

Abstract
Objective. To systematically review the efficacy and safety of mycophenolic acid and mycophenolate mofetil (MMF) compared to cyclophosphamide (CYC) for the induction treatment of lupus nephritis (LN).
Methods. Medline, Embase, the Cochrane Center Register of Controlled Trials, and abstracts presented in major international conferences were searched for randomized controlled trials. The primary outcome was renal remission (complete, partial, and overall) and secondary outcomes were adverse events during study period and longterm followup data. Data were compared between groups and relative risk (RR) and 95% CI were calculated.
Results. Four trials of a total of 618 patients were included. MMF was not superior to CYC for renal remission (partial RR 0.94, 95% CI 0.80 to 1.12; complete RR 0.67, 95% CI 0.35 to 1.28, and overall RR 0.89, 95% CI 0.71 to 1.10). There was a significant reduction in alopecia (RR 5.77, 95% CI 1.56 to 21.38) and amenorrhea (RR 6.64, 95% CI 2.00 to 22.07) with the use of MMF compared to CYC. These results should be interpreted with caution given the width of the CI. There was no significant difference for infections, leukopenia, gastrointestinal symptoms, herpes zoster, endstage renal disease, and death among groups during study period and longterm followup data.
Conclusion. We could not show that MMF is superior to CYC for the induction treatment of LN. Patients treated with MMF showed reduced risk of certain side effects. MMF can be used as an alternative to CYC for the induction treatment of LN.
Systemic lupus erythematosus (SLE) is a multisystem autoimmune disease that can affect the skin, joints, kidneys, lungs, nervous system, serous membranes, and/or other organs of the body. Sixty-five percent of patients with SLE have disease onset between the ages of 16 and 55 years1. Most renal abnormalities emerge within the first 6 to 36 months, although some patients may develop lupus nephritis later in their course of disease2. Lupus nephritis (LN) occurs in up to 60% of adults with SLE and predicts poor survival1. Chronic renal insufficiency plays a role in late mortality3.
The treatment of LN is in 2 phases: induction and maintenance therapy. The goal of induction therapy is to produce a remission in lupus activity and improvement of renal function. Intravenous cyclophosphamide (CYC) with or without steroid is used mainly to induce remission in patients with proliferative LN4,5,6,7. Metaanalysis indicated that immunosuppressive drugs (azathioprine or CYC) and steroids together are more effective than steroids alone in treating acute LN8,9. However, studies have reported that in patients with diffuse proliferative glomerulonephritis, renal flares are common despite initial responses to CYC10. Another metaanalysis reported that treatment with CYC had no survival benefit but was associated with better renal outcome; however, there was a significant increase in the risk for adverse effects including ovarian failure9.
Mycophenolate mofetil (MMF) is a potent, selective, non-competitive, and reversible inhibitor of inosine-5′-monophosphate dehydrogenase. It inhibits T and B lymphocyte proliferation and immunoglobulin production11. Mycophenolate is available in 2 forms: mycophenolic acid (MPA) and MMF. MMF is a prodrug of MPA that was developed to improve the bioavailability of MPA11. After oral administration, MMF is completely metabolized to MPA. MMF has been used since the early 1990s for the prevention of acute allograft rejection12. More recently, MMF has gained popularity as a potentially glucocorticoid-sparing agent for the treatment of patients with a variety of rheumatic illnesses including lupus11,13. It has a relatively better side effects profile14,15,16,17,18. Some studies reported that a combination of MMF and prednisone constitutes an effective continuous induction-maintenance treatment for LN3,16,19,20,21,22. A metaanalysis reviewing the literature until 2008 showed that MMF offers similar efficacy in renal remission and survival as CYC and appears to be safer in the treatment of proliferative LN23. However, the results of randomized controlled trials (RCT) and observational studies of MMF in the treatment of LN do not agree completely14,17,24. Meta-analyses have suggested that more patients responded to MMF than to intravenous (IV) CYC and recent studies have suggested that MMF may offer advantages over IV CYC for the treatment of LN14,24,25. This encouraging benefit, however, was not reproduced by Appel, et al17, where MMF was not superior to IV CYC as induction treatment for LN15,16,17,18. Given this uncertainty, we conducted a systematic review and metaanalysis to determine the efficacy and safety of MMF in inducing remission in patients with biopsy-proven active LN compared to CYC.
