory arthritides may be related to tissue-specific factors. Dr. McGonagle illustrated this in relation to several immune and non-immune-related conditions.
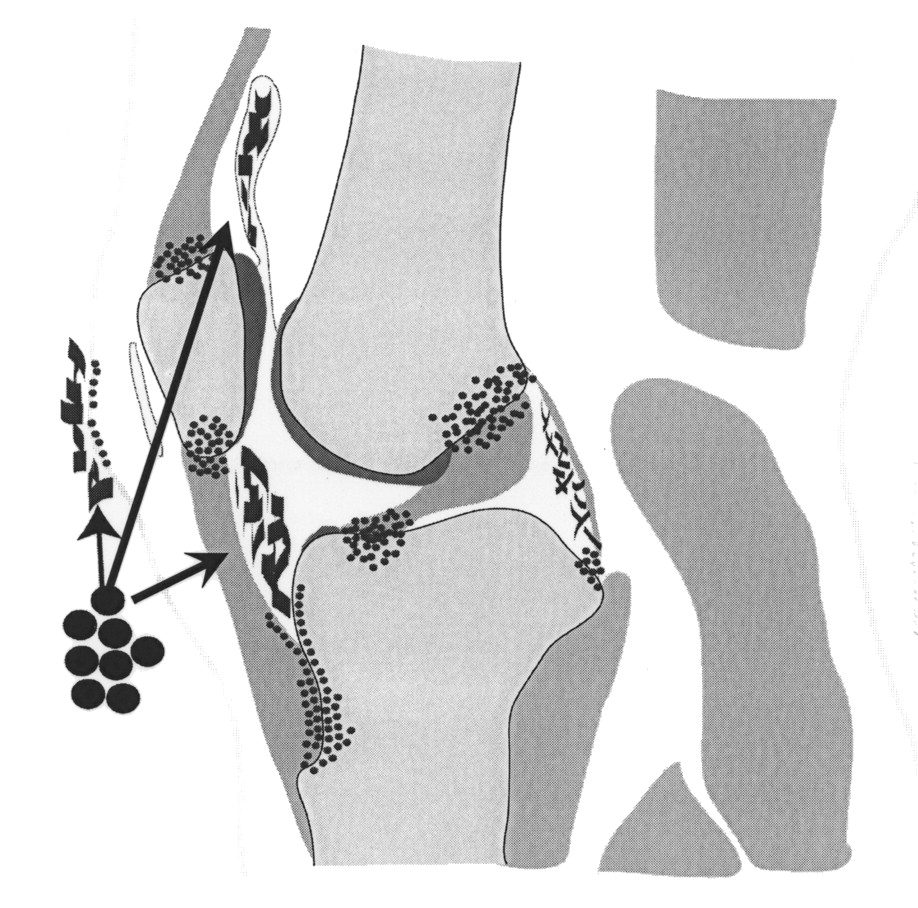
The common biomechanical basis between skin and joints: a knee joint. The historical perception in PsA and psoriasis was that autoreactive lymphocytes (large black circles) targeted a common unidentified autoantigen in the skin and synovial membrane (wavy rectangles). However, it is now evident from imaging studies that enthesitis is a key pathological lesion in PsA and that entheses form functionally integrated units with adjacent synovium in structures termed synovio-entheseal complexes1. These structures appear to be associated with microdamage at insertion sites in normal joints (small black dots). Even in normal joints this is associated with microscopic synovitis in adjacent soft tissues2. Therefore, the common denominator in PsA may be related to aberrant responses to stress at the enthesis, which offers a new biomechanical model for joint disease in PsA3. From McGonagle, et al. Ann Rheum Dis 2008;67:1–43, with permission.
Ultra-short echo time: Richard Hodgson
Dr. Hodgson presented new information regarding the new technique of ultrashort echo time (UTE) magnetic resonance imaging (MRI). In standard MRI sequences, tendons and fibrocartilage cannot be visualized as their echo time is too short to be identified. Therefore, on standard MRI images, the tendons and the fibrocartilage appear dark. Inflammation at these sites only becomes visible when it is severe and if the structures thicken significantly, both relatively late signs. Using UTE, MRI allows imaging of these structures in greater detail and identifies inflammation at an earlier stage. Given the involvement of the enthesis and the synovio-entheseal complex in PsA (discussed by McGonagle) and the level of subclinical disease seen previously on ultrasound, this will be an interesting technique for evaluation of PsA. As the image from a UTE MRI sequence shows only the signal received at a very short echo time, the contrast of the image can be poor unless it is further enhanced by techniques such as subtraction, T1 weighting, fat suppression, magnetization transfer, and intravenous contrast (Figure 2).

