

Abstract
Objective. To evaluate the utility of magnetic resonance imaging (MRI) in systemic sclerosis (SSc)-associated arthropathy.
Methods. MRI of the hand was performed in patients presenting with joint pain/swelling in order (1) to determine the frequency of inflammation on MRI, and (2) to compare MRI with radiography.
Results. Of 17 patients with SSc, 10 (59%) had inflammatory MRI findings with synovitis (n = 8), erosions (n = 7), joint effusion (n = 7), or tenosynovitis (n = 8). Bone edema was present in 9 patients. Of 7 patients with MRI erosions, only 2 had radiographic erosions.
Conclusion. Our study illustrates the usefulness of MRI in the accurate diagnosis and characterization of SSc-associated arthropathy.
Joint involvement in systemic sclerosis (SSc) is disabling1 and can be a result of arthritis, overlying skin tightness, flexion contractures, or fibromyalgia, which can be clinically challenging to determine accurately. Joint pain occurs in 24% to 97% of patients with SSc2 and in late disease may be due to synovial fibrosis without underlying synovitis3.
Radiographic abnormalities in SSc are well described2,4,5. The utility of magnetic resonance imaging (MRI) in evaluating SSc-associated arthropathy has not previously been described. MRI is able to reveal the extent of synovitis, tenosynovitis, and effusions contributing to the joint symptoms and to differentiate these from skin or soft tissue involvement, especially in early disease. This has significant therapeutic implications. With active synovitis, the early use of disease modifying antirheumatic drug or tumor necrosis factor-α inhibitors6,7 may prevent progressive joint damage and loss of function.
The aim of our study was (1) to determine the prevalence of inflammation on MRI, and (2) to compare MRI with radiography in patients with SSc presenting with joint pain/swelling of the hands.
MATERIALS AND METHODS
Patients
Patients > 18 years of age with SSc fulfilling American College of Rheumatology (ACR) classification criteria8 were included if they (1) had a history of joint pain/swelling of the hand/wrist and (2) agreed to have an MRI of the hand/wrist. The study was approved by the institutional research ethics board.
Medical records were reviewed for (1) demographic data (sex, age, disease duration from the time of SSc diagnosis, subtype according to LeRoy, et al9, onset of first joint symptoms); (2) rheumatoid factor (RF) and anti-cyclic citrullinated peptide (anti-CCP) status; and (3) examination findings on visit prior to MRI [tender and swollen joint counts (TJC/SJC), tenosynovitis, and flexion contractures in the hands and wrists only].
Radiology
Standard anterior-posterior radiographs of the hands and wrists were obtained. MRI of the hand/wrist was performed on a 1.0 or 1.5 Tesla MRI device with dedicated surface coils. Nonenhanced axial and coronal T1-weighted spin-echo imaging, plus either short-tau inversion recovery (STIR) or fast spin-echo T2-weighted fat suppressed sequences were performed in all patients. MRI and radiographs were reviewed by an independent radiologist blinded to the patients’ clinical detail. Results were recorded according to 4 predefined categories as appropriate for the mode of imaging as (1) articular [presence of joint space narrowing (JSN), erosion, synovitis, and effusion]; (2) soft tissue (calcification, tenosynovitis); (3) bone (osteopenia, bone resorption, bone edema); or (4) degenerative (subchondral sclerosis, bone cyst, osteophyte, or JSN plus one of the above).
Radiographic erosion was defined as interruption of the cortical surface. Inflammation on MRI was defined as any one of synovitis (synovial thickening on T1-weighted images and high signal intensity on STIR/T2-weighted images); erosion (a sharply marginated bone lesion visible in 2 planes with a cortical break in at least 1 plane); joint effusion (low signal intensity on T1-weighted images and high signal intensity on STIR/T2-weighted images with correct localization); or tenosynovitis (high signal intensity on STIR/T2-weighted images with correct localization). Bone edema was defined as a lesion in trabecular bone with ill-defined margins of high signal intensity on T2-weighted images.
RESULTS
Seventeen patients (10 diffuse, 7 limited SSc) were recruited; 14 had a history of symmetrical joint symptoms.