MATERIALS AND METHODS
Literature search
An experienced librarian searched Ovid Medline (1950 to November 21, 2009), Embase (1980 to November 21, 2009), and the Cochrane Center Register of Controlled Trials (1993 to November 21, 2009). Abstracts presented at major international conferences (Annual European Congress of Rheumatology, International Congress on SLE, and the American College of Rheumatology meeting) over the past 10 years were manually searched. We reviewed the bibliography of the retrieved trials and review articles for all relevant studies. We ran the search without language restriction; however, only English abstracts were reviewed. The search terms were modified to reflect database vocabularies (Appendix 1).
Study selection and assessment
We included randomized and quasirandomized trials (allocation based on possible identifiers such as date of birth, alternative medical records) that explored the efficacy of MMF or MPA over 6 months in biopsy-proven active LN compared to CYC as induction therapy and reported any outcomes of interest. We included information available from publications and contacted primary authors for additional data if they were missing. We did not restrict the selection of trials on the mode of the administration of CYC (parenterally or orally). We excluded studies in which MMF was compared with immunosuppressive drugs other than CYC, studies without clearly defined outcomes, and studies published only as abstracts. If a trial was an extension of a prior published trial, we included the most recent publication. Studies for which quality could not be determined were also excluded. Observational studies, case series, letters, commentaries, reviews, and editorials were excluded if they did not contain original data. One author scanned the titles and abstracts for initial selection. Selected articles were retrieved in full and 2 reviewers assessed them for eligibility. Discrepancies were resolved by consensus and involvement of other authors.
Outcome measures
The primary outcome of interest was achievement of complete, partial, and overall remission at 6 months after induction therapy. The definitions of complete and partial renal remission in our meta-analysis were based on the individual studies’ remission criteria, which were essentially similar to one another (Tables 1 and 2)14,16,17,18. Secondary outcomes were development of endstage renal disease (ESRD), mortality, and other adverse events at 6 months after initiation of treatment including infections, anemia, leukopenia, gastrointestinal symptoms, herpes zoster, amenorrhea, and alopecia (Table 3).
Definition of primary outcomes used in studies; partial and complete renal remission.
RCT included in the metaanalysis.
Results from included studies (primary and secondary outcomes).
Methodologic quality
For the assessment of bias risk, 2 reviewers independently assessed the methodologic quality of the studies using a predefined checklist suggested for the Cochrane Database of Systematic Reviews26. This checklist assesses risk of bias in the categories of sequence generation, allocation concealment, blinding of assessors and patients, incomplete outcome data addressed, avoidance of selective reporting, and avoidance of other bias26. The classification in each category was yes, no, or unclear. We performed an overall assessment of bias risk based on responses from these criteria, and resolved discrepancies by involvement of other authors.
Sensitivity and subgroups analysis
We planned sensitivity analyses that would exclude studies with a high likelihood of bias in 3 or more domains. The following subgroup analyses were planned: (1) the 3 studies where CYC was given parenterally were chosen in order to be compared to MMF; (2) the 2 studies where a dose of 3 g/day MMF was administered were selected in order to be compared to CYC; (3) studies based on the ethnicity of patients; (4) studies with a duration of 6 months; and (5) studies in which the rate of death and ESRD that occurred over longterm followup or ever reported (during study period and followup period).
Clinical heterogeneity was assessed for characteristics of the study populations (i.e., the ethnicity or race, mean age at enrollment, duration of SLE, renal biopsy class, range of serum creatinine and glomerular filtration rate, urine protein, and urine analysis), dose of MMF and CYC, and methodologic quality of the studies. Statistical heterogeneity among studies was assessed by using the Cochrane Q test and by calculating I2 values27.
We contacted the corresponding authors to obtain information about secondary outcomes that was missing from their articles.
