

Abstract
Objective. To synthesize descriptions of periarticular findings at the metacarpophalangeal (MCP) and wrist joints in different types of arthritis and in the normal state imaged by high-resolution peripheral quantitative computed tomography (HR-pQCT); to assemble the literature reporting on the ability of HR-pQCT to detect findings relative to other imaging modalities; and to collate results on the reproducibility of image interpretation.
Methods. A systematic literature review was performed using terms for HR-pQCT and MCP or wrist joints using medical literature databases and conference abstracts. Any study describing predefined pathology findings, comparison to another radiographic technique, or a measure of reproducibility was included with no limitation by disease state.
Results. We identified 44 studies meeting inclusion criteria from the 1901 articles identified by our search. All 44 reported on pathology findings, including erosions (n = 31), bone microarchitecture (n = 10) and bone mineral density (n = 10) variables, joint space evaluation (n = 7), or osteophyte characterization (n = 7). Seventeen of the studies compared HR-pQCT findings to either plain radiography (n = 9), ultrasound (n = 4), magnetic resonance imaging (n = 5), or microcomputed tomography (n = 2), with HR-pQCT having high sensitivity for erosion detection. Twenty-four studies included an assessment of reproducibility with good to excellent metrics, and highlighting the critical importance of positioning when assessing joint space variables.
Conclusion. Despite high sensitivity for erosion detection and good reproducibility, more research is required to determine where HR-pQCT can be applied to enhance our understanding of periarticular bone changes in a variety of arthritis conditions.
Diagnostic imaging plays a prominent role in the diagnosis and monitoring of disease progression in arthritis conditions. Plain radiography, magnetic resonance imaging (MRI), and ultrasound (US) dominate the current field and provide complementary information on the degree of both active and chronic changes1. Computed tomography (CT), however, remains the best modality to assess bone2. High-resolution peripheral quantitative computed tomography (HR-pQCT; Scanco Medical AG) is a technical modification of conventional CT designed to examine bone microarchitecture and density, allowing visualization and quantification of the separate behavior of trabecular and cortical bone structures3. This technology has been validated for the examination of systemic bone density and microstructure at the distal radius and tibia in osteoporosis research4.
Recent efforts have been made to use HR-pQCT to assess periarticular bone changes in a variety of arthritis conditions including rheumatoid arthritis (RA) and psoriatic arthritis (PsA), and in normal states. This research has been facilitated under the auspices of the SPECTRA Collaboration (Study grouP for xtrEme Computed Tomography in Rheumatoid Arthritis), an international collective of researchers in engineering, physics, and rheumatology who pursue development of periarticular image acquisition standards5, image interpretation and analysis guides, and applications in clinical research. Because the body of literature has grown substantially, there is a need to summarize findings. The purpose of this systematic review was to (1) summarize periarticular findings at the metacarpophalangeal (MCP) and wrist joints in different types of arthritis and in the normal state; (2) assemble the literature reporting on the ability of HR-pQCT to detect findings relative to other imaging modalities; and (3) collate results on the reproducibility of image interpretation.
MATERIALS AND METHODS
Search strategy
Assisted by a research librarian, US National Library of Medicine Medical Subject Heading (MeSH) terms, keywords, and acronyms for HR-pQCT were selected. We combined this search with MeSH terms, keywords, and acronyms for the metacarpophalangeal joints (MCP) and/or wrists, to specify the periarticular regions of interest in this new application of the imaging modality (search terms, Appendix 2). PubMed (1966–April 2015), Embase (1980–April 2015), and Medline (1946–April 2015) searches were conducted to identify potentially relevant studies. Filters were applied to eliminate animal studies and identify English language studies. We did not specify by disease, to identify studies in both normal state and in a variety of arthritis conditions. A hand search of conference abstracts (American College of Rheumatology, European League Against Rheumatism, Canadian Rheumatology Association, American Society for Bone and Mineral Research) was also performed, and references from identified articles were checked manually.
