Article Text

Abstract
Aim To evaluate the efficacy of infliximab treatment in patients with refractory uveoretinitis associated with Behçet's disease.
Methods Clinical records of 14 patients were retrospectively reviewed. Patients received infliximab infusions (5 mg/kg) at weeks 0, 2 and 6, and every 8 weeks thereafter. The main outcome measures were frequency of clinically observable ocular inflammatory attacks, background retinal and disc vascular leakage as assessed by fluorescein angiography during periods of clinical quiescence, visual acuity and adverse effects.
Results The median follow-up after initiating infliximab therapy was 19 months (range 12–29 months). At 12 months, eight of 14 patients (57%) had experienced no inflammatory attacks, and the frequency of attacks was significantly reduced when compared with the 6-month period just prior to infliximab use. Background retinal and disc vascular leakage assessed at 12 months improved in 11 of 14 patients (79%). Visual acuity improved or remained unchanged at 12 months in 26 of 28 eyes (93%). Infliximab therapy was terminated in two patients owing to infusion reactions. However, no serious adverse effects were observed.
Conclusion Infliximab over the first year of treatment appeared effective in reducing ocular inflammatory attacks, as well as background retinal and disc vascular leakage, in patients with refractory uveoretinitis associated with Behçet's disease.
- Behçet's disease
- infliximab
- treatment
- retinal vasculitis
- fluorescein angiography
- choroid
- retina
- inflammation
- treatment medical
Statistics from Altmetric.com
- Behçet's disease
- infliximab
- treatment
- retinal vasculitis
- fluorescein angiography
- choroid
- retina
- inflammation
- treatment medical
Introduction
Behçet's disease is a multisystem inflammatory disorder with a chronic and relapsing course.1–3 The four major clinical manifestations are intraocular inflammation, recurrent oral aphthous ulcers, genital ulcers and skin lesions.1–3 Patients with ocular involvement usually have unilateral or bilateral acute episodes of anterior uveitis with or without hypopyon, posterior uveitis and/or panuveitis.1–3 The disease eventually affects both eyes in the majority of cases, and is believed to be particularly severe in young men.4 The frequency and severity of ocular attacks determine the extent of damage to intraocular structures and ultimately visual prognosis.5 6 However, continuous background retinal and disc vascular leakage is well documented, even during periods of clinical quiescence,7 and such ‘background inflammation’ may also contribute to slow destruction of ocular tissues and decline in vision. To our knowledge, the effect of treatment on such retinal and disc vascular leakage in Behçet's disease has never been reported.
Until recently, the treatment of Behçet's disease was based on a strategy of inducing immunosuppression using drugs such as corticosteroids and ciclosporin, thereby inhibiting the pathways of the immune system in a broad and rather non-specific manner.8 New agents such as infliximab, an antitumour necrosis factor α antibody, have demonstrated their effectiveness in the treatment of rheumatoid arthritis and Crohn's disease.9 Recently, open-label clinical trials in Japan and Turkey have shown infliximab to be effective also in Behçet's disease in terms of reducing ocular inflammatory attacks, although no analysis of background retinal and disc vascular leakage was carried out in these studies.10 11
The overall aim of this retrospective study was to evaluate efficacy and safety of infliximab in ocular Behçet's disease over the first year of treatment. Efficacy was assessed, not only by the number of clear clinically observable ocular inflammatory attacks but also by the degree of background retinal and disc vascular leakage as observed by fluorescein angiography.
Methods
Patients
Medical records were reviewed of 14 patients with Behçet's disease followed in the Ocular Inflammation Service at the Kyorin Eye Center, Kyorin University Hospital (Tokyo, Japan) who received infliximab therapy for at least 6 months between January 2007 and December 2009. Eight patients met the International Study Group criteria for Behçet's disease, while six patients were diagnosed based on the criteria of the Behçet's Disease Research Committee of Japan.12 13 As per Japanese Ministry of Health, Labour, and Welfare (MHLW) guidelines concerning the indication for infliximab therapy, all 14 patients had ocular inflammation refractory to treatment with at least one immunosuppressive drug and/or corticosteroids, or were judged to be intolerant to such therapy owing to adverse effects.
