Article Text

Abstract
Background: Cyclooxygenase inhibiting nitric oxide donators (CINODs) are a new class of anti-inflammatory and analgesic drugs that may minimise gastrointestinal toxicity compared with standard non-steroidal anti-inflammatory drugs (NSAIDs) by virtue of nitric oxide donation.
Methods: A proof of concept study of the gastrointestinal safety of AZD3582, the first CINOD available for human testing, was conducted. Thirty one subjects were randomised to receive placebo, naproxen 500 mg twice daily, or its nitroxybutyl derivative AZD3582 in an equimolar dose (750 mg twice daily) for 12 days in a double blind three period crossover volunteer study. At the start and end of each dosing period, gastroduodenal injury was assessed by endoscopy and small bowel permeability by differential urinary excretion of lactulose and l-rhamnose. Pharmacokinetic profiles were assessed at steady state.
Results: On naproxen, the mean total number of gastroduodenal erosions was 11.5 (and one subject developed an acute ulcer) versus 4.1 on AZD3582 (p<0.0001). More than half of the subjects had no erosions on AZD3582. Differences were seen for both the stomach and duodenum. Naproxen increased intestinal permeability (lactulose:l-rhamnose ratio 0.030 before v 0.040 after treatment) whereas AZD3582 (0.029 before, 0.029 after; p=0.006 v naproxen) and placebo (0.030 before, 0.028 after; p<0.001 v naproxen) did not. The steady state bioavailability of naproxen metabolised from AZD3582 was 95% (95% confidence interval 87–101%) of that after naproxen administration.
Conclusions: This human study supports animal data showing reduced gastrointestinal toxicity with the CINOD AZD3582. The potential combination of effective pain relief and gastrointestinal protection offered by AZD3582 warrants further evaluation in human clinical studies.
- non-steroidal anti-inflammatory drugs
- nitric oxide
- naproxen
- cyclooxygenase
- CINOD
- stomach
- intestine
- ulcer
- erosion
- CINOD, cyclooxygenase inhibiting nitric oxide donator
- NSAIDs, non-steroidal anti-inflammatory drugs
- COX, cyclooxygenase
- AUC, area under the curve
Statistics from Altmetric.com
- non-steroidal anti-inflammatory drugs
- nitric oxide
- naproxen
- cyclooxygenase
- CINOD
- stomach
- intestine
- ulcer
- erosion
- CINOD, cyclooxygenase inhibiting nitric oxide donator
- NSAIDs, non-steroidal anti-inflammatory drugs
- COX, cyclooxygenase
- AUC, area under the curve
Non-selective non-steroidal anti-inflammatory drugs (NSAIDs) are widely used in the treatment of pain and arthritis but these benefits are counterbalanced by gastrointestinal toxicity which results in substantial morbidity and mortality due to ulcer complications.1,2 This has prompted a search for safer strategies, including cotherapy with misoprostol3 or a proton pump inhibitor4,5 and cyclooxygenase (COX)-2 selective inhibitors.6 All of these approaches have had some success but each also has limitations.
Recognition that nitric oxide can replicate many of the gastroprotective actions of prostaglandins7 has highlighted the possible clinical utility of this molecule. Human epidemiological studies have reported that those using nitrates have fewer ulcer complications than those who do not.8 Nitric oxide may exert its protective effects in the gastroduodenal mucosa by maintaining the defensive mechanisms that are abrogated by COX inhibition, such as mucosal blood flow, and mucus and bicarbonate secretion.7 In addition, nitric oxide decreases neutrophil-endothelial adherence, which is influenced by expression of intercellular cell adhesion molecule 1 and other adhesion molecules and plays an important role in NSAID induced mucosal injury, at least in animal models.9–11
Awareness of the protective effects of nitric oxide has led to the development of a novel class of drugs, the COX inhibiting nitric oxide donators (CINODs).12–14 This new drug class is characterised by a COX inhibiting moiety linked to a nitric oxide moiety. In animal studies, CINODs lead to rises in plasma nitrite/nitrate levels and marked reductions in gastroduodenal and small bowel injury.12,15–19 There is evidence that NSAIDs and COX-2 selective inhibitors can impair healing of established ulcers while CINODs appear capable of accelerating the process in animal models, perhaps via a dominant influence of nitric oxide.13,14 Some animal studies have suggested that the benefits of CINODs may extend beyond the stomach and duodenum to include reductions in intestinal injury and in other organ systems.16,19,20 NSAIDs and COX-2 selective inhibitors cause fluid retention, hypertension, oedema, and heart failure21–24 but increases in blood pressure have not been found with CINODs in animal studies, probably because of a combination of systemic vasodilation, possible enhanced renal blood flow, and altered vascular responsiveness to endogenous pressor agents, including renin and angiotensin.18,25–27 There has been recent speculation that COX-2 selective NSAIDs could promote thrombosis in patients with vascular disease as a result of selective reduction in prostacyclin.28 It is unlikely to occur with CINODs such as AZD3582 [4-(nitrooxy)butyl-(2S)-2-(6-methoxy-2-naphthyl)propanoate] because both COX-1 and COX-2 are inhibited to a large extent and because of the ability of nitric oxide to inhibit platelet aggregation29 and through other mechanisms such as coronary artery vasodilation.