Inclusion criteria
Any studies reporting original results of HR-pQCT imaging of the MCP and/or wrist joints were selected through the title/abstract search. These studies could report on normal state or any arthritis conditions [including RA, osteoarthritis (OA), PsA], as well as “pre-arthritis” states [e.g., persons positive for anticitrullinated protein antibodies (ACPA) with arthralgias]. At the full text review stage, we selected articles for data extraction if they reported on any of the following outcomes: (1) pathology findings, determined a priori to include bone mineral architecture, bone mineral density (BMD), erosions, vessel channels, cortical breaks, joint space, osteophytes, or surface changes; (2) comparison to other radiography; and (3) reproducibility. Article selection and data extraction were performed by 2 authors (SN and CB). If data from the same study were reported in multiple abstracts, or subsequently published, the full manuscript was preferentially used for data extraction, or the latest version of the abstract was used.
Analysis
Owing to the heterogeneity of case definitions for different pathologies, variations in analysis techniques, and the identification of studies in a variety of normal and disease states, it was not possible to perform any form of metaanalysis. Therefore, a narrative summary of the work was performed following pathology descriptions and comparisons to other radiography and reproducibility.
RESULTS
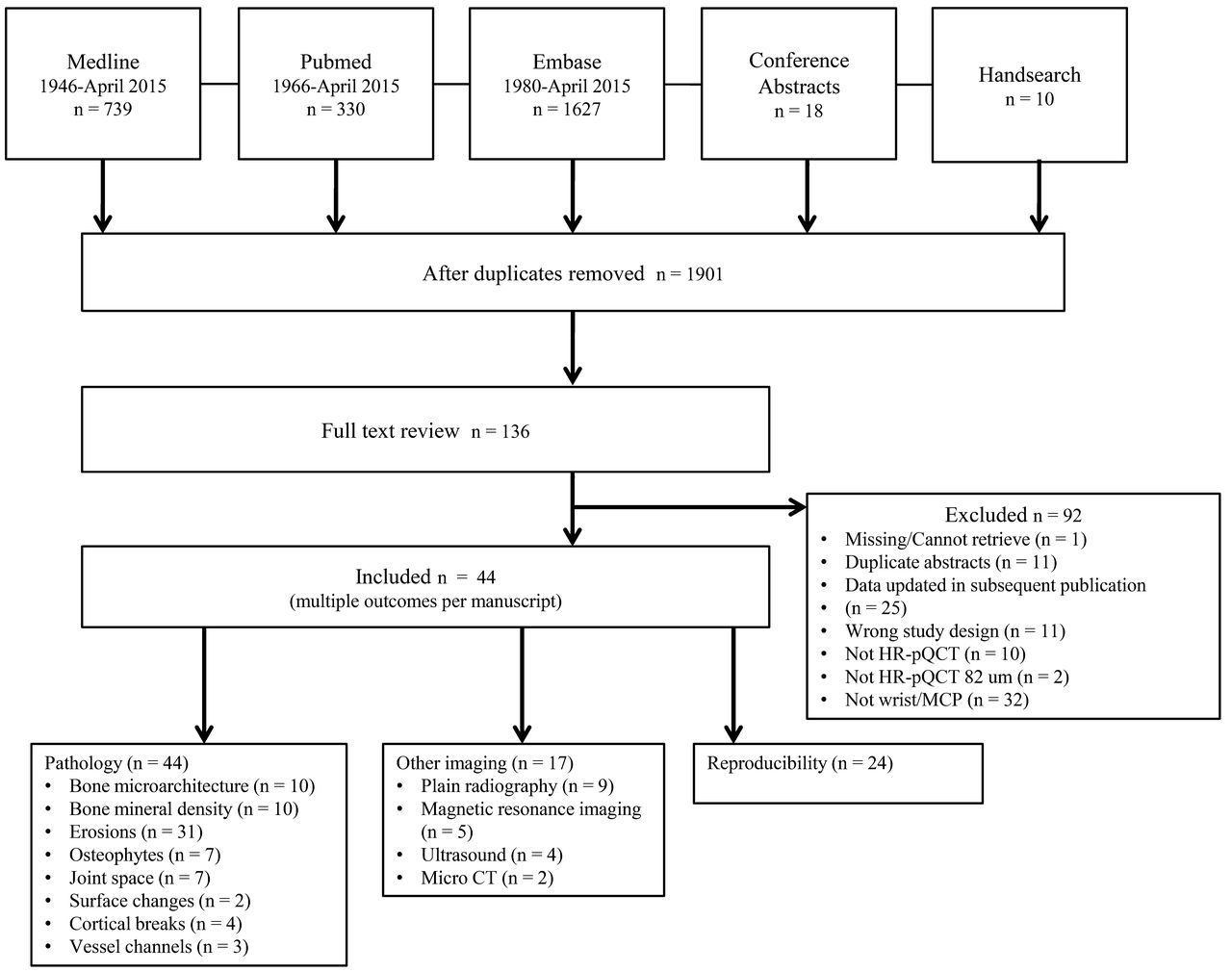
A total of 1901 unique publications was identified, each subject to selection based on the title and abstract. One hundred and thirty-six met eligibility for full-text review, with 44 selected for data extraction. Of the 44 articles, all described pathology findings, 17 related a comparison of HR-pQCT findings to another imaging modality, and 24 described precision or reproducibility (Figure 1). The studies meeting inclusion criteria are detailed in Table 16–15,16–25,26–35,36–45,46–49.

Flow diagram for study inclusion. HR-pQCT: high-resolution peripheral quantitative computed tomography; MCP: metacarpophalangeal (joint).
Studies included in the systematic review.
Pathology
Bone microarchitecture