Conventional image (A) and T1-weighted ultra-short echo time (UTE) image (B) of the Achilles tendon at the enthesis. With conventional T1-weighted MRI, the Achilles tendon (T) appears uniformly dark. With UTE imaging, the tendon is of high signal intensity, and internal fibrillar structure is evident. Images courtesy of Richard Hodgson and Matthew Robson.
Dr. Kavanaugh gave a brief presentation reporting the use of UTE imaging in patients with PsA, emphasizing that the work was still at a developmental stage. He presented data reported to the American College of Rheumatology in 2007 in which UTE images of the Achilles tendon were related to clinical signs of enthesitis at this site in patients with PsA. Although these were preliminary results, imaging scores using UTE were found to be higher in those cases with clinical enthesitis4.
Imaging musculoskeletal tissues in psoriasis: Paolo Gisondi
Dr. Gisondi presented results of a study designed to look for imaging abnormalities at entheses in asymptomatic people with psoriasis5. Thirty people with chronic psoriasis were examined by a rheumatologist and found not to have PsA or symptoms at the entheses. These people were examined with ultrasound at several lower-limb enthesis sites and evaluated using the Glasgow Ultrasound Enthesitis Scoring System (GUESS)6. A series of people with other dermatoses were used as controls. The results are shown in Figure 3. The increased frequency of abnormalities in the entheses of people with chronic psoriasis is evident, leading to speculation that musculoskeletal abnormalities in uncomplicated psoriasis may be much more widespread than was previously thought. Dr. Gisondi introduced the concept of “psoriatic disease,” and speculated on the significance of the entheseal abnormalities — do they predict those who will develop PsA? Dr. Gisondi reported that indeed 2 of the original 30 people studied had developed PsA after 2 years of followup.
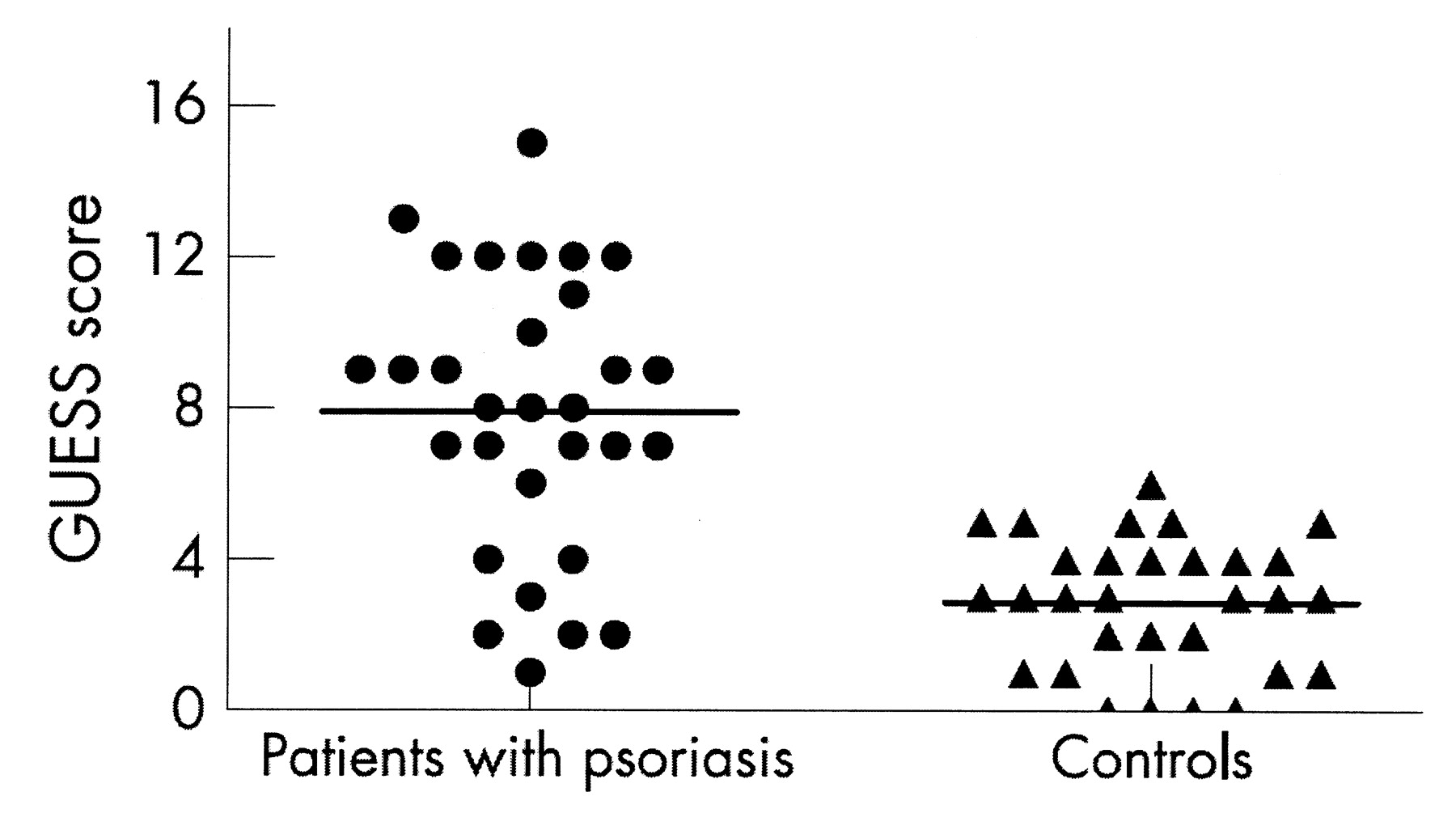
Glasgow Ultrasound Enthesitis Scoring System (GUESS) scores in patients with psoriasis and those with other dermatoses. From Gisondi, et al. Ann Rheum Dis 2008;67:26–30, with permission5.
Imaging Discussion Summary: Breakout Groups
Discussion Group Leaders: Oliver FitzGerald, Dafna Gladman, Philip Mease, Abrar Qureshi, Jerry Krueger, Chris Ritchlin, Arthur Kavanaugh
Following these brief presentations, 7 breakout groups were convened to discuss the presentations and to consider the following, with summary of the discussions further below:
-
What further studies do we need to elaborate the pathophysiology of PsA?
-
What is the role of new technologies such as UTE?
-
What specific collaborative research initiatives might be generated within GRAPPA?
Two key study populations were identified by most of the groups: a psoriasis group at risk of developing PsA and an early PsA group. For some of the newer imaging techniques in particular, it was felt that evaluating normal controls would also be important. This control group would have to be well characterized clinically to correlate with imaging findings.