There is some evidence from animal models that COX-1 can contribute to inflammation and that dual COX inhibition may enhance anti-inflammatory potency.30,31 In addition, exogenous nitric oxide could act in an anti-inflammatory way through inhibition of caspase dependent processing of interleukins.32 In rat adjuvant arthritis, AZD3582 has been reported to interfere with T cell activation to a larger extent than naproxen.19 In a rat model of colitis, a nitric oxide donating mesalamine derivative was reported to be a more potent anti-inflammatory agent than mesalamine.33
AZD3582 is the first CINOD to be extensively tested in animals and humans.17,34 It contains naproxen esterified to nitric oxide (fig 1). It has recently been shown to be well absorbed in animals, with pharmacokinetic bioequivalence to naproxen.34 Similar absorption profiles of naproxen have also been demonstrated in single dose studies of AZD3582 and naproxen in humans, and AZD3582 and naproxen have similar molar dose effect relationships on ex vivo COX inhibition (unpublished data). Because CINODs may have potential safety advantages over standard NSAIDs, AZD3582 was evaluated in humans to investigate whether the improved acute gastrointestinal safety profile seen in animals could be replicated.

Structure of AZD3582.
METHODS
Design
A double blind, randomised, three period crossover study was conducted to compare the gastrointestinal safety of placebo, naproxen (500 mg twice daily), and AZD3582 (750 mg twice daily, equimolar with naproxen) over 12 days. The main variables evaluated were the total number of gastroduodenal erosions and ulcers (by endoscopy), small bowel permeability (differential urinary excretion ratio of lactulose and l-rhamnose), steady state pharmacokinetic characteristics, changes in blood pressure, and other safety assessments.
Subjects
Healthy male and female volunteers between the ages of 20 and 65 years of age were recruited. The main exclusion criteria included history of peptic ulceration, NSAID hypersensitivity, and intake of NSAIDs up to three weeks prior to the study. Other exclusion criteria were smoking >10 cigarettes/day or the finding of more than one erosion at any baseline endoscopy. Helicobacter pylori status was defined by serology and urease (CLO) testing.
Conduct of the study
Subjects were studied while receiving each of the three treatments (placebo, naproxen 500 mg twice daily, and AZD3582 750 mg twice daily), on each occasion. Subjects were randomised with equal probability to one of the six possible orders of treatments. There was a 14 day washout period between each treatment regimen. Prior to administration of the first dose, subjects were admitted to the Clinical Investigation Unit of the Division of Gastroenterology, University Hospital, Nottingham, for assessment of small intestinal permeability. Endoscopy was performed on the following day before administering the first of 23 twice daily doses of the study drug. Doses were given at approximately 07.00 h and 19.00 h each day. On the penultimate day of the treatment period (that is, after 11 days), subjects returned for further assessment of intestinal permeability and for samples to be taken for steady state pharmacokinetic evaluations (described below). On the next (12th and final) day of each treatment period, they underwent endoscopy, 90 minutes after the final dose of drug.
