

Abstract
Objective. To evaluate some measurement properties of the Myositis Activities Profile (MAP) in adult patients with polymyositis (PM) and dermatomyositis (DM) in the United States.
Methods. To assess content validity, patients with PM/DM rated difficulty and importance of items of the MAP using a visual analog scale (VAS), range 0–10. For construct validity, consecutive patients with PM/DM performed the 6-item core set for disease activity including the manual muscle test (MMT) and the Health Assessment Questionnaire (HAQ), the Functional Index-2 (FI-2; muscle endurance), and the MAP plus disease effect on well-being on a VAS. Item fit within subscales was analyzed by Cronbach’s alpha. Patients with stable disease activity filled out the MAP again 1 week later.
Results. The median combined difficulty and importance, 0–10, of the 31 items was 5.00 (range 2.10–5.95). One item was added, giving a 32-item MAP. Correlations between the median of subscales/single items of the MAP and the HAQ and disease effect on well-being were rs = 0.69 and rs = 0.68, respectively, with lower correlations to the MMT (rs = −0.35), and the FI-2 (rs = −0.29 to −0.47) and disease activity measures (rs = 0.36–0.41). Cronbach’s alpha coefficients for the 4 subscales varied between 0.85 and 0.95. Weighted kappa coefficients (Kw) ranged between 0.77 and 0.93 for the 4 subscales and between 0.74 and 0.83 for the 4 single items without systematic variations (p > 0.05).
Conclusion. This initial validation of the MAP indicates promising measurement properties for assessing limitations in activities of daily living and participation in patients with PM/DM in the United States.
Adult polymyositis (PM) and dermatomyositis (DM) are rare systemic inflammatory conditions with an incidence of 0.3–0.7 per 100,000 and a prevalence of 5–11/100,0001. Muscle impairment, general fatigue, and interstitial lung disease (ILD) are common symptoms2,3. High-dose corticosteroids and immunosuppressive agents are used3 and accumulated evidence supports adapted exercise as part of the treatment4. Although most patients respond favorably to treatment, many develop sustained disability5 and reduced perceived health6. Activity limitations, e.g., limitations in activities of daily living, increased over a 5-year period for patients with PM and DM, with correlations between higher corticosteroid doses and increased Stanford Health Assessment Questionnaire (HAQ) scores7. In addition, a polyphasic or chronic progressive disease course and osteoporosis were predictive factors for higher Health Assessment Questionnaire (HAQ) scores8. Limitations in sexual activity, walking, biking, social activities, and sleep were disease consequences identified as most important to improve by patients with chronic PM and DM in Sweden9.
The HAQ is the outcome measure most commonly used to assess activity limitation in myositis. However, it is arthritis-specific and not yet validated for adult patients with PM or DM. Nonetheless, the HAQ is included in the 6-item core set of measures recommended for assessment of disease activity in patients with myositis in clinical trials10. The first disease-specific activity limitation questionnaire, the Myositis Activities Profile (MAP)11, was developed for patients with PM and DM in Sweden. It was based on the International Classification of Impairments, Disabilities and Handicaps-2 (ICIDH) Beta-2 draft12, an earlier version of the International Classification of Functioning, Disability and Health (ICF)13. Swedish patients with PM and DM with varying disease activity rated the difficulty and importance on separate visual analog scales (VAS) of 81 items in the ICIDH-2 Beta-2 draft identified by a group of health professionals as relevant for individuals living in Western countries. Patients were also invited to suggest additional items. Based on these results and additional analysis of internal consistency and redundancy as well as test-retest reliability, a 31-item MAP was developed. It asked the patients to weigh both difficulty and importance of each item, on a 7-grade ordinal scale, according to the wording, “how much trouble does. . .cause you in daily life?”. The 7-grade ordinal scale was chosen following advice from the statistician to produce optimal sensitivity to change with acceptable test-retest reliability. Items were divided according to the domains of the ICIDH-2 Beta-2 draft. The MAP showed the highest correlation to the HAQ, with lower correlations to measures of other constructs; and demonstrated good to excellent test-retest reliability11. Today the MAP is used in clinical practice and research in Sweden. It has been used in a short-term exercise intervention study, but showed no statistically significant change at group level, although a few patients responded by improving 2 or more scale steps. The research group considered this a clinically relevant change14. However, further studies are needed to investigate sensitivity to change after different interventions and in followup. The MAP assesses activity limitation with a broader perspective, also including the concept of how important each activity is for an individual to perform. Thus an activity that is moderately difficult to perform might be considered to cause severe trouble in daily life if the individual wants to or needs to perform it very often. Conversely, an activity that is very difficult to perform but is rarely or never done might not cause so much trouble in daily life. Patients’ ability to weigh both the difficulty and the importance of activities as a single issue has not been investigated. The MAP was recently translated into American English but has not yet been validated for use in the United States. No validated myositis-specific activity limitation measure is available in the United States, although there is a need for an instrument that could improve understanding of how PM and DM affect activities of daily living and aid in assessment of treatment effects in these patients.