There was some debate about attempting to enrich the first group (psoriasis with no clinical evidence of PsA) to increase the numbers of patients who develop arthritis. Suggestions included using patients with a positive family history or using patients with a psoriasis history of less than 10 years’ disease duration who are more likely to develop PsA. Dr. Mona Stahle (Sweden) made the point that any attempt to enrich the population would introduce bias to the study.
It was felt that both arthritis and enthesitis should be studied further to attempt to improve our understanding of the pathophysiology of PsA. The data presented on the prevalence of enthesitis in asymptomatic psoriasis patients was exciting. However, the link between subclinical enthesitis detected in this way and the subsequent development of arthritis remains unknown. Further, in established PsA, there is a poor relationship between ultrasonographic enthesitis and clinical enthesitis6. Research is needed to determine which specific enthesitis sites are more distinct in PsA, and enthesitis should be investigated at these sites both clinically and with imaging. Perhaps certain enthesitis sites can be identified that increase the risk of the development of PsA in patients with psoriasis. Distinguishing fibromyalgia tender points (FMTP) from enthesitis is important, and we must rule out inclusion of FMTP in enthesis counts.
The effect of treatment was also discussed in terms of pathophysiology. Clearly, disease-modifying drugs work differently, which may be reflected in the diverse presentations of PsA. For example, anti-tumor necrosis factor (TNF) drugs probably work better than methotrexate (MTX) on enthesitis, and drugs targeting the p40 subunit of interleukin 23 work better on the skin than the joints. Is this a site-specific effect, or is there genetic or pathoanatomic variation within the disease that affects response to treatment? Imaging may teach us more about these differences.
The possibility of linking imaging studies to tissue sampling and analysis was also discussed. It may be possible to use animal models of inflammation, with ultrasound and MRI to target tissue sampling. Specific models such as the Jun mouse model would have potential for this. It is also important to collect human tissue where possible in certain sites, particularly if this can be done as an adjunct to a clinical procedure, or for any arthroscopic procedure or joint replacement. It was felt that further investigating the Koebner phenomenon would be of interest and could combine imaging and tissue studies. This may require collaboration in a team with suitably experienced bioengineers and cell biologists/immunologists. Cadaveric tissue might also be helpful and contribute to our understanding. National patient organizations may help acquire these tissues.