Data extraction and synthesis
Two reviewers extracted data from each eligible study using custom-made data collection forms. The original data were not modified, and calculations were performed from available data for the metaanalysis. For binary outcome variables (complete, partial, and overall rate of renal remission and rate of adverse events such as infections, leukopenia, anemia, gastrointestinal symptoms, herpes zoster, amenorrhea, alopecia, ESRD, and death) we calculated relative risk (RR), along with 95% CI. For ESRD and death we included data available during the study period, longterm followup, and ever reported. We expected clinical and statistical heterogeneity among the studies. Review Manager 5 software was used in our metaanalysis. The effect sizes were based on the use of the Mantel-Haenszel test. We used the random-effect model for metaanalyses because it accounts for random variability both within and among studies. We planned to evaluate publication bias by visual inspection of funnel plot if there were a sufficient number of studies identified.
RESULTS
Literature search
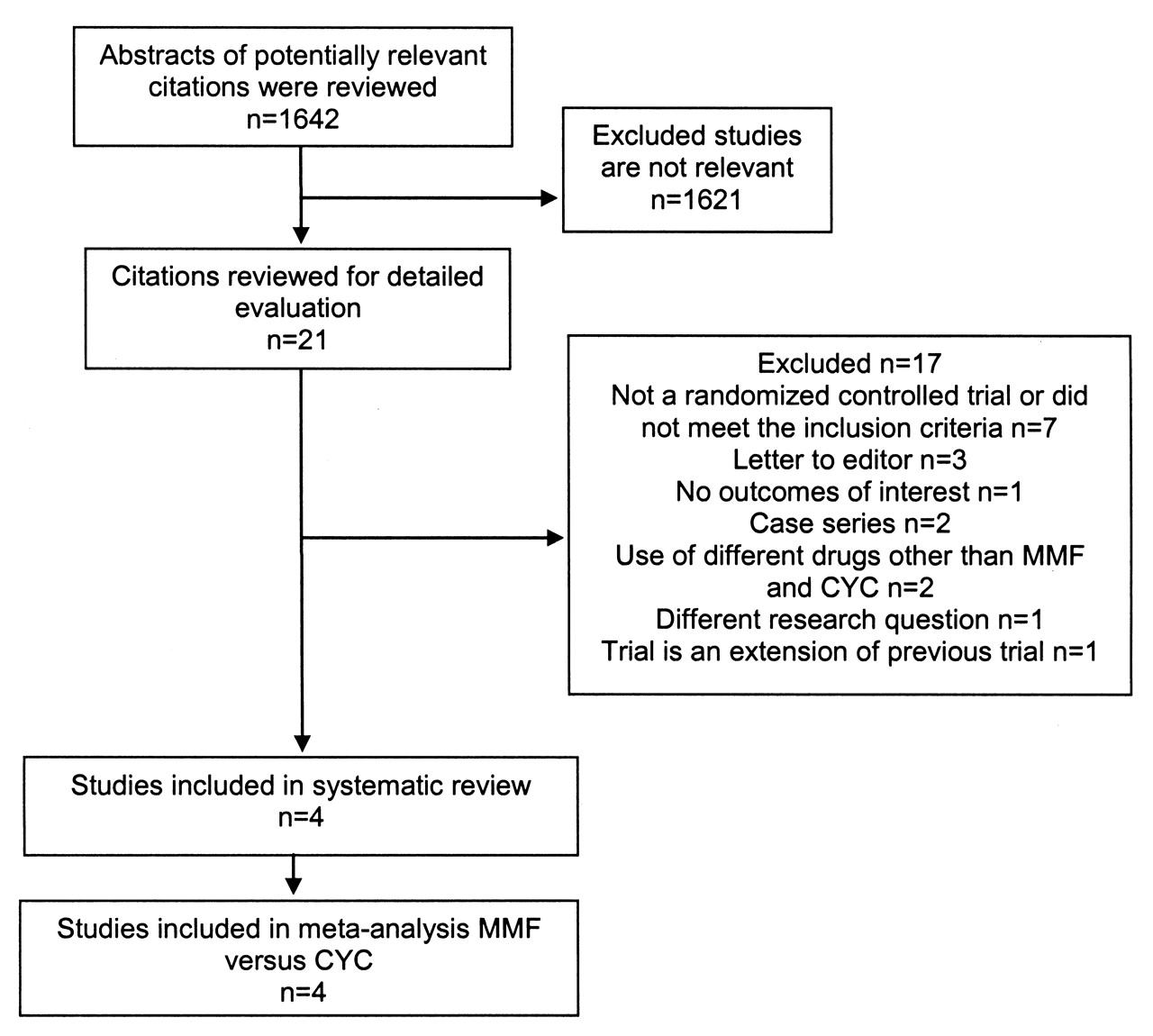
The results of our search strategy and selection of included and excluded articles are given in Figure 1. Four eligible RCT were identified and included in this review14,16,17,18. We excluded 17 reports for the following reasons: uncontrolled trials, a review of an RCT, the trial did not compare MMF and CYC, the trial involved LN maintenance, the trial was an extension of a published trial, or the report was an editorial (Figure 1). We identified that 1 trial was included in another trial with a bigger sample15.