Our aim was to evaluate some aspects of the content and construct validity and the test-retest reliability of the MAP in adult patients with PM and DM in the United States.
MATERIALS AND METHODS
Patients
Two cohorts of patients were included. Cohort 1 was 29 patients chosen to represent diversity in sex, age, diagnosis duration, disease activity, ethnicity, and social and employment status, who were identified from medical records of the Rheumatology Division, Mayo Clinic, Rochester, Minnesota, USA. Cohort 2 was all consecutive patients visiting the Rheumatology Division at the Mayo Clinic between 2007 and 2008 (n = 70). Inclusion criteria for both cohorts were diagnosis of probable or definite PM or DM according to Bohan and Peter criteria15,16 and ability to speak and understand English. Excluded were patients diagnosed with inclusion body myositis according to the Griggs criteria17.
Disease measures
The 6-item core set for assessment of disease activity for inflammatory myositis trials was used: physician’s assessment of disease activity on a VAS, the manual muscle test (MMT), the HAQ, analysis of the muscle enzymes creatine kinase, aspartate aminotransferase, alanine aminotransferase, lactate dehydrogenase, and aldolase, and the extramuscular disease activity scores on the extramuscular Myositis Activity Index (MYOACT) and the Myositis Intention to Treat Index (MITAX)10,18. The MMT 8-muscle group was applied on the dominant body side and included neck flexors, deltoids, biceps brachiae, wrist flexors, gluteus maximus, gluteus medius, quadriceps, and dorsi flexors of the ankle, with a total score varying from 0 to 80, where 80 indicates good strength. The HAQ is an arthritis-specific activity-limitation questionnaire19 with 20 activities divided into the 8 categories: Dressing and grooming, Rising, Eating and preparing meals, Walking, Personal hygiene, Reaching, Gripping, and Other activities. Total score varies from 0–3 (0 = no activity limitation). The MYOACT is scored as the sum of 6 individual organ systems on a VAS, 0–10: Constitutional, Cutaneous, Skeletal, Gastrointestinal, Pulmonary, and Cardiac. The sum score is divided by 60, for a total score ranging from 0–1 (0 = no disease activity)18. The MITAX is scored as the sum of the highest categories selected for each of the 7 organ systems: Constitutional, Cutaneous, Skeletal, Gastrointestinal, Pulmonary, Cardiac, and Muscle. The sum of these 7 organ systems is divided by 63, creating a total score ranging between 0–1 (0 = no activity)18.
Muscle impairment
Muscle endurance on the dominant body side was assessed using the shoulder abduction and hip flexion tasks of the disease-specific Functional Index-2 (FI-2). Each muscle group is scored as the number of correctly performed repetitions varying from 0–60 (60 = normal endurance)20.