Treatment protocol
Before starting infliximab, all patients underwent a complete internal medical examination, tuberculin protein purified derivative (PPD) skin testing and chest x-ray examination. Patients found to be PPD-positive received tuberculosis prophylaxis consisting of 400 mg/day of isoniazid for 9 months. The treatment protocol as per MHLW guidelines involved intravenous infusions of infliximab at a dose of 5 mg/kg at weeks 0, 2 and 6, and every 8 weeks thereafter. In patients receiving ciclosporin at the time of initiating infliximab therapy, the ciclosporin was tapered down to a lower dose and then maintained in an attempt to inhibit the development of human antichimera antibodies.14 15 All other immunosuppressive agents were tapered, with the goal of eventual discontinuation.
Main outcome measures
The main outcome measures were the number of clinically observable ocular inflammatory attacks, background retinal and disc vascular leakage as assessed by fluorescein angiography during periods of clinical quiescence, visual acuity and adverse effects.
Anterior chamber cells and flare were graded as per the SUN Working Group.16 Ocular inflammatory attacks were defined as the sudden onset of cells and/or flare in the anterior chamber or vitreous, or cellular infiltrates and/or haemorrhage in the retina, as assessed clinically by slit-lamp biomicroscopy and funduscopy. The number of ocular attacks before and after initiating infliximab treatment was converted to frequency per 6-month period. To assess the degree of background retinal and disc vascular leakage, fluorescein angiography (FA) was performed prior to initiation of infliximab therapy (baseline) and at 12 months, at times of clinical quiescence defined as the absence of signs of an ocular inflammatory attack. FA was also performed at 24 months in five patients. The extent of fluorescein leakage was graded on a scale of 0 to 3 (0=none, 1=mild, 2=moderate, 3=severe) for the peripheral retina, the macula and the optic disc. Two ophthalmologists (HK and AO) performed the FA grading in a masked fashion. The mean scores were calculated for the peripheral retina, macula and optic disc separately, with the total vascular leakage score representing the sum of these three mean scores.
Best-corrected visual acuities were measured at each clinic visit. Adverse events including infusion reactions (occurring during and up until 2 h after conclusion of the infliximab infusion) were recorded. This study was conducted in accordance with the tenets of the Declaration of Helsinki and was deemed by the Kyorin University Hospital Research Ethics Committee not to require institutional review board approval.
Statistical analysis
Statistical analysis was performed using the Wilcoxon signed-rank test. A p value of <0.05 was considered to indicate statistical significance. All results were expressed as mean±SE.
Results
The demographic characteristics of the 14 Behçet's disease patients who received infliximab are summarised in table 1. Twelve patients were men, and two were women, with ages ranging from 13 to 68 years (mean 38 years). The median duration of intraocular inflammation associated with Behçet's disease prior to starting infliximab therapy was 30 months. Manifestations or history of oral aphthous ulcers, skin lesions and genital ulcers were noted in 14, six and four patients, respectively. One patient had also been diagnosed as having neurological manifestations of Behçet's disease. Twelve of the 14 patients were receiving ciclosporin at the time of initiating infliximab therapy, and the ciclosporin was tapered down in nine patients. At 12 months on infliximab, seven patients were receiving a ciclosporin dose of 100 mg/day or less. Six of the 14 patients were receiving oral corticosteroids in addition to ciclosporin at the initiation of infliximab therapy, and the corticosteroid was tapered to a dose of 10 mg/day or less in five of six patients and discontinued in two patients. Two patients were receiving methotrexate in addition to ciclosporin and corticosteroids at the initiation of infliximab therapy, and the methotrexate was continued at a dose of 8 mg/wk in one patient for neurological manitfestations and discontinued in the other patient.