Selection of studies for metaanalysis of the effect of mycophenolate mofetil (MMF) and cyclophosphamide (CYC) on induction therapy.
Study participants and interventions
The characteristics of the included studies are reported in Table 3. In the study by Chan, et al, CYC was administered orally instead of parenterally16. The study by Appel, et al enrolled patients with endstage kidney disease17. Thirty-two patients with an estimated glomerular filtration rate (eGFR) < 30 ml/min per 1.73 m2 were enrolled (20 patients treated with MMF and 12 patients treated with CYC)17. In the remaining 3 studies by Chan, et al, Ong, et al, and Ginzler, et al, patients with serum creatinine > 300, 200, and 252.2 μmol/l, respectively, were excluded14,16,18. In all the studies, patients included in both arms received prednisone at 0.7–1 mg/kg/day, which was tapered progressively14,16,17,18.
Methodologic quality
The results of our assessment of the risk of bias among included studies and compliance rates showed a low to moderate risk of bias. One study did not provide enough details about allocation concealment (Appendix 2)16. None of the studies masked assessors and patients; nevertheless, we believe that this would not affect the determination of the primary outcome, which was based on objective laboratory findings. This could affect ascertainment of secondary outcomes such as adverse events. However, the use of checklists for study quality evaluation does not identify all the aspects of methodological approach in each trial and these findings should be interpreted with caution.
Outcomes
Details of the primary and secondary outcomes reported in the individual studies are provided in Tables 2 and 3. All 4 studies reported on the primary outcome of renal remission (complete, partial, and overall)14,16,17,18. All studies compared MMF (n = 308) treatment with CYC (n = 310). In 3 studies, CYC (n = 279) was administered intravenously, but in 1 study it was given orally (n = 31)16. All 4 studies included extensive followup data for ESRD and death (Table 3). MMF was neither superior to nor worse than CYC for overall renal remission (RR 0.89, 95% CI 0.71 to 1.10), partial renal remission (RR 0.94, 95% CI 0.80 to 1.12), or complete renal remission (RR 0.67, 95% CI 0.35 to 1.28; Figure 2).

Primary outcomes (partial remission, complete remission, and overall remission). Random-effect metaanalysis of the rate of partial, complete, and overall renal remission among patients given mycophenolate mofetil (MMF) versus cyclophosphamide (CYC). Values < 1.0 favor MMF. M-H: Mantel-Haenszel test.
For the secondary outcomes, the risks of alopecia (RR 5.77, 95% CI 1.56 to 21.38) and amenorrhea (RR 6.64, 95% CI 2.00 to 22.07) were significantly higher among patients given CYC compared to those given MMF. However, the estimates of alopecia and amenorrhea appear unstable given the width of the CI and this should be interpreted with caution in clinical practice.