Activity limitation
The MAP, a self-administered questionnaire11 translated into American English, was assessed. Its 31 activities are divided into 4 subscales: Movement, Moving Around, Self-care, and Domestic; and 4 single items: Social Activities, Avoiding Overexertion, Work/school, and Leisure activities. Each item is scored on a 7-grade ordinal scale: 1 = no difficulty, 2 = slightly difficult, 3 = somewhat difficult, 4 = moderately difficult, 5 = very difficult, 6 = extremely difficult, and 7 = impossible to do. For the subscales Movement (8 items), Moving around (4 items), and Domestic (6 items), the median values, 1–7, are scored as the lowest of the 2 middle values. For the subscale Personal care (9 items) the median value is scored. Single items are scored as the actual item score11. The MAP is not calculated as a total score: each subscale and single item is scored separately. This allows presentation of a profile of disability with information on what activities are most limited. For missing item responses, the subscales are scored as the lowest of the 2 middle values or as the middle value depending on an odd or even number of items left.
Well-being
Global disease effect on well-being was assessed on a VAS, 0–100, with the wording, “What impact does your myositis have on your general well-being?”, where 0 = no impact, 10 = maximal impact.
Experimental procedures
The MAP was translated into English by a registered translator and then translated back into Swedish by a bilingual health professional as described21. The wording “trouble in daily life” in the original publication11 was translated as “Difficulty” in American English. Otherwise no changes were made during the translation process. Five patients with PM or DM were then recruited from the American Myositis Association and asked to comment on the wording and understanding of the items. The first author then discussed the adaptation with the translator and a bilingual rheumatologist over the telephone. No need for further adaptation was identified at this stage.
Cohort 1 was included for evaluation of content validity of the MAP and received the first draft of the MAP by mail. To evaluate both the difficulty and importance of each activity the scale was modified to include two 10-cm VAS for each item, one for the difficulty performing each activity in daily life and one for the importance of performing each activity. Patients were also asked to list other important activities in an open question at the end of the questionnaire. A second draft was then developed based on these initial findings including the items scored as the median value or above of combined difficulty/importance. Based on the development of the original Swedish version of the MAP, a cutoff of combined difficulty/importance of > 6 for inclusion in the second draft was hypothesized. In the second draft, each question was rephrased as: “How much difficulty do you have. . . in your daily life?”. The second draft of the MAP was presented to patients in cohort 2 for evaluation of construct validity. Before filling out the questionnaire, patients were given written instructions phrased as: “Difficulty pertains to both how hard it has been for you to complete activities, as well as how important it was for you to be able to perform that particular activity. Try to weigh your difficulties with your needs as you answer the questions”.
The 6-item core set assessment of disease activity was performed by a physician (SRY) while the FI-2, MAP, and the rating of disease effect on general well-being were assessed by a physical therapist (HA). All measures were collected on the same day for most patients or in some cases within the same week.
We hypothesized that the second draft of the MAP would correlate moderately or highly with another activity limitation measure (HAQ) and a participation restriction measure (disease effect on well-being), with moderate correlations to muscle function measures and low correlations to disease activity measures.
All patients in cohort 2 with unchanged medication and disease activity for 1 month (n = 49) were included for test-retest analysis, receiving another copy of the MAP to fill out 1 week later at home and send back to the clinic. Unchanged medication and disease activity was defined as no appreciable change in physician’s global assessment of disease activity on the VAS, total MMT score change < 2 points, or single muscle group score change < 1 point, stable muscle enzymes, and no evidence of new extramuscular disease activity compared to the previous clinical visit.
Data analysis
Data are presented as median values with lower and upper quartiles. The Spearman correlation coefficient was used to correlate the MAP with the HAQ and measures of other constructs. Correlation coefficients between 0 and 0.25 were considered as no or very low correlation, coefficients between 0.26–0.40 as low correlation, coefficients between 0.41–0.69 as moderate, coefficients between 0.70–0.89 as high, and coefficients between 0.90–1.0 as very high22. Cronbach’s alpha coefficient was used to evaluate item fit within the subscales. For scales used in research, reliability coefficients < 0.70 are generally seen as inadequate23. The weighted kappa coefficient (Kw) was used to analyze random variation between test and retest of subscales and also for each item of the MAP. Weighted kappa coefficients between 0–0.20 were considered as no or low agreement, 0.21–0.40 as fair, 0.41–0.60 as moderate, 0.61–0.80 as substantial, and 0.81–1.0 as almost perfect24. The Sign test was used to analyze systematic variation between test and retest of the MAP, at a significance level of p < 0.05.