Baseline patient demographics and clinical manifestations
The median follow-up after initiating infliximab therapy was 19 months (range 12–29 months). Eight of 14 patients (57%) had no ocular inflammatory attacks over the first 12 months. Two of five patients examined after 24 months on infliximab also had no clinically observable ocular attacks. As shown in figure 1A, the mean frequency of ocular attacks before infliximab treatment was significantly reduced during the first 6 months of infliximab administration. However, over subsequent 6-month periods, this mean frequency of ocular attacks gradually rose. Of note, infliximab treatment was terminated owing to severe infusion reactions in two patients at 6 and 12 months of initiating therapy. As shown in figure 1B, when these two patients were excluded from the data, the mean numbers of ocular attacks per 6-month period were significantly reduced at 6, 12 and 18 months after initiating therapy. Concomitant drugs were reduced or discontinued in 10 of the 12 patients who were able to continue infliximab therapy.

Frequency of ocular inflammatory attacks before and after initiation of infliximab treatment. (A) Number of ocular inflammatory attacks before and after initiation of infliximab treatment, converted to the frequency per 6-month period, with the mean±SE shown for each period. (B) Mean number of ocular inflammatory attacks (±SE) before and after initiation of infliximab treatment, shown after excluding data from two patients in whom infliximab therapy was terminated due to severe infusion reactions. A statistical analysis was performed using the Wilcoxon signed-rank test. *p<0.01 versus baseline. **p<0.05 versus baseline.
Six patients had ocular attacks during the first 12 months after initiating infliximab therapy (figure 2). Patients 4 and 5 developed ocular attacks at various time points after the last infliximab infusion, although these were the two patients mentioned above who experienced infusion reactions leading to discontinuation of infliximab treatment. Thereafter, patient 4 moved to a different city, where he was reportedly restarted on infliximab. In patient 5, the dose of concomitant ciclosporin was increased with moderate control of ocular recurrences.

Timing of recurrence of ocular attacks from the last infliximab infusion. The interval between the last infusion of infliximab and recurrence of ocular attacks was analysed. Six patients had recurrence of ocular attacks during 12 months. In four patients (patients 2, 6, 7 and 11), recurrence occurred 7 or 8 weeks after the last infliximab infusion. Patients 4 and 5 developed recurrence at various time points. Arrows indicate the occurrence of ocular attacks. Open arrows indicate bilateral ocular attacks. The numbers shown in the figure indicate the exact time point after infliximab treatment in the 8-week interval between infliximab infusions.
The remaining four patients who had ocular attacks experienced them at weeks 7 to 8 after the last infliximab infusion. These consisted of asymptomatic small cellular infiltrates in the peripheral retina with no decrease in visual acuity in patients 2, 6 and 11, for which additional treatments were not performed. In patient 7, mildly symptomatic anterior chamber cells were noted at week 8, for which topical corticosteroids were prescribed and quickly tapered. The interval between infliximab infusions was not shortened in these four patients.
One patient, a 38-year-old man, was also diagnosed as having neuro-Behçet's disease based on symptoms of leg weakness and urinary retention, with corresponding parenchymal abnormalities on brain MRI and cerebrospinal fluid pleocytosis. This patient had no neurological or ocular inflammatory recurrences over the first 24 months of infliximab.