The rates of infections, gastrointestinal symptoms, herpes zoster, leukopenia, and anemia were not significantly different between groups (Figure 3). There was no significant difference between MMF and CYC for ESRD during the study period (RR 1.29, 95% CI 0.22 to 7.63)17,18. Fifteen patients developed ESRD in the CYC group and 8 in the MMF group. There was no significant difference between MMF and CYC for death during the study period (RR 1.07, 95% CI 0.14 to 8.03). Seven patients died in the CYC group and 9 in the MMF group14,17,18 (Table 4).

Secondary outcomes. MMF: mycophenolate mofetil; CYC: cyclophosphamide; M-H: Mantel-Haenszel test; ESRD: endstage renal disease.
Results of secondary outcomes.
Heterogeneity and publication bias
There was high statistical heterogeneity for outcome of renal remission (I2 = 68%–75% for complete and overall remission, respectively) and for adverse events (I2 = 81%–87% for leukopenia and infections, respectively). There was no statistical heterogeneity for outcome of renal remission when we excluded Ginzler, et al (I2 = 0% for partial, complete, and overall renal remission)14. Since only 4 studies were included in our metaanalysis, a funnel plot was not developed. Publication bias is unlikely because of the open-label design of the studied trials. Moreover, the assessment of renal outcome (partial and complete remission) was based on laboratory findings and not affected by the subjective reports of the patients or assessors.
Subgroup and sensitivity analyses
Subgroup analysis including only studies that administered CYC intravenously (n = 279) versus MMF (n = 275) revealed no difference in the rate of renal remission (partial, RR 1.06, 95% CI 0.89 to 1.26, p = 0.51; complete, RR 1.91, 95% CI 0.83 to 4.44, p = 0.13; overall, RR 1.23, 95% CI 0.90 to 1.67, p = 0.19)14,17,18.
There was no statistical difference in the rate of renal remission (partial, RR 1.07, 95% CI 0.90 to 1.28, p = 0.42; complete, RR 1.91, 95% CI 0.54 to 6.80, p = 0.32; overall, RR 1.30, 95% CI 0.81 to 2.08, p = 0.28) between patients who received a maximum target dose of 3 g/day MMF compared to CYC14,17.
There was no statistically significant difference in partial renal remission among Asian patients who received MMF compared to CYC (RR 0.85, 95% CI 0.65 to 1.11, p = 0.23)16,17,18.
Three studies compared MMF (n = 275) treatment with CYC (n = 279) over a period of 6 months. There was no significant difference between MMF and CYC for overall renal remission (RR 0.82, 95% CI 0.60 to 1.11), partial renal remission (RR 0.94, 95% CI 0.79 to 1.12), or complete renal remission (RR 0.52, 95% CI 0.23 to 1.21)14,17,18.
There was no significant difference between MMF and CYC for ESRD over longterm followup (RR 2.24, 95% CI 0.80 to 6.30)14,16,18. Eleven patients developed ESRD in the CYC group and 4 in the MMF group. In the Ginzler, et al study, the duration of followup was similar in the 2 groups (36.2 ± 16.9 months in the MMF group vs 37.2 ± 16.9 months in the CYC group). Renal failure and death were twice as frequent among patients in the CYC group compared with those in the MMF group, but the number of events was not statistically significant14. The duration of followup in the study by Chan, et al was 63 months and the mean followup period was 37.8 ± 7 months in the study by Ong, et al for the whole group16,18.
The rate of ESRD ever reported (during study period and longterm followup) was significantly higher among patients given CYC than among those given MMF. Twenty-six patients developed ESRD in the CYC group and 12 in the MMF group14,16,17,18.
There was no significant difference between MMF and CYC for death over longterm followup (RR 2.00, 95% CI 0.73 to 5.43). Eleven patients died in the CYC group and 5 in the MMF group14,16,18.
There was no significant difference between MMF and CYC for death ever reported (RR 1.15, 95% CI 0.47 to 2.82). Sixteen patients died in the CYC group and 14 in the MMF group14,16,17,18 (Table 4).