Kolling, et al47 and Feehan, et al30 studied healthy volunteers only. Kolling, et al found that cortical thickness (CtTh) was higher at the phalangeal base compared to the metacarpal head of the MCP joint. Feehan, et al’s study objective was to evaluate short-term measurement precision at the metacarpal head (as well as metacarpal shaft and ultra-ultra-distal radius). Mean (SD) values for the ratio between bone volume and total volume (BV/TV), CtTh, cortical porosity, trabecular number (TbN), trabecular thickness (TbTh), and trabecular separation (TbSp) were calculated from 10 individuals for the second and third metacarpal heads. Kleyer, et al scanned ACPA-positive and -negative individuals without clinical symptoms of inflammatory arthritis17. The BV/TV was significantly reduced in ACPA+ individuals [mean 17.2 (SEM 0.6)% vs mean 20.4 (SEM 0.4)%, respectively]. Quantitative analysis of trabecular variables showed no significant differences between ACPA+ and ACPA– individuals, although a trend toward thinner trabeculae was observed in the ACPA+ group. The CtTh was significantly lower in the ACPA+ group compared to the ACPA– group (mean 0.22 vs 0.32 mm, respectively).
Five cross-sectional studies compared bone microarchitecture between subjects with RA and controls, with variable findings (Table 2). Of 3 studies assessing BV/TV, one found it to be higher in RA27, whereas it was lower in RA subjects compared to controls in the other 2 studies10,39. TbTh was higher in RA subjects in 1 study27, lower in RA subjects in 2 studies39,46, and not different from controls in 1 study10. TbN was higher in RA subjects in 1 study27, lower in RA subjects in 1 study10, and not different in 2 studies39,46. TbSp and TbSpSD were higher in RA subjects in 1 study10 but not different in the others27,39,46. In 2 studies each, CtTh was lower in RA subjects27,39 and comparable to controls10,46.
Comparison of bone microarchitecture (BMA) findings between rheumatoid arthritis (RA) subjects and controls.
Two studies reporting longitudinal evaluation of bone microarchitecture have been reported. One study of early inflammatory arthritis patients receiving first-line therapy did not find significant changes in quantitative values obtained8. Töpfer, et al selected 5 different texture variables calculated directly from grey value images including global and local inhomogeneity, local anisotropy, variogram slope, and entropy, which are dependent on trabecular architecture in a study of erosions9. At baseline, no significant differences for any of the texture variables were found, when comparing erosions that eventually progressed, regressed, or remained stable.