The study complied with the Helsinki Declaration and was approved by the Mayo Clinic institutional review board. All patients signed informed consent forms before entering the study.
RESULTS
Content validity
Twenty-nine patients were invited to participate in cohort 1. Eight declined, one because of recent hip and shoulder replacement and the others for unknown reasons, thus the results are based on the remaining 21 patients who returned the first draft of the MAP. Patients in cohort 1 included 21 patients (13 women, 8 men), 7 with PM (3 definite and 4 probable diagnosis), 13 with DM (10 definite and 3 probable diagnosis), and 1 with definite juvenile DM; patients had a median age of 53 years (range 24–76). Three patients also had ILD. Eighteen were white, 2 African American, and 1 a Pacific Islander. Median disease duration was 3 years (range 0.2–18). Disease activity was rated low in 9, moderate in 5, and moderate-high in 5. The median daily prednisone dose was 10 mg (range 0–50 mg); 10 patients were taking an immunosuppressive agent, 1 a tumor necrosis factor inhibitor, and 1 intravenous immunoglobulin. Twelve patients were employed, 3 were retired, 3 were on sick leave, 2 were homemakers, and 1 was a student. Eight patients were married with children, 8 were married without children, and 5 were single without children. Five lived in a city with population > 200,000, 4 in a city of 40,000–100,000, 13 in a town of 1000–40,000, and 1 in a rural area with population < 1000.
The median value for difficulty of each activity was 1.70 (0.50–2.80) ranging from 0.10 to 7.70, and the median value for importance for each activity was 9.60 (9.20–9.80) ranging from 1.80 to 10.00. The combined difficulty and importance of each activity was median 5.00 (5.00–5.25) ranging from 2.10 to 5.95 for the 31 activities in the first draft of the MAP (Table 1). Based on these results, a cutoff limit for difficulty and importance combined was set to 5.00 or above, somewhat lower than we had hypothesized. “Standing for a longer period” (combined median 4.90) and “Using public transportation” (combined median 2.10) were rated < 5.0. Following discussions in the research group and an informal discussion with patients at a patient group meeting, this latter activity was modified to replace train travel by air travel. Although rated below 5.00, these 2 activities were not excluded because they were considered to be more relevant in populations living in larger cities. Five patients suggested “Opening jars” and this activity was added to the Movement subscale according to the ICF domain structure, giving a 32-item second draft of the MAP. Other activities suggested by only 1 patient each were: “Squatting,” “Keeping up with children during play,” “Sitting without back support,” “Watching soccer/baseball games,” “Going on vacation,” “Getting up from floor,” “Punching door codes,” “Changing gear when driving,” “Having to pre-plan every day,” “Talking on the phone too long,” “Worrying,” “Time management due to fatigue,” “Walking on a steep incline,” “Applying make-up and hair conditioning,” “Fine motor applications,” and “Singing in a choir.”
Ratings of difficulty, importance, and difficulty/importance from patients in Cohort 1.
Construct validity
Of 70 patients invited to participate in cohort 2, 6 declined because of lack of time to perform all the tests (1 with high disease activity, 2 with moderate, and 3 with low). Thus 64 patients were included (Table 2). Patients needed 5 min to complete the second draft of the MAP. As hypothesized, the median of subscales/single items of the second draft of the MAP correlated moderately, almost reaching high correlation coefficients, with the HAQ and disease effect on general well-being. Correlations to measures of muscle function were, as expected, moderate regarding the FI-2 hip flexion, with only fair correlations to the FI-2 shoulder flexion and the MMT. There were low to fair correlations to measures of disease activity (Table 3). Correlations between the MAP subscales Movement, Activities of moving around, Personal care, and Domestic and the HAQ were rs = 0.82, rs = 0.67, rs = 0.69, and rs = 0.70, respectively. Correlations between the MAP single items Social activities, Avoiding overexertion, Work, and Recreational and the HAQ were rs = 0.37, rs = 0.32, rs = 0.52, and rs = 0.53, respectively. Cronbach’s alpha coefficients for the 4 subscales varied between 0.85 and 0.95.