DISCUSSION
In our systematic review, we showed that MMF is not superior to CYC for renal remission (partial, complete, and overall) during induction therapy for LN. The rates of alopecia and amenorrhea in patients treated with MMF were lower than among patients given CYC. The risk of ESRD was reduced among the MMF-treated group during study period and longterm followup (ever reported). This should be interpreted with caution in clinical practice since the same results could not be demonstrated when we analyzed the data available during study period or longterm followup separately. The difference in rates of anemia, leukopenia, infections, gastrointestinal symptoms, and herpes zoster between both groups was not statistically significant. The definitions of leukopenia and infection were heterogeneous among studied trials, which could have accounted for the wide difference in the reported rates of these events, especially infections.
In all studies, participants and personnel were not blinded to the drugs; however, this is unlikely to affect the determination of the primary outcome. There has been a statistically insignificant tendency for anemia to occur more commonly in the MMF group compared to CYC; this is to be reconfirmed because only 2 studies in the metaanalysis reported on anemia and Health Canada has previously issued a warning on the risk of pure red cell aplasia in patients receiving MMF concomitantly with other immunosuppressive agents28.
Published RCT and metaanalyses are not in total agreement and their results are inconsistent. This could have resulted from the heterogeneity in patients’ demographics and characteristics, study methods, inclusion criteria, and objectives, and to the same extent the dose and route of administration of CYC and MMF adopted in each study. Our findings substantially differ from those reported previously by Zhu, et al and Moore and Derry, who concluded that MMF was superior to CYC in inducing remission in LN24,25. Moore and Derry showed that the occurrence of infections, serious infections, leukopenia, amenorrhea, and alopecia with MMF was significantly less frequent, compared to the CYC group24. These results could not be reproduced by Zhu, et al except for infection and leukopenia, while Walsh, et al reproduced only for amenorrhea13,25. Mak, et al found significantly less amenorrhea among the MMF group23. However, the collection of data differed among the metaanalyses13,23,24; in our metaanalysis we included published RCT on induction therapy of LN. Zhu and colleagues evaluated published RCT for induction and maintenance therapy of LN, while Moore and Derry studied RCT, cohort studies, and abstracts for induction and maintenance therapy of LN24. Moreover, Mak, et al conducted a metaanalysis and metaregression, reviewing the literature until 2008 and including published RCT and abstracts23. This could explain the discrepancies in the results.
Mak and colleagues concluded that MMF offers similar efficacy to CYC regarding renal remission and renal survival. Further, they stated that MMF showed fewer side effects than CYC. Based on the data they analyzed, they showed that MMF is encouraged in nonwhite and non-Asian patients with severe LN, at least for induction therapy23. In their analysis, they included the Ginzler, et al trial, which attempted to compare the renal response with MMF among different races and ethnicities14. Ginzler, et al may have been able to report therapeutic success because that study reached a dose of 3 g/day MMF among a majority of high-risk patients and blacks14. This regimen was based on transplantation data suggesting that black patients require higher doses of MMF. Fifty-six percent of the patients were black (43 patients in the MMF group and 36 in the CYC group). This could have biased the results of the trial to a certain ethnic group. Nevertheless, when we interpret the data of 3 trials excluding Ginzler, et al, the statistical heterogeneity was absent but the renal outcome did not change. In our metaanalysis we included the RCT conducted by Appel and colleagues, which has the highest number of patients with LN ever studied in RCT17. In this trial, the sensitivity analysis showed that the number of patients achieving the primary efficacy endpoint, which was a partial renal remission, was not statistically significantly different between MMF and intravenous CYC. Response rates were similar for Asian and white patients; however, among a group referenced as “other” and mostly comprising black and mixed-race patients, 60.4% responded with MMF and 38.5% with CYC. Posthoc analysis showed that response rates among Hispanic patients were 60.9% for MMF and 38.8% for CYC. This is an interesting observation confirming Ginzler’s as well as other studies, which showed that black race, minority ethnic background, and low socioeconomic status are associated with poor outcome (an outcome not mitigated by CYC therapy)29,30,31. In our metaanalysis, we could not study further the interaction between treatment group and race because Ginzler’s paper did not report the data about the effect of medications on each race14. Further, we could not study the potential interaction between ethnicity and MMF dosing regimen and the implications on adverse event rates because of the lack of data.