Bone mineral density
Studies by Kolling, et al47 and Feehan, et al30 of healthy volunteers have evaluated BMD. Kolling, et al reported that the whole (volumetric) BMD (vBMD) increased in the distal region of the MCP, and decreased in value from the second MCP to the fourth MCP47. The study by Feehan, et al provides normative means for vBMD, as well as cortical (CtBMD) and trabecular (TbBMD) compartments at the second and third MCP30. Kleyer, et al’s study in ACPA+ and ACPA– individuals without features of inflammatory arthritis found that vBMD was significantly reduced in ACPA+ individuals (mean 280 vs 327 mg/cm3)17. In studies comparing vBMD in RA subjects to controls, all found lower vBMD in RA10,46 except for one27. Barnabe, et al27, Yang, et al10, and Fouque-Aubert, et al46 found no difference between RA subjects and controls for CtBMD, whereas Zhu, et al39 reported it to be significantly lower in RA. For TbBMD, Barnabe, et al reported it to be higher in RA subjects27, whereas it was lower in late RA subjects only in the study by Fouque-Aubert46, et al, and at the third MCP only in the Yang, et al study10, but significant in the Zhu, et al study39.
In a longitudinal study of changes during 1 year of therapy in early inflammatory arthritis, no significant changes were detected8. Two studies investigated associations between erosions and BMD measures, in particular periarticular regions of interest. In Toepfer, et al37, the percent change in erosion volume correlated significantly with the percent change in BMD. In a more detailed assessment in 2015, it was found that BMD in the immediate vicinity of an erosion was significantly higher than further away from the erosion, perhaps reflecting repair mechanisms9.
Erosions
Thirty-one publications characterizing erosions were found (Table 3). Erosions have been assessed in a variety of arthritis conditions including early inflammatory arthritis, RA, PsA, and erosive hand OA, as well as in persons with psoriasis and healthy controls, and subjects with ACPA antibodies but no features of arthritis. The case definitions used for erosions have also varied; some have required only a break in the cortical shell9 whereas others have specified a minimum number of consecutive slices and planes with cortical breaks, but also requiring changes to be found in the trabecular bone11. Differences in the frequency of erosions likely reflect the underlying disease state (Table 3). In RA, a predilection for the second MCP joint, and in particular for the metacarpal head and radial side of the joint, is consistently noted16,33,35,48. However, in PsA, involvement of the phalangeal base and palmar surface is more common42.
Publications characterizing erosions using HR-pQCT.
A variety of methods to describe erosion size have been proposed, including semiquantitative scores6,48, different approaches to determining erosion volume23,46, sphericity and surface area9,36, and most commonly, direct measurements of the width of the cortical break and depth of trabecular loss11. Eight studies have reported longitudinal changes in the number and/or size of erosions8,9,13,25,37, with some comparing changes with different therapies33,34,45. A small number of articles have characterized osteosclerosis of erosions in relationship to change in size with therapy7,33,45, and 1 article described cystic bone lesions in erosive hand OA43. Detailed summaries of these characterizations appear in Table 3.
Vessel channels
Simon, et al studied subjects with cutaneous psoriasis in the investigation of bone microstructural changes prior to the onset of joint involvement, in comparison to healthy controls21. Patients with psoriasis had significantly more vessel channels (mean 10.8 vs 4.1) at the second metacarpal head. Similarly, more vessel channels were seen in patients with RA compared to healthy controls (mean 4.6 vs 2.3) in a study by Haschka, et al15. Cortical breaks were found in 93% of patients with PsA and 87.5% of patients with PsA in an earlier study reported by Finzel, et al42.