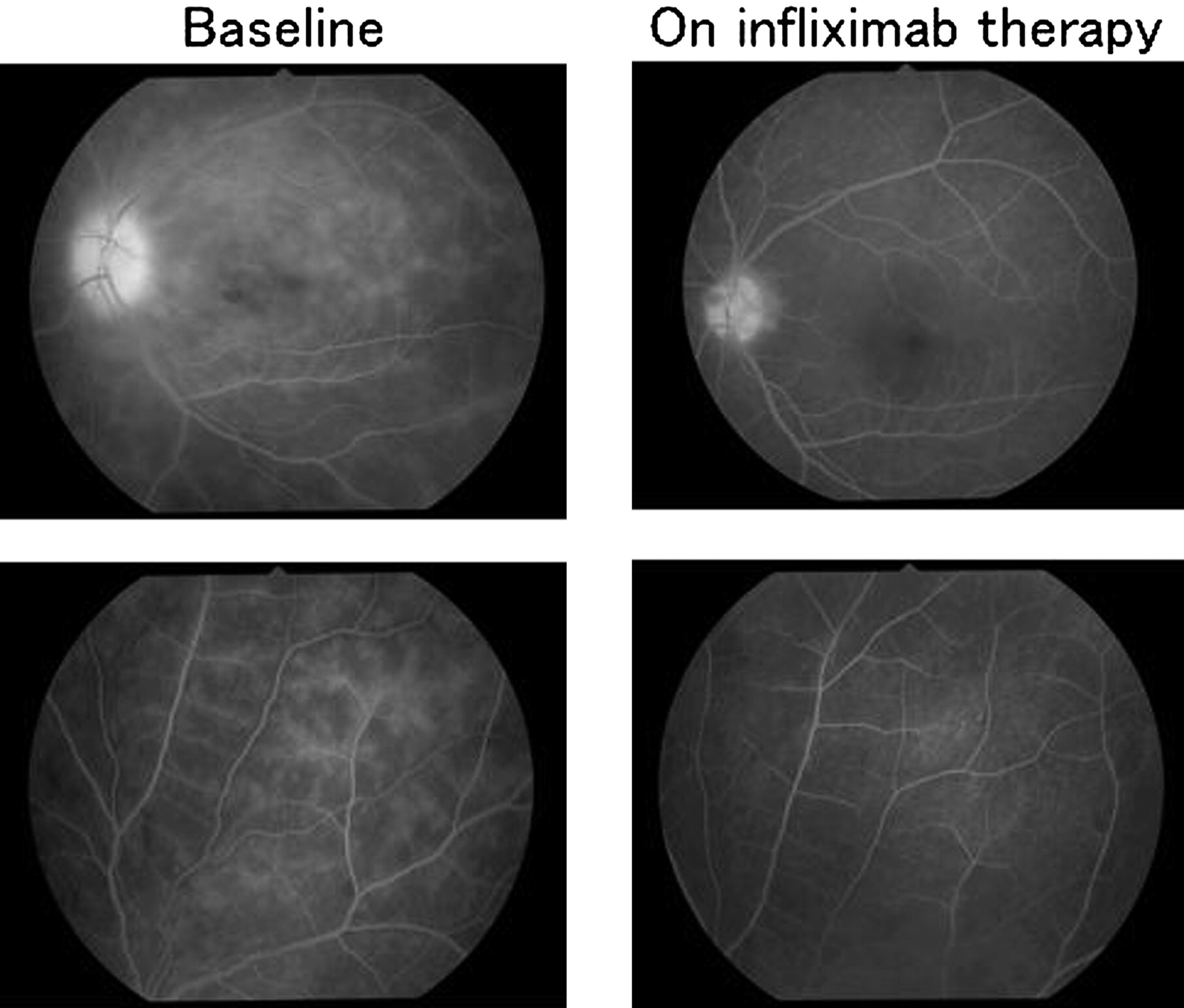
Figure 3A shows the mean grade of retinal vascular leakage as assessed by FA at baseline before initiating infliximab therapy and at 12 months of therapy. There was a significant decrease in the total vascular leakage score with infliximab treatment (p=0.0338). The score was reduced for peripheral retina, macula and optic disc, although the difference was statistically significant only for peripheral retina. As shown in figure 3B, the total vascular leakage score on infliximab decreased in 11 of 14 patients (79%). The two patients in whom infliximab therapy had been terminated owing to severe infusion reactions (patients 4 and 5) represented two of the three patients in whom no improvement in total vascular leakage score was noted. Figure 4 shows representative FA images (patient 2), showing decreased peripheral retina and disc vascular leakage at 21 months after initiation of infliximab therapy.