Inflammatory findings on MRI
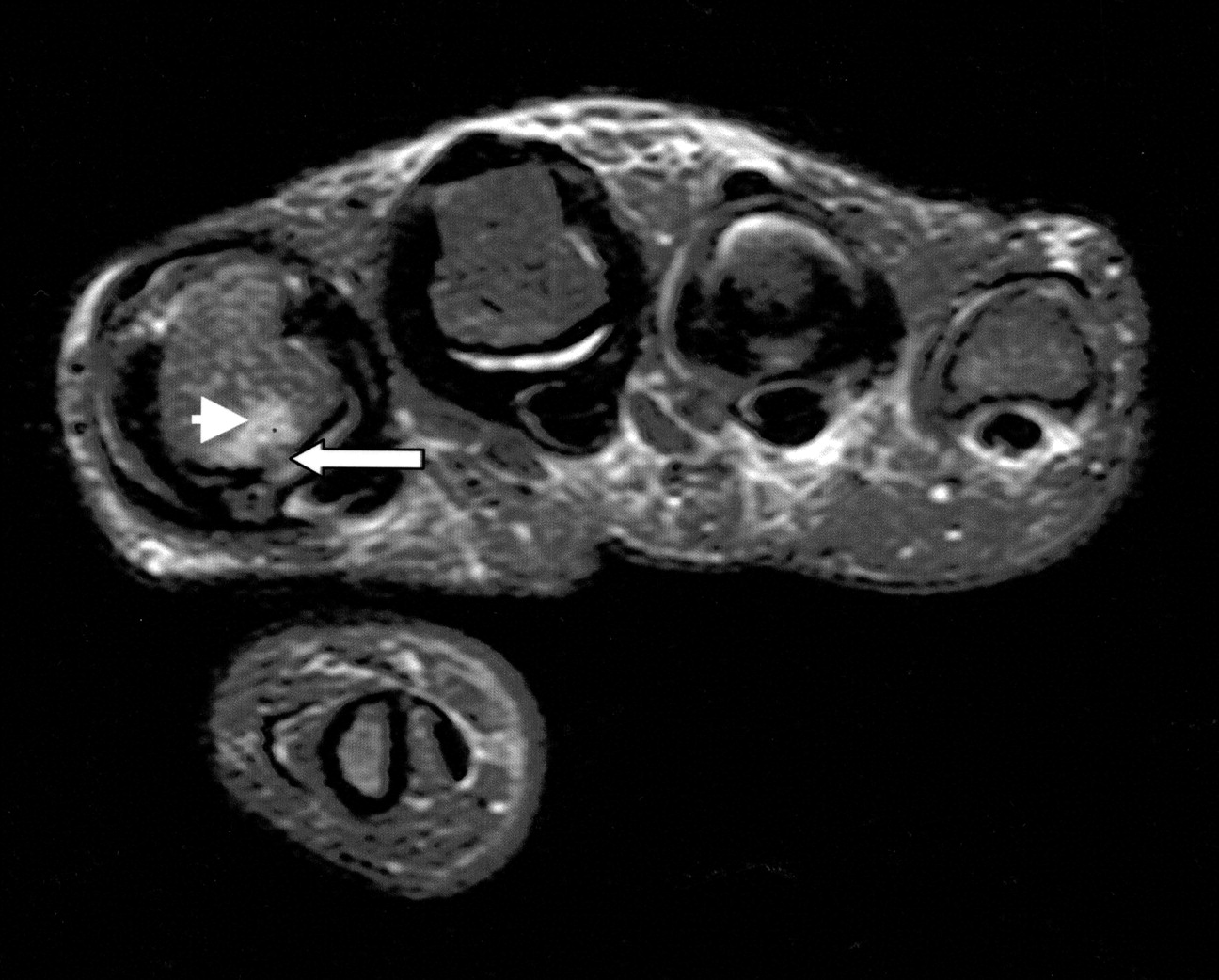
Ten (59%) patients had inflammatory findings on MRI. Eight (47%) had synovitis, 7 (41%) had erosions, 7 (41%) had joint effusion, and 8 (47%) had tenosynovitis. Bone edema was present in 9 (53%) patients. Inflammatory changes were symmetrical in 5 patients who had MRI of both hands (Table 1). Patients 4 and 11 had contrast-enhanced MRI that confirmed findings on STIR imaging. Figures 1A and 1B illustrate MRI findings of synovitis, flexor tenosynovitis, and erosions.