Cortical breaks
Two studies of RA subjects31,41, 1 study of ACPA+ and ACPA− individuals without inflammatory arthritis17, and 1 cadaver study38 have reported on cortical breaks; the former 3 studies used a definition of a break in the cortical lining detectable in 2 perpendicular planes with no size specification, whereas the latter used a minimum break size of > 0.5 mm38. In both Finzel, et al 2012 and Finzel, et al 2011, mean longitudinal and transverse width and depth dimensions of the breaks, relative to controls, were summarized31,41. Kleyer, et al found significantly more breaks in ACPA+ individuals compared to ACPA– (mean 7.4 vs 1.0 breaks, not specified whether total or per joint)17. The Williams, et al study included MCP as well as proximal and distal interphalangeal joints without separating the results at each region, and found 35 breaks in 13 joints38.
Joint space
Several approaches to measuring joint space have been proposed. Barnabe, et al used region-growing image processing in a study of RA subjects matched to healthy controls, finding that MCP were narrowed in the RA group27. In further studies by this group, a custom script applying the approach of “fitting maximal spheres” was applied to estimate mean joint space width in early inflammatory arthritis26, and also in a cadaver study examining changes in mean, median, minimum, and maximum joint space widths and total volume estimates based on angle of positioning12. They also applied this script in assessing treatment effect over 1 year in early inflammatory arthritis, seeing improved/increased joint space at the second MCP8. Burghardt, et al applied a method of voxel counting for joint space volume and a 3-D distance transformation method for morphology also using a method of “fitting of maximal spheres” to examine joint space mean, minimum, maximum, asymmetry, and SD in RA and healthy controls29. RA subjects had a smaller joint space minimum compared to the control group, but without significant differences found for the other variables29. Burghardt, et al also examined the wrist, finding a higher SD of the radiolunate and radioulnar joints in RA subjects, with lower minimum measurement in the radiolunate joint but higher maximum, indicating asymmetry29. Boutroy, et al has also developed an automated algorithm, but technical specifications were not provided28. In an abstract by Finzel, et al comparing RA, PsA, and erosive hand OA, joint space narrowing was measured using a manual technique at medial, lateral, and middle aspects of the joint; however, age, sex, and postmenopausal state were associated with joint space narrowing in the OA subjects43.
Osteophytes
Seven studies, all from the same research group, have applied a definition of osteophytes as bony protrusions from the juxtaarticular cortical shell. In the original publication of RA subjects and healthy controls, osteophytes were described as being small and located at the dorsal and palmar aspects of the joint, with similar frequency of occurrence in the 2 groups and correlating with subject age48. In a 1-year followup study of RA subjects, osteophytes increased in both quantity and size25. Patients with PsA were described as having a more significant osteophyte burden relative to RA. In the study by Finzel, et al in 2011, 16% of RA but 100% of PsA subjects had osteophytes, predominantly located at the second and third MCP rather than the fourth MCP42. The mean number of osteophytes was 11.6 in PsA but only 2.1 in RA, with a mean size of 1.2 mm in PsA versus 0.5 mm in RA42. Also, in RA the osteophytes were predominantly located at the dorsal and palmar aspects of the joint, but those in PsA were located at all aspects and appeared as a bony corona42. In a 1-year longitudinal study of patients with PsA treated with antitumor necrosis factor or methotrexate therapy, osteophytes significantly progressed in size in both treatment groups; and with an RA comparison group there was a similar finding34. A comparison between PsA and hand OA has been performed14. In this study, osteophytes/bone spurs were nearly universal in both conditions, but with PsA having larger spurs, and with different localizations; at the second MCP both phalangeal and metacarpal heads were more likely affected in PsA, and with a predilection for radial aspect. In hand OA it was the third MCP, with palmar and dorsal quadrants affected14. Also in PsA, spurs in entheseal regions were prominent, whereas in OA these were emerging at the cartilage/bone interface and the joint margin14. In psoriasis, 1 abstract describes a population of 55 subjects, all of whom were found to have osteophytes but without further characterization20. One cross-sectional study compares psoriasis patients and healthy controls, with more frequent bony spurs in psoriasis, most commonly located at the second metacarpal head, but being larger in size in psoriasis subjects19.