Steady state pharmacokinetic evaluation
Blood samples were collected on the penultimate dosing day of every treatment period, ⩽10 minutes before and 1.5, 2.5, 4, and 6 hours after drug administration. After separation of plasma, levels of naproxen and AZD3582 were measured by high performance liquid chromatography. Pharmacokinetic calculations were performed by means of a non-compartmental analysis using WinNonlin (Pharsight Corporation, Mountain View, USA). The low and varying plasma concentrations of AZD3582 did not enable full pharmacokinetic evaluation. For calculation of the naproxen area under the curve (AUC) during a 12 hour dosing interval at steady state (AUCss), it was assumed that plasma concentrations at 12 hours and pre-dose (Css,min) were equal. The relative steady state bioavailability of naproxen was calculated from the ratio of naproxen AUCss values after AZD3582 and naproxen administrations.
Endoscopy
Following an overnight fast, endoscopy was performed unsedated in the morning, immediately before the start of each treatment and 90 minutes after the final dose on day 12. Erosions, ulcers, and petechiae were recorded separately for the oesophagus, stomach, and duodenum. Ulcers were defined as breaks in the mucosa with a depth ⩾3 mm in diameter. Erosion and ulcer counts were used to derive a score on the modified Lanza injury scale (0, normal mucosa; 1, erythema (petechiae) only; 2, 1–5 erosions; 3, 6–10 erosions; and 4, >10 erosions or an acute ulcer).35
Intestinal permeability
For assessment of intestinal permeability, subjects drank 100 ml of test solution containing 0.2 g of 3-O-methyl-desoxy-glucose, 0.5 g of d-xylose, 1.0 g of l-rhamnose, and 5.0 g of lactulose at 08.00 h following an eight hour fast (60 minutes after the morning dose of study drug for the on-treatment measurement on day 11). All urine excreted over five hours was collected for determination of sugars by thin layer chromatography combined with scanning densitometry. This analytical method is accurate (recovery >90%), sensitive (minimum level of detection <1 mg/100 ml), and precise (coefficient of variation 2–8%). The ratio of lactulose to l-rhamnose (% dose) was used as an index of intestinal permeability.36
Safety data
Safety and tolerability data, including physical examination, blood pressure/pulse rate (supine and after five minutes of standing), 12 lead ECG, and standard clinical chemistry and haematology were assessed at baseline on the penultimate day of each dosing period and 4–10 days after the last dose. The on-treatment assessments of blood pressure/pulse rate and 12 lead ECG were done three hours after dosing, which is approximately at the predicted Cmax for AZD3582 and naproxen. Spontaneous adverse event reports were collected throughout the study and categorised according to WHO adverse reaction terminology.
Statistical analysis
Thirty subjects were chosen in order for the sign test to have at least 80% power to detect a difference between AZD3582 and naproxen assuming that the distributions of the Lanza scores were 40%, 11%, 27%, 20%, and 2% for AZD3582, and 11%, 6%, 25%, 44%, and 14% for naproxen. The main analyses concerned non-parametric pairwise comparisons for naproxen versus AZD3582, and for naproxen versus placebo based on the sign test adjusted for period effects with two tailed alpha levels of 0.05. For pharmacokinetic analyses, log [naproxen, AUC0–12h at steady state] (AUCss), log [naproxen Cmax at steady state] (Css,max), log [naproxen Cmin at steady state] (Css,min), and tmax were modelled as dependent variables with subject, period, and treatment as independent variables. Safety data were assessed descriptively, without formal statistical comparisons. In general, data are given as means (SD) for continuous variables and medians and interquartile ranges (IQR) for categorical variables.
RESULTS
Subjects
Thirty six subjects were screened, of whom 31 met entry criteria and agreed to enter the study. Twenty eight were male and 26 were H pylori negative. Median age was 32.4 (range 22.0–56.9) years. Two subjects withdrew from the study after the first treatment period (naproxen in one case and placebo in the other). Two withdrew after two study periods (both after receiving both AZD3582 and naproxen). The reasons were withdrawal of consent,2 lost to follow up,1 and persistent mucosal injury at the following baseline endoscopy (after naproxen). Thus 29 subjects completed the naproxen treatment period, 29 finished the AZD3582 treatment period, 29 completed the placebo treatment period, 28 subjects completed AZD3582 and naproxen, and 27 subjects completed all treatment periods. Gastrointestinal data were analysed for all available paired drug comparisons. Safety data were analysed for all subjects receiving treatment.