Demographic and descriptive data for Cohort 2 and patients with unchanged disease activity and medication included for test-retest reliability.
Correlations between the median of subscales and single items of the American Myositis Activities Profile (MAP) and other measures.
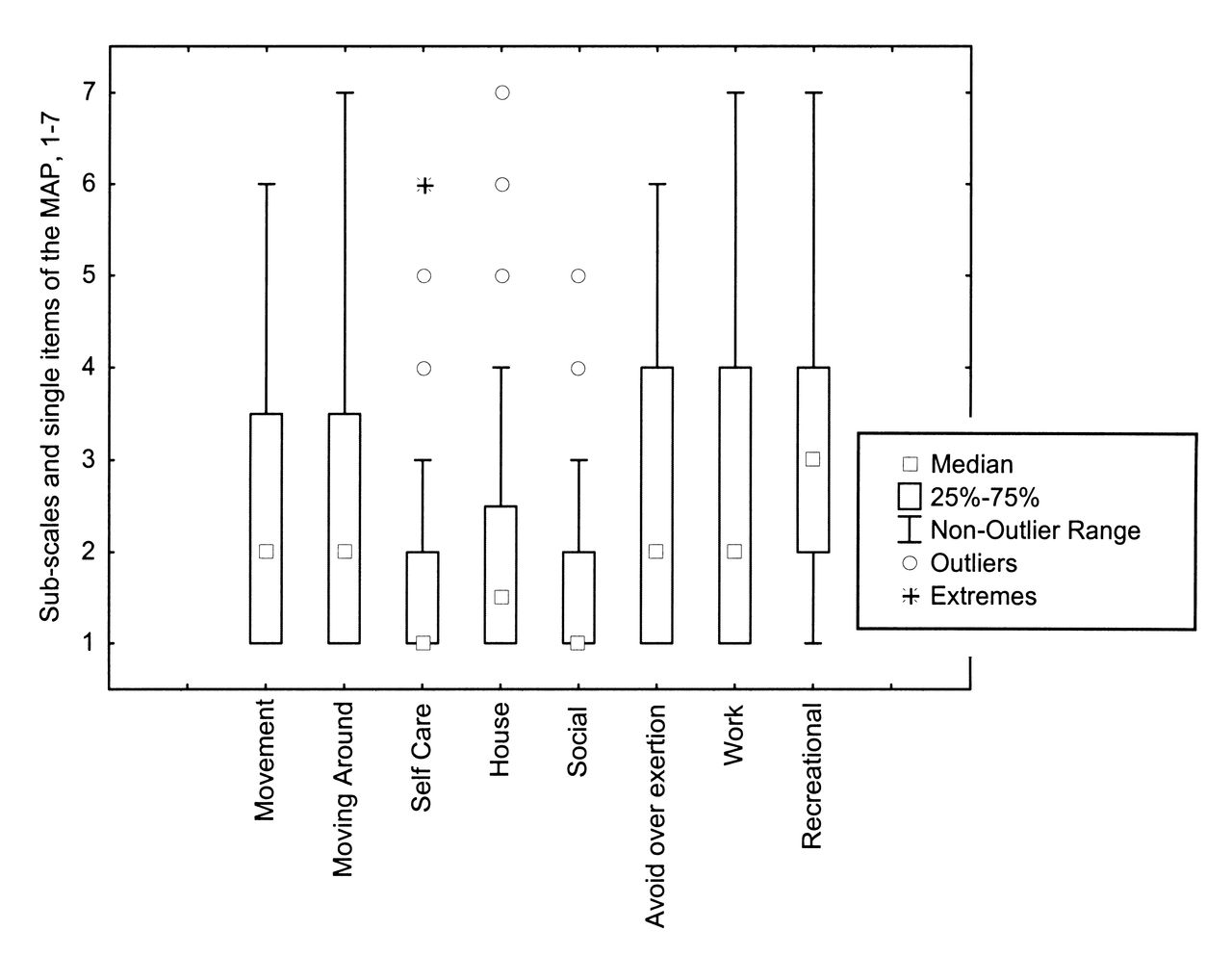
Score distribution of the subscales and the single items of the second draft of the MAP are shown in Figure 1. Seventeen patients (27%) in cohort 2 scored 0 (no limitations) in the HAQ, while 4 (6%) scored 1 (no difficulty/importance) in all subscales and single items of the second MAP draft. A majority stated that the items included in the second draft were relevant in their daily life, although some had difficulty understanding the meaning of the single item “Avoiding overexertion in daily life.”