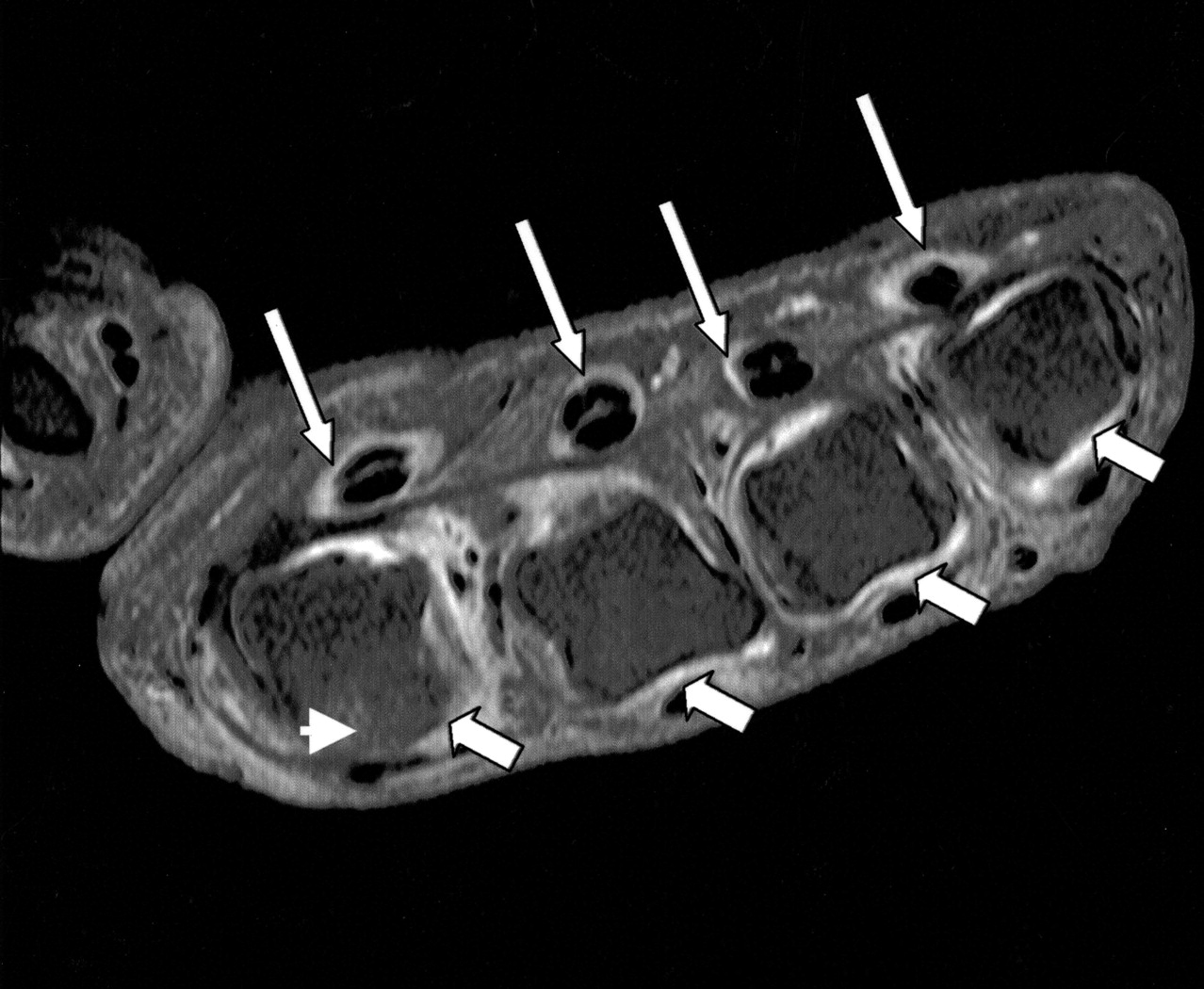

A. Enhanced MRI image of metacarpophalangeal (MCP) joints (Patient 4). Arrowhead: bone edema; long arrow: flexor tenosynovitis; short arrow: synovitis. B. MRI/STIR image of MCP joints (Patient 2; hand radiographs showed no erosions). Arrowhead: bone edema; long arrow: bone erosion.