This systematic review is strong because it is focused and covers an extensive literature search. It included 618 patients reported in RCT for induction therapy of LN by multiple studies and different centers. We aimed to interpret the data available from RCT published in full manuscript form as suggested by the Cochrane Database of Systematic Reviews. This resulted in limiting the number of included studies in our metaanalysis to 4 RCT. It is very unusual to eliminate the risk of publication bias when the number of studies is as small as in our metaanalysis. Moreover, the results are heavily subject to random error, and thus our findings should be interpreted with caution. Other meta-analyses included published abstracts in their analysis and this limits the reliability and interpretation of their results. Other limitations in our metaanalysis included heterogeneity in patients’ demographics, clinical difference in the studies, lack of a standard regimen in all RCT on MMF dose and CYC dose, route of administration of CYC, the heterogeneity of the definitions of infections and leukopenia among trials, missing data on interaction between treatment group and race, and missing data on side effects to treatment group. All these features could have an effect on renal remission outcomes and underestimate or overestimate the RR of adverse effects of both MMF and CYC. This highlights the need for future RCT, which should address these perspectives. The fact that the included RCT in our metaanalysis had patients from different ethnicities increases the generalizability of the results. However, since disease severity and progression might differ among ethnicities, the result of our metaanalysis might not truly reflect the efficacy and safety profile of MMF for all ethnic groups.
The included trials in our metaanalysis reported on primary and secondary outcomes at 6 months14,17,18. One trial defined failure of induction immunosuppressive treatment within 12 months after starting treatment and provided data for both primary and secondary outcomes for 12 months18. This approach may have allowed more information to be identified regarding subsequent increase in remission rates because of the continued improvement of renal outcomes commonly observed after the first 6 months, or may have overestimated subsequent occurrence (or resolution) of adverse events. We strongly encourage publication of longterm outcomes of these patients.
Further research considerations are needed to answer certain critical questions. Current RCT have used different MMF and steroid doses, and optimal regimens have yet to be established. Does MMF use have the same results among different races? Does MMF have the same results among patients with advanced ESRD, knowing that the toxicity of MMF may increase in this group32? Will MMF treatment as induction for LN decrease the rate of adverse events in the long term? Does the dose and duration of MMF used in induction and maintenance phases in LN affect the incidence of relapse and renal outcome? Does MMF differ in terms of short and longterm renal outcome when comparing MMF and other immunosuppressants in maintenance therapy for LN?
In our metaanalysis we could not show that MMF is superior to CYC for inducing remission of LN. MMF is an alternative to CYC in inducing renal remission. We found a tendency toward fewer adverse events in the short and long term with the use of MMF in the induction of LN compared to CYC, notably, less amenorrhea and alopecia. Although comparing MMF to CYC did not demonstrate a statistically significant difference in the rate of adverse events related to leukopenia and infections, there was a tendency to fewer events with MMF. These results should be interpreted with caution given the small number of RCT included and patients’ sample size in our metaanalysis.
Acknowledgment
The authors thank investigators of the original trials for providing data on secondary outcomes.
- Accepted for publication September 7, 2010.
APPENDIX 1. Literature search terms
-
exp lupus erythematosus, cutaneous/ or exp lupus erythematosus, systemic/
-
((mycophenolate adj2 mofetil) or cellcept).mp. or Mycophenolic Acid/ or (myfortic or mmf or “Erl 080” or Erl080 or “Erl 080a” or Erl080a or Melbex or “Nsc 129185” or Nsc129185).mp.
-
1 and 2
-
limit 3 to (clinical trial, all or clinical trial, phase I or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or clinical trial or comparative study or controlled clinical trial or meta analysis or multicenter study or randomized controlled trial) (64)
-
exp case-control studies/ or exp cohort studies/ or exp cross-sectional studies/ or exp clinical trials as topic/ or cross-over studies/ or double-blind method/ or meta-analysis as topic/ or random allocation/ or sample size/ or single-blind method/ (1433808)
-
3 and 5
-
6 or 4








{kind=link}
{kind=link}
{kind=link}