Surface changes
Using 3-D reconstruction images of the bone surface, alterations of cortical thinning and fenestration but not breaks have been characterized. Surface changes predominated in PsA relative to RA (93% vs 79% of patients had surface changes, respectively) but the extent of the changes was similar between diseases42. Another finding was that of lesser lesion severity at the fourth MCP in PsA compared to RA, whereas these were similar at the second and third MCP42. Controls had small areas of these changes relative to RA subjects48.
Comparison to other radiographic modalities
Seventeen individual publications have compared findings on HR-pQCT to other imaging modalities, including plain radiography, MRI, power Doppler US, high-resolution US, and ex-vivo micro-CT scans, and predominantly for erosion detection but also in correlating findings of inflammation (primarily by MRI) and joint space narrowing. In an abstract, Stach and Schett reported a sensitivity of 0.75 and specificity of 0.85 for HR-pQCT compared to plain radiography to detect small bone erosions49. This abstract was followed by a full publication that reported that 58% of patients with lesions on HR-pQCT had normal radiographs, and that no patient with lesions on radiographs had a normal HR-pQCT scan48. Similarly, authors comparing erosion detection by plain radiography and HR-pQCT have found HR-pQCT to have increased sensitivity8,18,27,38,46. HR-pQCT has been used in further studies as the gold standard for erosions relative to MRI6,7,24,35, power Doppler US31,32,33, high-resolution US44, and plain radiography6. Simon, et al reported poor correlation between bony changes seen in HR-pQCT scans with osteitis and synovitis seen on MRI in patients with psoriasis20. A single study has compared plain radiography scored by the van der Heijde modified Sharp method and an HR-pQCT joint space width measurement algorithm29. Joints with radiographic narrowing had higher joint space heterogeneity and less than half the minimum joint space width on HR-pQCT compared to joints without radiographic narrowing29.
Reproducibility
Reproducibility metrics for inter- and intrarater readings, repositioning, scan/re-scan, and contouring reproducibility have been reported for measures of bone microarchitecture and BMD, erosion and osteophyte characterization, and joint space width (Table 4).
Reproducibility measures.
Intraclass correlation coefficients (ICC) for inter- and intrarater assessments of bone microarchitecture exceeded 0.917, whereas scan/re-scan coefficients of variation (CV) ranged up to 12.5%30,46. The root mean square CV (RMSCV) for contouring reproducibility was < 0.8%27. The RMSCV for BMD measures for intra- and interrater were < 3.3%40, and scan/re-scan and contouring reproducibility were excellent27,30,46. Good interrater agreement for erosion detection and count has been reported by most authors7,11,13,16,24,25. In general, good values for interrater determination of erosion size were obtained, with excellent intrarater ICC9,11,13,33,35,45. There is evidence for variations in joint space width measurements related to repositioning and scan/re-scan26,28,29.
DISCUSSION
This systematic review serves as a comprehensive narrative summary of the available literature on the use of HR-pQCT imaging of the periarticular bone of the MCP or wrists. Despite HR-pQCT being available for only about 10 years, there is considerable literature on its use in imaging of MCP or wrists to describe findings in early inflammatory arthritis, RA, PsA, erosive hand OA, psoriasis, “pre-arthritis,” and healthy controls. The vast majority of studies identified focus on characterizing erosions, with an apparent evolution in case definition standardization but with an ongoing need to standardize and automate methods to measure erosion dimensions. In the evaluation of erosions, other reasons for breaks in the cortical bone such as vessel channels have become apparent, with further studies required to elucidate whether these channels reflect disease pathophysiology or evolve into pathologic states. Other areas of pathology description require further development, such as defining and measuring osteophytes, and achieving consensus on methods for measuring joint space width, along with correlation to tissue studies to confirm findings. At this time standard evaluations have been applied to provide quantitative measures for bone microarchitecture and BMD, although notably the region of interest to be evaluated has varied among authors, either using a set number of slices to be evaluated or a percentage of the metacarpal length to adjust for size.