Pharmacokinetics
Table 1 shows steady state pharmacokinetic parameters at the end of the naproxen and AZD3582 regimens. The overall bioavailability of total naproxen metabolised from AZD3582 was 95% (95% confidence interval 87–101%) of that following naproxen dosing, well within the standard bioequivalence range. Css,max was lower for naproxen metabolised from AZD3582 but Css,min values were similar. The tmax was slightly longer after AZD3582 administration. Plasma levels of AZD3582 were in the lower nmol/l range and varying, and were quantifiable up to six hours or shorter (table 1).
Steady state pharmacokinetic parameters following oral administration of naproxen (500 mg twice daily) and AZD3582 (750 mg twice daily)
Gastroduodenal injury
There were no differences in the mean total number of erosions at baseline before each of the three treatments. No change from baseline in the mean total number of erosions was seen during placebo treatment (mean (SD) 0.2 (0.7) at baseline, 0.2 (0.5) at 12 days). For patients on naproxen, the mean total number of erosions increased from 0.03 (0.19) to 11.5 (10.6) at 12 days (fig 2) and one subject developed an acute duodenal ulcer.
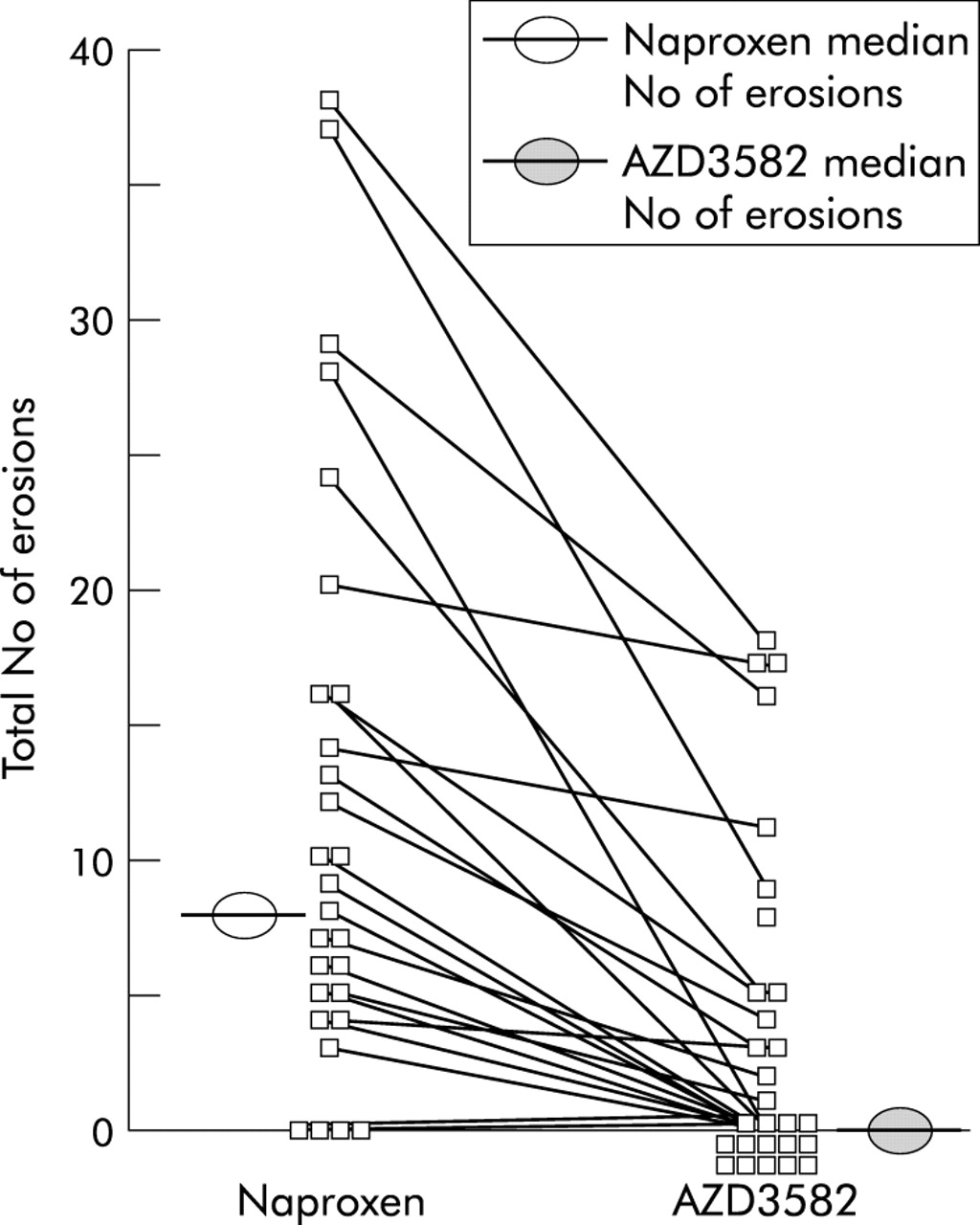
Total number of erosions in the stomach and duodenum following oral administration of naproxen (500 mg twice daily) and AZD3582 (750 mg twice daily). Medians and results for individual subjects are shown.
The mean total number of erosions at baseline for AZD3582 recipients was 0.1 (0.5) at baseline and 4.1 (6.1) on day 12 (p<0.0001 compared with naproxen). No subject on AZD3582 or placebo developed an ulcer. Most erosions with naproxen and AZD3582 were in the stomach. The difference in the mean number of erosions between AZD3582 and naproxen was significant for the stomach (3.2 (5.1) v 8.8 (9.2); p=0.007) and duodenum (0.9 (2.2) v 2.7 (3.7); p=0.0023) and the significant difference between the two agents was maintained when injury was scored using the modified Lanza scale (median 1 (IQR 0–2) v 2 (2–3); p=0.007).
Intestinal permeability