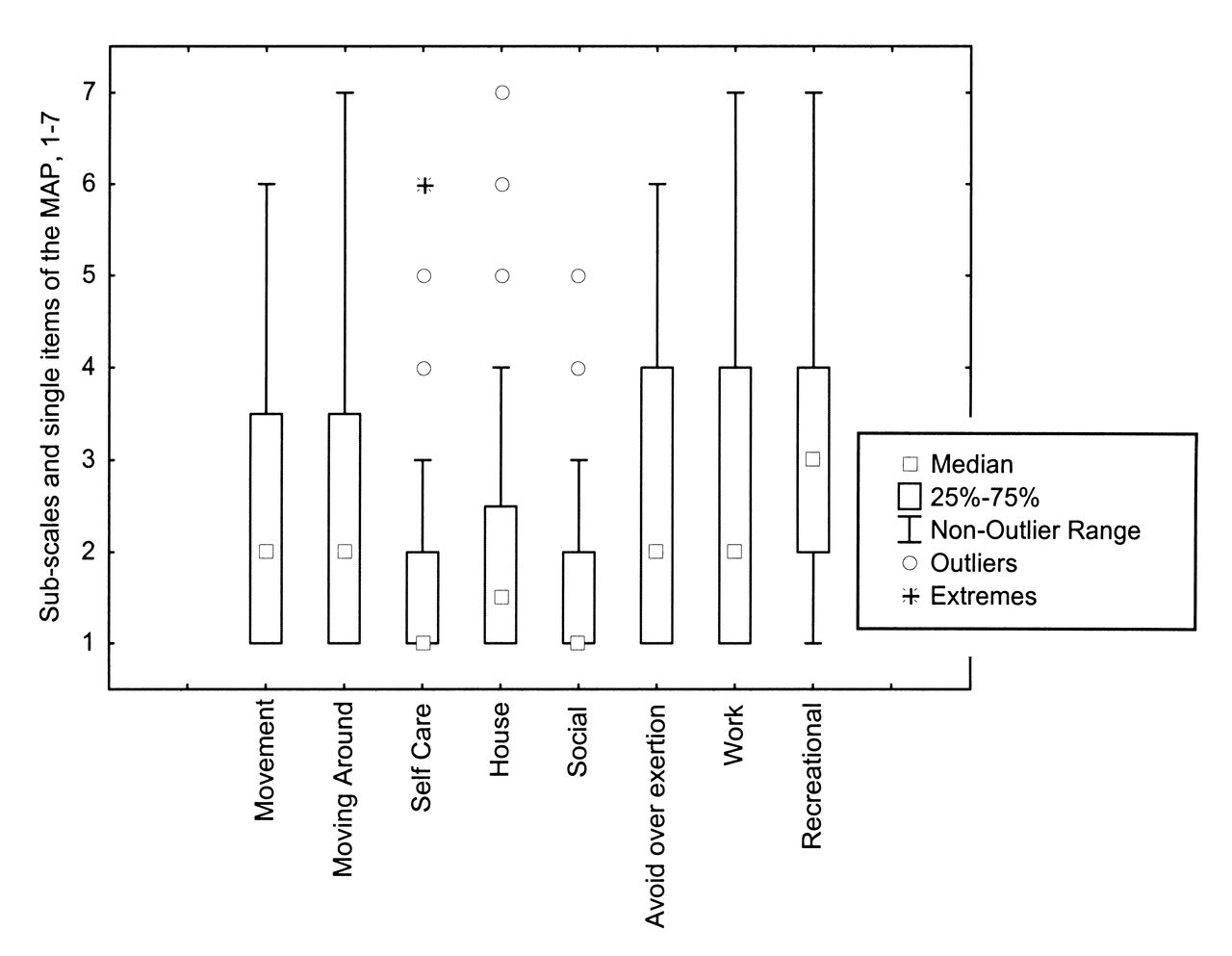
Score distribution of the subscales and single items of the Myositis Activities Profile (MAP); 1 = no difficulty, 7 = impossible to do.