HR-pQCT is frequently used as the gold standard for erosion detection relative to other imaging modalities including plain radiography, US, and MRI. The high resolution it provides also allows identification of erosive findings in unexpected states, such as in healthy controls, and further work should be directed to refining what is a naturally occurring finding, and how a pathological finding evolves. Although not able to detect soft tissue changes, limiting its abilities relative to US and MRI, HR-pQCT provides microarchitectural detail that those modalities cannot, and is useful in elucidating the evolution of joint damage and even regression of developing lesions35.
Current assessment protocols for quantitative measures exhibit good to excellent reproducibility metrics, whether for direct or derived outcomes, or application of semiquantitative scores. There is evidence that positioning affects quantitative joint space width measures, and there is a need to ensure that a standardized positioning device or protocol be used going forward, in particular for longitudinal studies.
Our review also serves to highlight areas in which data are lacking. Very few reports have assessed the wrist joint, which is a common location for damage in most types of arthritis. Findings have not been described in other systemic inflammatory arthritis conditions such as crystal arthritis, and at a variety of disease stages for RA, PsA, and erosive hand OA. Normative data have been collected infrequently and longitudinal assessments have been rare, and both types of data would further enhance our understanding of the sensitivity of HR-pQCT imaging assessments over time. Of note, a second-generation version HR-pQCT has been released, providing 61 μm of nominal isotropic resolution in contrast to the 82 μm technology that all studies in this review have used. With higher sensitivity imaging available, resolving the determination of the relevance of findings will be important.
HR-pQCT may ultimately prove to be key in the diagnosis of arthritis conditions, and may be used in conjunction with biomarkers or other imaging modalities such as US to more accurately predict patient outcomes. As well, it could be an important tool for the longitudinal monitoring of disease activity and structural bone changes. The sensitivity of the technique may allow detection of small but significant improvements for the purposes of clinical trials for inflammatory diseases. HR-pQCT imaging can be applied in rheumatology outcomes research for the benefit of patients affected by inflammatory joint disease regarding early diagnosis, resulting in initiation of early and appropriate treatment.
APPENDIX 1.
List of study collaborators. SPECTRA Collaboration Members: Cheryl Barnabe, University of Calgary; Susan Barr, University of Calgary; Stephanie Boutroy, Université de Lyon; Steven K. Boyd, University of Calgary; Andrew Burghardt, University of California San Francisco; Roland Chapurlat, Université de Lyon; Angela Cheung, University of Toronto; Joost de Jong, Maastricht University Medical Centre; Klaus Engelke, University of Erlangen; Lynne Feehan, University of British Columbia; Stephanie Finzel, Department of Rheumatology and Clinical Immunology, University Medical Center Freiburg, Faculty of Medicine, University of Freiburg; Piet Geusens, Maastricht University Medical Centre; Ellen-Margrethe Hauge, Aarhus University Hospital; Yebin Jiang, University of Michigan; Kresten Keller, Aarhus University Hospital; Roland Kocijan, University of Vienna; Sebastian Kraus, University of Erlangen; Xiaojuan Li, University of California San Francisco; Hubert Marotte, Université de Lyon; Liam Martin, University of Calgary; Rosa Pereira, University of Sao Paolo; Andrea Scharmga, Maastricht University Medical Centre; Georg Schett, University of Erlangen; Kristian Stengaard-Pedersen, Aarhus University Hospital; Kathryn S. Stok, ETH Zurich; Nikolay Tzaribachev, SCANCO Medical AG; Joop van den Bergh, Maastricht University Medical Centre; Bert van Rietbergen, Eindhoven University of Technology; Astrid van Tubergen, Maastricht University Medical Centre; Mira van Veenendaal, University of Toronto; Paul Willems, Maastricht University Medical Centre; Jeroen Williams, Maastricht University Medical Centre; Rae Yeung, University of Toronto.
APPENDIX 2.
Footnotes
As part of a supplement series from SPECTRA on HR-pQCT, this report was reviewed internally and approved by the Guest Editors for integrity, accuracy, and consistency with scientific and ethical standards.
S. Nagaraj was funded by an Alberta Innovates-Health Solutions Summer Studentship. C. Barnabe is a Canadian Institutes of Health Research New Investigator.








{kind=link}
{kind=link}