Improvement in retinal vasculitis after infliximab infusions. (A) Fluorescein angiography (FA), performed at times of clinical quiescence prior to initiation of infliximab treatment (baseline) and at 12 months to assess the degree of vascular leakage. The extent of fluorescein leakage was graded on a scale of 0 to 3 (0=none, 1=mild, 2=moderate, 3=severe) for the peripheral retina, the macula and the optic disc. The data represent means±SEM within each group. A statistical analysis was performed using the Wilcoxon signed-rank test. (B) Total vascular leakage score, calculated for each individual patient, with the black bar indicating the score at baseline and the white bar indicating the score at 12 months.
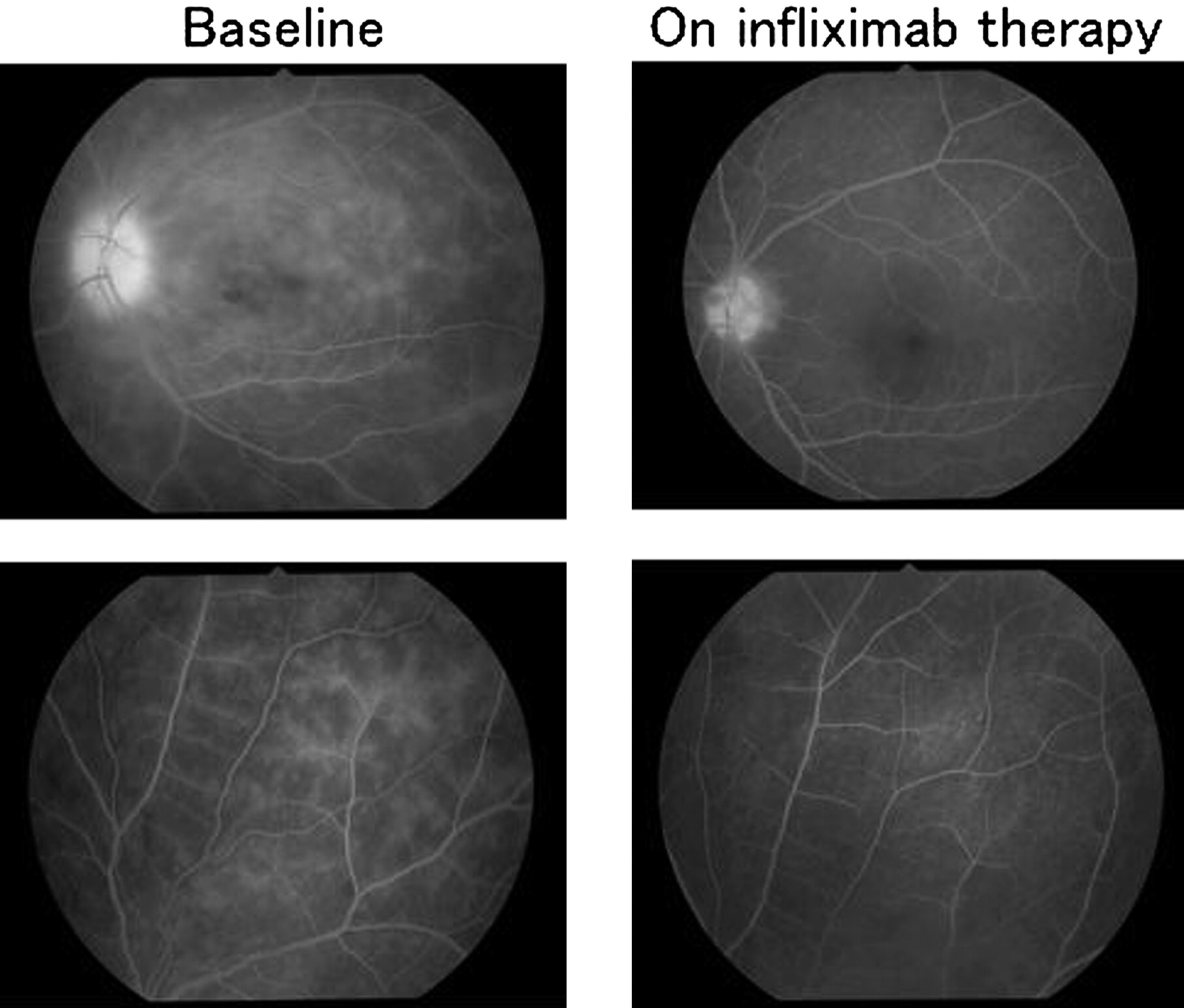
Fluorescein angiographic images of a representative Behçet's disease patient at baseline and on infliximab therapy. Fluorescein angiographic images of the left eye of patient 2 at baseline and at 21 months after initiation of infliximab treatment during times of clinical quiescence. Fluorescein leakage from vessels in the macula, the peripheral retina and the optic disc were observed before infliximab treatment (left upper and lower images). This fluorescein leakage showed an improvement on infliximab therapy (right upper and lower images).