There were no changes in intestinal permeability during placebo or AZD3582 treatment. Naproxen caused a significant rise in small intestinal permeability ratio (mean (SD)) from 0.030 (0.022) to 0.040 (0.021) (fig 3). On-treatment values for both AZD3582 (0.029 (0.014)) and placebo (0.028 (0.015)) were significantly less than for naproxen (p=0.006 and p=0.001 respectively) (fig 3).

Intestinal permeability, measured as lactulose/l-rhamnose ratio. Means and 95% confidence intervals are given. **p=0.006, ***p=0.001 versus naproxen.
Cardiovascular parameters
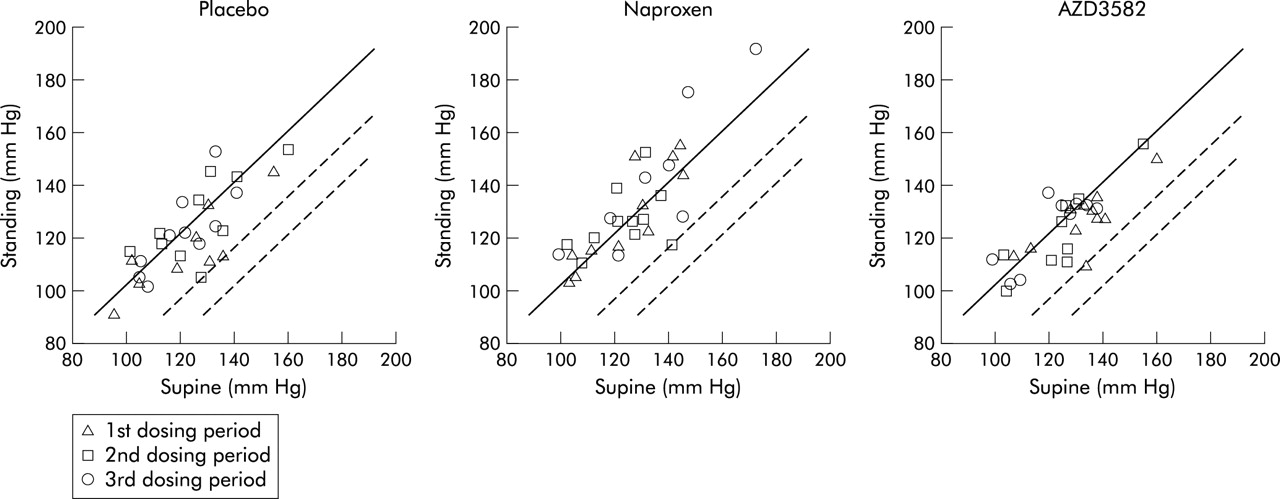
Mean (SD) lying systolic pressure on treatment was 124 (16) mm Hg on placebo, 129 (17) mm Hg on naproxen, and 127 (15) mm Hg on AZD3582 compared with 130 (16)/70 (9) mm Hg at baseline. Values for diastolic blood pressure were 69 (10) mm Hg on placebo, 69 (11) mm Hg on naproxen, and 68 (9) mm Hg on AZD3582. The number of systolic readings of ⩾140 mm Hg and/or diastolic readings ⩾90 mm Hg at the end of each dosing period were four on placebo, 10 on naproxen, and three on AZD3582. A statistical test of these differences was not pre-specified and was therefore not done. The orthostatic effect on blood pressure was similar for the different treatments and study periods and there was no postural hypotension with any treatment (fig 4). No significant changes in ECG configuration or conduction times were seen with any treatment.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Standing and lying systolic blood pressure following oral administration of placebo, naproxen (500 mg twice daily), and AZD3582 (750 mg twice daily). Continuous line shows equality between standing and lying pressures. The two broken lines show falls of 25 and 40 mm Hg in standing compared with lying systolic blood pressure.
Adverse events and safety data
There were no serious adverse events. In total, 33 different adverse events were reported. Fourteen were on AZD3582, 13 on placebo, and six on naproxen. There was no obvious pattern of adverse events. There were five adverse events with placebo that affected the gastrointestinal system, six with naproxen, and five with AZD3582 (dyspepsia n=1; abdominal pain n=2; nausea n=1; and diarrhoea n=1). There were no differences between any of the treatments with regard to the major laboratory variables assessed.