Inflammatory findings on MRI scans in 10 patients.
Synovitis (n = 8), joint effusion (n = 7), and tenosynovitis involving flexor and extensor compartments (n = 8) were more frequently detected on MRI than was clinically evident (joint swelling n = 5, joint tenderness n = 7, and tenosynovitis n = 2).
Characteristics of patients with (Group 1) and those without inflammation (Group 2) on MRI
Baseline demographics of the patients were similar except that in Group 2 there were more patients with diffuse disease and shorter disease duration (Table 2). Group 1 had lower median TJC/SJC than Group 2, with similar frequency of finger flexion contractures. RF and anti-CCP were present in 40% (4/10) and 11% (1/9) of patients in Group 1 and 43% (3/7) and 20% (1/5) of patients in Group 2.
Characteristics of patients with (Group 1) and without (Group 2) inflammation on MRI scan.
Comparison of MRI and radiography
Sixteen patients had both MRI and radiographs available for comparison (n = 25 hands). These were obtained at about the same time, except in Patients 6, 10, and 16, in whom radiographs were performed about 1 year prior to the MRI, and Patients 4, 7, and 8, about 1 year after the MRI.
In Group 1, 13 sets of MRI and radiographs were available for comparison for the presence of erosions (n = 7 patients). MRI erosions were detected concomitantly on 3 radiographs (n = 2 patients), but were not detected on 6 radiographs (n = 4 patients). In 3 patients (n = 4 hands), erosions were not detected by either method. Disease duration at the time of MRI in the 2 patients with radiographic and MRI erosions were 0.2 years and 13.7 years.
Radiographs were more sensitive in detecting JSN than MRI. Of 25 hands imaged, there was agreement between radiographs and MRI for the presence of JSN in 12. Of the 13 that were discordant, JSN was detected on 11 radiographs but not on MRI. The efficacy of MRI and radiography in detecting degenerative change appeared to be similar.
DISCUSSION
MRI was more sensitive than clinical examination in detecting synovitis, joint effusion, and tenosynovitis. Patients with MRI inflammation had fewer tender and swollen joints than those without inflammation, illustrating the difficulty in accurate clinical assessment due to overlying tight skin, finger contractures, or fibromyalgia. In one study1, 49% of patients with SSc had > 11 tender points.
MRI showed the presence of erosive arthritis in 41% of patients with SSc and was more sensitive than radiography. Whether these changes are due to an overlap SSc/rheumatoid arthritis (RA) syndrome or SSc per se is unclear. In a study of hand vascular involvement assessed by MR angiography in 38 SSc patients10, 16% had erosions, 50% had synovitis, and 11% had tenosynovitis.
SSc-associated radiographic erosions, with reported prevalence of 21%–40%2,4, has traditionally been thought to be less aggressive than RA because of the notable absence of pannus3. The prevalence of RF in SSc is reported to be 20%–60% but, as in our study, it has not been associated with erosive arthritis2,5. Similarly, anti-CCP did not appear to be associated with arthritis, although one study suggested that it can help define a subgroup of patients with SSc/RA overlap due to its association with clinically apparent arthritis and radiographic erosions11.
The presence of selection bias needs to be considered when interpreting the data, as MRI scans were ordered in most instances because of diagnostic uncertainty regarding the presence of arthritis, and may represent patients with more severe disease. Due to small numbers of patients and limitations associated with observational studies the data must be interpreted with caution. Although contrast-enhanced T1-weighted images would have been the optimal method in delineating synovitis according to RA OMERACT (Outcome Measures in Rheumatology) guidelines12, this was not routinely done due to concerns regarding nephrogenic systemic fibrosis13.
Our study illustrates the usefulness of MRI in the accurate diagnosis of SSc-associated arthropathy. This pilot study provides a basis for prospective studies to investigate the implications of MRI joint abnormalities in SSc in terms of early aggressive treatment and improved outcomes.
Footnotes
- Accepted for publication December 24, 2008.








{kind=link}
{kind=link}