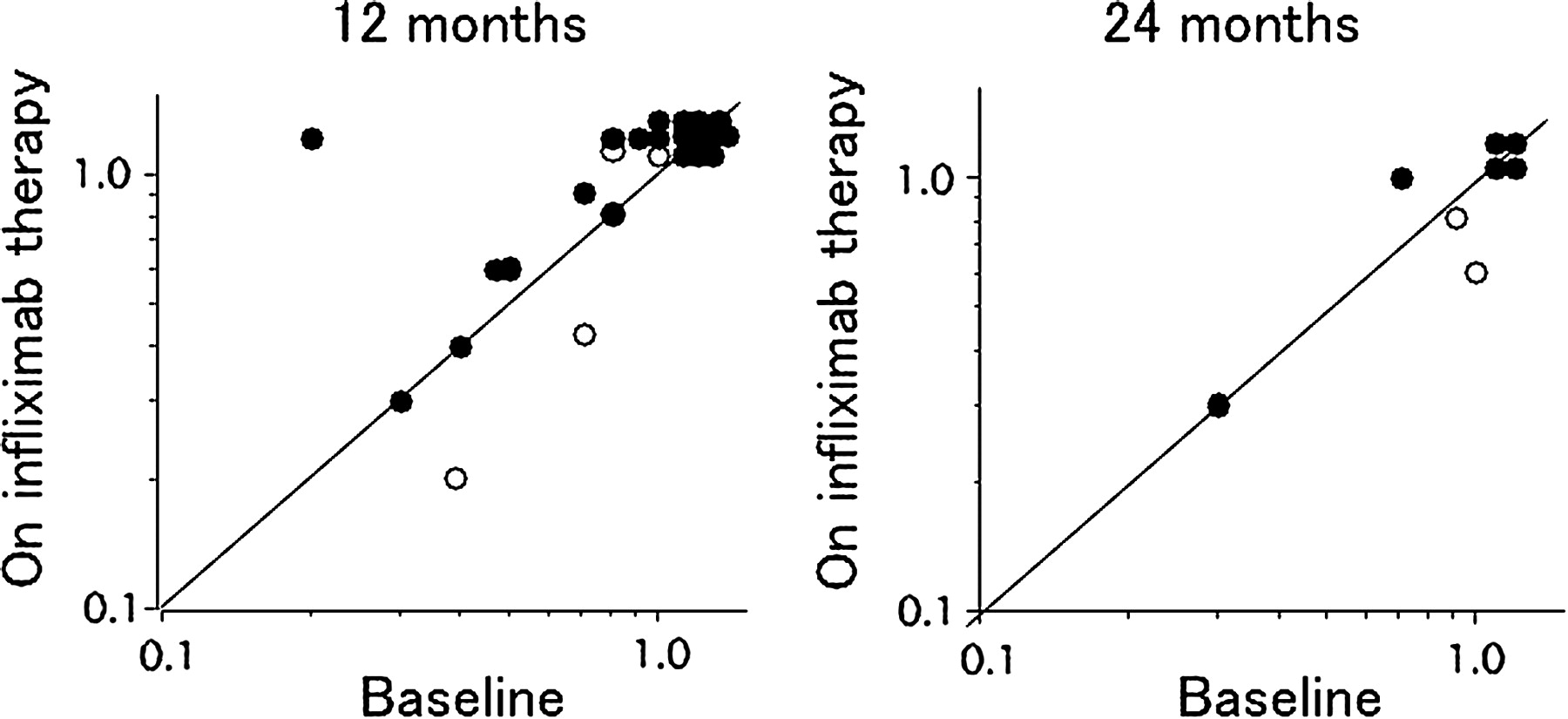
As shown in table 2, the percentage of patients with a best-corrected visual acuity (BCVA) of 1.0 or better rose from 46% at baseline to 61% at 12 months. Three eyes (10%) with a BCVA of 0.1 or less at baseline experienced no improvement in visual acuity, although these eyes had optic disc atrophy and/or macular atrophy prior to the initiation of infliximab therapy. The BCVAs before and after initiating infliximab treatment are shown in figure 5. The BCVA was maintained or improved in 26 of 28 eyes (92.8%) at 12 months, and in eight of 10 eyes (80%) at 24 months. The two eyes that had a decrease in BCVA at 12 months were from patient 4, who discontinued infliximab therapy (at 6 months) owing to severe infusion reactions; this patient subsequently moved to another city after 22 months of follow-up. A further two eyes had a decrease in BCVA at 24 months; these belonged to patient 5, who also had to discontinue infliximab therapy (at 12 months) owing to severe infusion reactions.
Best-corrected visual acuities in Behçet's disease patients treated with infliximab (number of eyes)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Visual acuities at baseline and on infliximab therapy. Best-corrected visual acuities of all study eyes are shown at baseline and at 12 months (n=14) and 24 months (n=5) after initiation of infliximab administration. The closed circles represent the 12 patients who received infliximab treatment for over 1 year. The open circles represent the two patients who discontinued infliximab treatment due to infusion reactions at 6 and 12 months, respectively.
With regard to adverse effects, five patients experienced symptoms consistent with the common cold; all these patients recovered without specific treatment. One patient had suspected bacterial pharyngitis that responded to antibiotic therapy.