DISCUSSION
In this study, we compared doses of the CINOD AZD3582 and the non-selective NSAID naproxen at molar equivalent doses. The oral bioavailability of the active principal naproxen was similar, which is consistent with previous human data showing similar inhibition of COX-1 (98% with AZD 3582 v 97% with naproxen) and COX-2 (86% v 85%, unpublished data). We found that AZD3582 was associated with significantly less acute gastrointestinal toxicity that naproxen. Differences between AZD3582 and naproxen were seen both for erosive gastroduodenal damage in both the stomach and duodenum, and for a well validated measure of small intestinal damage. These potentially important advantages were not associated with postural hypotension, which could theoretically occur if excessive nitric oxide were released. In these respects, our data in humans are qualitatively similar to those reported in rats.17,18
Our data represent the first human proof of concept evaluation of the gastrointestinal effects of a CINOD. They are likely to be broadly reflected in improved clinical outcomes: although the significance of erosions has been debated, and they are unlikely to be intrinsically harmful, what evidence there is suggests that erosions are broadly predictive of endoscopic ulcers and of perforations, ulcers, and bleeds.37 Moreover, protective strategies tested hitherto have given qualitatively similar results in acute endoscopic and long term endoscopic and outcome studies.38 Likewise, there is good evidence that NSAID induced increases in small intestinal permeability are a prerequisite for the development of NSAID enteropathy,1,39 seen in 50–70% of patients on long term treatment.39 All NSAIDs that cause enteropathy are associated with increased intestinal permeability in the short term in humans and in experimental animals while those that do not increase intestinal permeability are not.39 It is therefore likely that the lack of AZD3582 induced increased intestinal permeability in the short term will be translated into tolerability when taken long term.