What is the role of new technologies such as UTE?
The UTE MRI technique is still being developed but promises to be an exciting method for demonstrating further detail in soft-tissue structures such as tendon and enthesis. Two centers currently studying this technique are linked to the GRAPPA group (University of Leeds and University of California at San Diego). It was agreed that collaboration between these groups would be of interest and was likely to optimize protocols and images. The clinical relevance of the technique cannot be evaluated at such an early time, but further work should clarify this. Obviously, future studies should include a direct comparison of UTE and ultrasound to evaluate the ideal use of both techniques in this field.
What specific collaborative research initiatives might be generated within GRAPPA?
All the groups felt that there was potential for GRAPPA to help coordinate a multicenter imaging study. Many groups commented that this should be linked into other proposed multicenter studies, including the ambition to collect prospective “cohort” data across GRAPPA in a standardized way and in the proposed collaborative biomarkers study. It was acknowledged that not all sites would have the ability or expertise to perform all modes of imaging, but that sites interested in ultrasound and MRI could become involved in a substudy of the patient registry. Therefore, the majority of the support was for a longitudinal study with efforts to collect clinical data, imaging, and tissue. Registries should collect patients with different clinical presentations so that certain basic information is mandatory, but additional information and imaging could be optional for centers with a particular interest.
It was agreed that careful planning is needed to ensure that collection of clinical data, images, and the processing/storage of any tissue samples is done uniformly across different sites. To ensure uniform data collection, it was also recognized that the group should agree on the core clinical data to be collected, including demographic data, data according to CASPAR criteria7, and assessment of skin, nails, dactylitis, enthesitis, spine and joints. Not everyone will be expected to collect all the imaging, and centers that can collect tissue should do so. Small collaborative studies should be done between groups that have new technologies such as UTE imaging, to provide basic information about the utility of these techniques before they are adopted in multiple centers.
It was also recognized that any collaboration in imaging would have to be carefully controlled by protocol and standardization of technique to ensure that images and subsequent analysis could be compared across centers. This is a particular problem with ultrasound, where the skill and experience of the ultrasonographer is key. Ultrasound was felt to be more practical for investigating entheses at multiple sites without UTE expertise, but because of operator variability there must be adequate training and standardization to assure similarity in approach. Ideally, techniques should specify minimal experience and skill and be highly protocol-driven. Digitization will be important in the sharing of images.
There was a discussion of the development of standard operating procedures for the different imaging techniques, which could be included within the OMERACT initiative. An OMERACT group for ultrasound has submitted an application for a session at OMERACT 10. Perhaps collaboration could be sought between the 2 groups to try and develop this common interest. A new development with 3-D ultrasound imaging also may be helpful in terms of reproducibility, although further study of this is required.
Dr. John Moll (Sheffield, UK) commented that some years ago, when plain radiographs were considered sophisticated, Kellgren and Lawrence developed an atlas of standard images that came to be used by all researchers. Similar initiatives have been developed in rheumatoid arthritis for newer imaging techniques with the development of the RAMRIS atlas for MRI as an outcome measure8. Dr. Moll wondered whether these new imaging techniques and studies in PsA may eventually lead to an atlas of PsA imaging.
It was hoped that GRAPPA will allow optimal utilization of resources that are available to individual sites and countries to pool data. It also was hoped that each institution may be able to find some support through local funding channels. An overriding theme was the reality of fundraising, as well as imaging, when doing a large study in different countries. This work will more likely take place locally or nationally than internationally. A centralized database also will be needed. At present, 3 key databases are available in this field. Philip Mease discussed the US-based CORRONA (COnsortium of Rheumatology Researchers Of North America) database, which is in the process of adding more variables for PsA. Currently, the CORRONA database contains data on more than 2500 PsA patients. Dafna Gladman (Toronto, Canada) introduced the International Psoriatic Arthritis (IPART) database, which is collecting data on patients with psoriasis and PsA in multiple sites in Canada and the USA. Finally, a Web-based European database is available to members of the Psoriatic Arthritis Genetics in Europe (PAGE) consortium.
In this issue








{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- The synovio-entheseal complex: Dennis McGonagle
- Ultra-short echo time: Richard Hodgson
- Imaging musculoskeletal tissues in psoriasis: Paolo Gisondi
- Imaging Discussion Summary: Breakout Groups
- What is the role of new technologies such as UTE?
- What specific collaborative research initiatives might be generated within GRAPPA?
- REFERENCES
- Figures & Data
- Info & Metrics
- References
- eLetters