Test-retest reliability
Forty-nine patients in cohort 2 had unchanged disease activity and medication for at least 1 month and 37 returned the questionnaires for analysis of test-retest reliability (Table 4). Weighted kappa (Kw) ranged between 0.77 and 0.93 for the 4 subscales and between 0.74 and 0.83 for the 4 single items of the MAP without systematic variations (p > 0.05). Weighted kappa for each of the 32 items ranged between 0.60 and 0.95. Median values and quartiles for test and retest with Kw and 95% CI for the subscales and single items are presented in Table 4.
Test retest reliability of subscales and single items of the American MAP.
DISCUSSION
The MAP 32-item self-administered questionnaire is the first disease-specific measure of activity limitation/participation restriction available for patients with PM and DM in the US. This initial validation suggests promising content and construct validity and moderate to excellent test-retest reliability.
The majority of activities in the first draft of the MAP were considered by patients in cohort 1 as very important to be able to perform in daily life, while the difficulty ratings for the items were lower. Activities relating to walking, climbing stairs, running, and recreational activities were rated as difficult/important to perform, whereas those relating to personal hygiene imposed less trouble in daily life. This is in agreement with results from the development and validation of the original Swedish MAP11. Similar physical activities have received high priority for improvement by patients with PM and DM9 and by patients with systemic sclerosis, who also have reduced muscle endurance and ILD25.
When the MAP was being developed in Sweden11, patients rated higher difficulty/importance of most activities included (resulting in a median difficulty/importance cutoff of 6 or above for inclusion of items) than did the US patients in our present study. Here, the median difficulty/importance of items was 5.00, giving a cutoff of 5 or above for item inclusion. It cannot be ruled out that the strategically chosen Swedish patients in cohort 1 (n = 10) had more severe disease or worse activity limitation than the present cohort 1 patients. However, this difference could be due to many factors, for example, that the majority of patients in Sweden lived in a metropolitan area whereas most of the present US patients lived in smaller communities. There may also be a cultural difference in the perception of activity limitation and participation restriction. Two activities (“Standing for a longer period” and “Using public transportation”) were not excluded although their rated combined difficulty and importance were < 5.0. This was because they were considered to be more difficult and relevant to patients living in larger cities, where many depend on public transportation, which probably often requires people to stand for considerable periods. Following the analysis of content validity, the item “Using public transportation” was modified to include air travel instead of train. This was also considered to increase the relevance. The relevance of the item “Using public transportation” was not commented on by the 5 patients involved in the initial translation of the MAP, perhaps indicating that more patients should have been included in the translation phase. In our cohort 1, 5 patients suggested the activity “Opening jars” for inclusion in the second draft of the MAP. Other activities were suggested by only 1 person, and several of these were included in the single items “Recreational activities” or “Avoiding overexertion,” and thus were omitted from the second draft of the revised MAP. As expected, the second draft correlated best to measures of activity limitation and participation restriction, and less to measures of impairment and disease activity. These results are in agreement with the validation of the Swedish MAP, although even lower correlations were shown between the Swedish MAP and CPK levels used as a measure of disease activity. This difference could be because the present 6-item core set includes measures of both muscle function and activity limitation when assessing disease activity. Lower correlations between measures of activity limitation and disease activity were also evident when validating the semistructured McMaster Toronto Arthritis Patient Preference Questionnaire (MACTAR) in patients with myositis9, while activity limitation assessed with the HAQ correlates well to disease activity in patients with rheumatoid arthritis26,27,28. Patients with PM and DM have inflammatory infiltrates in muscles not affected by muscle weakness29, which indicates that disability may not be associated with active myositis. The median of all subscales and single items of the MAP correlated well with the total HAQ score, indicating that the MAP does measure activity limitations. The MAP subscales also correlated well with the HAQ, while there were only low to moderate correlations between the MAP single items and the HAQ. This could be because the subscales include activities partly similar to those in the HAQ. The HAQ does not include categories such as social activities, ability to plan activities, work/school, or recreational activities.