Four patients experienced infliximab-related infusion reactions consisting of rash, itchiness and/or respiratory distress. These infusion reactions occurred at the fifth infusion in two patients, the eighth infusion in one patient, and the 15th infusion in one patient. All four of these patients had been receiving concomitant ciclosporin. After the initial infusion reaction, subsequent infusions were performed with preadministration of intravenous hydrocortisone (100 mg), and the infusion reactions abated in two patients. However, infusion reactions continued in the remaining two patients with increasing severity, and infliximab therapy was discontinued as mentioned previously at 6 and 12 months. The dose of concomitant ciclosporin was subsequently increased to 250 mg/d in patient 5 in whom infliximab therapy was terminated at 12 months; no increase in ocular inflammatory attacks has been observed in this patient over a 24-month period since stopping infliximab.
Discussion
In our hands, infliximab therapy significantly reduced the frequency of ocular inflammatory attacks in 12 of 14 Behçet's disease patients, with eight patients experiencing no attacks whatsoever over the first 12 months of therapy. Furthermore, on infliximab, we were able to reduce the concomitant immunosuppressive regimen in 10 of 12 patients. These results suggest that in Behçet's disease patients who are treated continually with infliximab therapy, ocular inflammatory attacks are markedly suppressed with successful tapering or discontinuation of immunosuppressive drugs in the majority of patients. These results are in line with previous reports, indicating that infliximab is effective for suppressing ocular attacks in Behçet's disease.10 11 17 18 In addition, the frequency of ocular inflammatory attacks was found not to rise with time in patients who were able to continue successfully with infliximab therapy (figure 1B).
The ocular attacks while on infliximab we observed were mild and occurred just prior to the next infliximab infusion in most cases, similar to the experience of other clinicians.19 The serum infliximab concentration in these patients may have dropped to lower than a certain threshold necessary for control of ocular disease.20 However, in our study, two patients developed recurrences at various time points regardless of their infusion schedule. In these patients, ocular recurrence may have been related to inadequate infliximab dosing owing to the development of infusion reactions.