Nevertheless, there is some debate over the significance of short term endoscopy studies as quantitative prediction has not been established and additional factors may influence longer term clinically important outcomes,38 making acute models generally rather than quantitatively predictive. When protective cotherapy strategies, with misoprostol or proton pump inhibitors, have been employed in acute models, there has usually been some residual injury,40–43 in contrast with COX-2 selective inhibitors, while in longer term studies both approaches achieve a fourfold reduction in endoscopic ulcers.5,44 Moreover, protective cotherapy45 achieves reductions in ulcer complications that are at least as great as seen with COX- 2 inhibitors, although there are no direct comparisons. Some acute gastroduodenal injury was observed with AZD3582, where nitric oxide donation represents a protective principle, but it was of a magnitude similar to that reported for cotherapy of misoprostol or proton pump inhibitors with non-selective NSAIDs.40–43 Differences in study protocols mean that the relative levels of acute gastrointestinal injury with AZD3582 compared with COX-2 selective inhibitors and with coprescription of mucosally protective drugs with NSAIDs can only be determined by direct study. Similarly, appropriate future direct comparisons would be needed to identify the comparative long term gastrointestinal outcomes of these three strategies.
The reduced small intestinal toxicity with AZD3582 compared with naproxen may well translate into overall clinical benefit, and AZD3582 may have other advantageous properties over COX-2 selective inhibitors. There is mounting evidence that dual inhibition of the two COX enzymes is detrimental to gastrointestinal integrity19,46 and the donation of nitric oxide8 by AZD3582 has the potential to protect against gastrointestinal damage by coprescribed aspirin. CINODs such as AZD3582 could also protect against thrombosis via both COX-1 inhibition and the effects of nitric oxide.29 Animal studies suggest that AZD3582 and other CINODs do not appear to cause hypertension,18,25 unlike standard NSAIDs and COX-2 selective inhibitors,21–24 and AZD3582 did not cause postural hypotension in this study. All or some of these differences, such as relative efficacy, remain to be established clinically by direct comparison with NSAIDs.
How CINODs result in less mucosal injury in animals is not fully determined. Nitric oxide stimulates gastric mucosal blood flow and enhances secretion and bicarbonate, all of which are fundamental protective mechanisms shared with prostaglandins. Animal studies also suggest that neutrophil abrogation and endothelial adherence with consequent vascular congestion may contribute to acute injury; whether this occurs in humans is not known. Nitric oxide can also abrogate this potential mechanism of disease. The results of our study mean that a mechanistic evaluation of AZD3582 in humans will be needed. AZD3582 is metabolised to some extent in human gastrointestinal fluid. On the basis of pharmacokinetic, stability, and permeability data for AZD3582 and naproxen, it has been calculated that at least 15–20% of AZD3582 is absorbed intact and the remaining part is hydrolysed to naproxen in the gastrointestinal tract (unpublished data). AZD3582 undergoes extensive first pass metabolism in animals,34 and this is apparent also in this study in humans. This makes it likely that sufficient local release of nitric oxide occurs to achieve protection. The tendency to a delay to peak plasma concentrations of naproxen could be explained by lower permeability of AZD3582, slower dissolution of the AZD3582 formulation, and/or by the time taken for AZD3582 to be metabolised to naproxen. However, an altered pattern of drug exposure, with a delayed rise to a reduced peak plasma concentration, is unlikely to explain the reduction in gastrointestinal injury as extended release preparations of NSAIDs are associated with equal or greater mucosal injury and ulcer complications compared with immediate release preparations.6,47
Our data suggest that AZD3582 has the potential to be a clinically beneficial drug with an improved gastrointestinal safety profile compared with naproxen. Consequently, clinical trials are underway to assess their role in the management of pain and arthritis by direct patient based comparisons.
Acknowledgments
We thank Miss Laura Garratt for her assistance in the production of this manuscript.
The study was initially conceived and designed by Chris Hawkey, Bror Jonzon, and Ingvar Bjarnason and the protocol developed additionally with John Jones and Clare Atherton and refined by Maeve Skelly and James Bebb. Clare Atherton organised the conduct of the study with the endoscopies done by John Jones, Maeve Skelly, and James Bebb. Ingvar Bjarnason analysed the permeability samples. Urban Fagerholm performed the pharmacokinetic analyses, Par Karlsson the statistical analysis and, together with Bror Jonzon, they completed the first study report. Chris Hawkey drafted the paper and developed it to a final draft with the other authors.