In cohort 2, 27% of patients scored 0 (no limitation) on the HAQ, while 6% scored 1 (no limitation) in all subscales and single items of the MAP. This could indicate that the MAP is more sensitive to activity limitations in patients with PM and DM than is the HAQ. However, the MAP was not distributed to healthy controls matched for age and sex, which is a limitation of our study. Although scores were distributed almost across the whole range in the majority of subscales and single items of the MAP from 1–7, median values were lower, varying between 1 and 3, implying that there is a risk of ceiling effects in several subscales and single items of the MAP. As patients in cohort 1 scored “Difficulty of activities” rather low and “Importance” very high, further investigation to evaluate patients’ ability to weigh both difficulty and importance is needed. Also, further use of the MAP in intervention studies is needed to evaluate whether this score distribution contributes to potential ceiling effects and to study the sensitivity to change of this new questionnaire.
All subscales and single items demonstrated moderate to excellent test-retest reliability, equivalent to the reliability analysis run for the Swedish MAP. Some patients, when filling out the MAP, asked about the meaning of the single item “Avoiding overexertion,” which could indicate a need for it to be rephrased. However, as the Kw analysis suggested a substantial agreement between test and retest for this item, it was not excluded.
The content validity of the original MAP was based on patients’ rating of difficulty and importance of items in the ICIDH-2 Beta-2 draft. As our present study set out to evaluate the content validity of the original MAP in patients with PM and DM in the United States, no further literature was included in the validation process. Patients with PM and DM may well be the real experts on disease consequences in myositis, so we believe that their ratings of difficulty and importance of the items and their suggestions for additional items strengthen our study. However, the fact that most patients were white people living in smaller communities in the upper midwestern United States is a limitation. A larger sample size including more patients representing other ethnicities and more urbanized areas would have strengthened the content validity of the MAP. Further, patients with both probable and definite diagnoses were included, as PM and DM are very rare conditions. However, there is to our knowledge no publication describing difference in disability in patients with probable and definite diagnosis.
In cohort 2, six patients with various disease activity and diagnosis durations declined participation. It is not likely these dropouts significantly affected the construct validity analysis, but cohort 2 had low disease activity scores. A broader variety in disease activity would have been preferred to strengthen the construct validity results. Twelve of 49 patients with stable disease did not return the second copy of the questionnaire to assess test-retest reliability. The CI for the Kw of the subscales were fairly small, which was true for most of the individual items except Climbing stairs, indicating reliable analysis and a sufficient number of participants24. The study evaluates some aspects of validity, but as PM and DM are rare diseases, our ability to perform robust psychometric evaluations was hampered. No fewer than 150 patients or a recommended 460–930 patients should have been included for adequate factor analysis of the MAP30, necessitating a multicenter trial. Rasch analysis or Item Response Theory analysis was not undertaken, which is a limitation. However, high to very high Cronbach’s alpha coefficients showed that all items contributed equally to the sum of their subscale score, indicating good item fit. A population of at least 68 subjects is recommended to achieve statistical power for correlation analysis22, which our study almost managed.
The initial validation of the MAP revealed promising measurement properties in assessment of activity limitation/participation restriction in patients with PM and DM in the United States. The instrument is easily administered and not time-consuming, and could improve clinical assessment in these patients. However, further validation is needed to establish sensitivity to change and patients’ ability to weigh both the difficulty and the importance of items.
Acknowledgment
We thank all participating patients, and Elisabeth Berg, KI, for statistical advice, and Tim Crosfield for linguistic checking.
Footnotes
-
Supported by the Centre for Care Science, Karolinska Institutet, Stockholm, Sweden.
- Accepted for publication July 6, 2012.








{kind=link}