We also investigated whether infliximab therapy would affect the degree of background retinal and optic disc vascular leakage as assessed by fluorescein angiography at times of clinical quiescence. It is well known that retinal and optic disc atrophy are major causes of morbidity in Behçet's disease,21 22 and we suspect that damage to these intraocular structures occurs not only because of acute inflammatory attacks, but also because of chronic smoldering inflammation as evidenced by background vascular leakage. In our study, we found that infliximab significantly reduced vascular leakage in the peripheral retina at 12 months of therapy. In addition, vascular leakage in the macula and at the optic disc also improved, although this was not statistically significant. Suppression of such chronic vascular leakage, whether via infliximab therapy or other treatments, would be expected to aid in the preservation of tissue function and therefore ultimately visual function. Furthermore, vascular leakage on FA may serve as an important surrogate marker for the degree of inflammatory control for Behçet's disease patients on various drug regimens.
In the present study, the percentage of eyes with a BCVA of 1.0 or better increased from 46% at baseline to 61% at 12 months after initiating infliximab therapy. In contrast, three eyes (10%) with a BCVA of 0.1 or less at baseline experienced no improvement in visual acuity owing to prior optic disc and/or macular atrophy. Previous studies have shown that the major reasons for poor visual outcomes in Behçet's disease are macular atrophy, optic disc atrophy and chorioretinal atrophy.5 6 Moreover, a relationship between the number of ocular inflammatory attacks and poor visual prognosis has been documented.5 6 Taken together, this strongly suggests that the initiation of infliximab therapy early on during the uveitis disease course would be beneficial in maintaining good visual function in patients with Behçet's disease.
Serious adverse effects were not observed in the present study. Notably, although six of 14 patients had positive PPD test results and received isoniazid prophylaxis, no patients developed tuberculosis during the follow-up period. Consistent with our findings, previous studies have also reported that infliximab treatment did not result in PPD-positive patients developing tuberculosis if proper prophylaxis was used.11 However, in a preliminary open label study of infliximab in Behçet's disease in Japan, Ohno and colleagues reported one case of miliary tuberculosis among 13 patients.10
Some patients on infliximab have been known to develop antibodies against the drug (human antichimera antibodies), and it has been speculated that the presence of these antibodies may be associated with a greater risk of infusion reactions.14 Furthermore, it has been reported that the development of anti-infliximab antibodies is associated with low circulating drug levels.23 In patients with rheumatoid arthritis and Crohn's disease, the use of infliximab with concomitant methotrexate has been shown to reduce the incidence of infusion reactions.14 15 Given such data, in our study we elected to continue concomitant ciclosporin albeit at lower doses, with the hope of reducing the immunogenicity of infliximab treatment. However, four of 14 patients developed infusion reactions, and the infliximab therapy was eventually halted in two of these patients. Anti-infliximab antibodies were not measured, and therefore any relation between infusion reactions and the development of antidrug antibodies cannot be determined. Furthermore, the dose of concomitant ciclosporin may have been inadequate to suppress the development of antibodies. Finally, it is possible that methotrexate, as commonly administered in rheumatoid arthritis, may be more effective than ciclosporin in suppressing antibody development.
The limitations of this study are that the data were examined retrospectively, all patients were from a single institution, and the number of the patients was small. Furthermore, several years of follow-up would be necessary to evaluate the full scope of the efficacy and safety of using infliximab in Behçet's disease. Even so, our results suggest strong efficacy for infliximab in suppressing not only ocular inflammatory attacks but also background retinal and optic disc vascular leakage, with the BCVA improving or being maintained in 93% of eyes at 12 months.
References
Footnotes
Competing interests HK and AAO have received lecture fees and research grants from Mitsubishi Tanabe Pharma, the distributor of infliximab in Japan.
Provenance and peer review Not commissioned; externally peer reviewed.