Article Text

Abstract
Background Up to 70% of children and teenagers referred to a paediatric gastroenterology centre with suspected inflammatory bowel disease (IBD) do not have the disease.
Objective To evaluate whether faecal calprotectin as an ‘add-on test’ improves the specificity of the clinical case definition for suspected IBD in a general paediatric practice.
Design A prospective diagnostic accuracy study.
Setting Six outpatient clinics for general paediatrics and one tertiary care hospital in the Netherlands.
Patients 117 children and teenagers with a clinical suspicion of IBD.
Diagnostic tests Faecal calprotectin was measured (index test) in all patients. Patients with a high index of suspicion on the basis of the paediatrician's global assessment, physical examination and blood results were referred for endoscopy (reference standard). Children and teenagers who were not selected for endoscopy initially were followed for half a year for the appearance of possible additional symptoms (delayed type reference standard).
Primary outcome The proportion of referred patients with confirmed IBD.
Results The mean age of patients was 14 years (range 6–18). A total of 42 (36%) had confirmed IBD. The paediatricians, who were blinded to the faecal calprotectin result, referred 68 children and teenagers for endoscopy. If they had referred only those patients with a positive faecal calprotectin result (>50 μg/g), 54 patients would have undergone endoscopy.
Limitation The study relied on clinical follow-up to detect missed IBD.
Conclusions A diagnostic strategy in general paediatric practice of using a simple clinical case definition for suspected IBD in combination with a positive faecal calprotectin result increases the specificity to detect IBD and reduces the need for referral to a paediatric gastroenterology centre with a very low risk of missing cases.
- Faecal calprotectine
- Inflammatory bowel disease
- endoscopy
- Children
- Diagnostic algorithm
Statistics from Altmetric.com
What is already known on this topic
-
Diagnosing inflammatory bowel disease (IBD) requires invasive and time-consuming endoscopy.
-
In a relatively large proportion of patients with symptoms suggesting IBD the results of endoscopy are negative.
-
Faecal calprotectin is a sensitive marker of intestinal inflammation and justifies urgency for endoscopy.
What this study adds
-
Selecting patients for ileocolonoscopy based on increased faecal calprotectin levels in the absence of gastrointestinal infection reduces the number of negative endoscopies.
-
Paediatricians can safely rule out IBD in their patients when a normal calprotectin level is measured in the stool.
Introduction
For the paediatrician treating a child with recurrent abdominal pain and diarrhoea it is often difficult to clinically distinguish between those who need an endoscopy and those who do not. Identification of children with low likelihood of organic disease would justify a non-invasive ‘watchful waiting’ strategy, while a high likelihood of inflammatory bowel disease (IBD) would justify referral to specialist services for endoscopy. In a recently published diagnostic meta-analysis1 we found that increased levels of calprotectin in the stool can identify children who are most likely to have IBD. All included studies used the fully paired design in which a group of patients first undergo faecal calprotectin testing and then endoscopy. These studies estimated the diagnostic accuracy of faecal calprotectin under ideal experimental circumstances. We conducted a phase III diagnostic accuracy study to determine whether faecal calprotectin could serve as a screening test to identify children with a high likelihood for IBD and reduce the number of children and teenagers undergoing invasive endoscopy.
We aimed to determine an objective diagnostic strategy to minimise the number of children and adolescents with negative endoscopy results without missing any cases of IBD.
Patients and methods
Study setting and participants
This study was performed at the paediatric outpatient clinic of six general hospitals and one tertiary care hospital (University Medical Center Groningen (UMCG)) in the northern region of the Netherlands. Most paediatricians in the general hospitals were trained as fellows in paediatric gastroenterology and half of them had their training at UMCG. Children and teenagers between 6 and 18 years of age with abdominal complaints were eligible for participation. Younger children have higher normal values of faecal calprotectin and were excluded for this reason.2 ,3 Patients were included when they fulfilled the clinical case definition for suspected IBD (box 1).
Criteria used to define a population of children and teenagers with a clinical suspicion of inflammatory bowel disease
-
Persisting diarrhoea (>4 weeks)
-
or recurrent (≥2 episodes in 6 months) abdominal pain and diarrhoea
-
and at least one of the following criteria
-
rectal blood loss
-
unintended weight loss or linear growth retardation
-
peri-anal symptoms (skin tag, fistula, fissure, abscess)
-
anaemia (haemoglobin cut-off point in mmol/litre): <12 years: 7.1; girls ≥12 years: 7.4; boys ≥12 years: 8.14 or other extra-intestinal manifestations (erythema nodosum, arthritis, uveitis)
-
increased markers of inflammation: erythrocyte sedimentation rate >20 mm/h; C-reactive protein >10 mg/litre
-
Data collection
After the first presentation at the outpatient clinic, all patients provided a stool sample collected at home. The faecal samples were analysed at the Department of Laboratory Medicine, UMCG by a commercially available quantitative assay (CALPRO ELISA test (ALP); Calpro AS, Lysaker, Norway). The manufacturer cut-off point is 50 µg/g stool. Laboratory technicians were blinded to the final diagnosis of the patients. The decision to perform any other diagnostic tests (including endoscopy) was left to the paediatric gastroenterologist's discretion and was independent of the faecal calprotectin result. Confirmation of IBD was obtained after endoscopic and histological evaluation according to the European Society for Paediactric Gastroenterology Porto Criteria.5 The diagnosis ‘non-IBD’ was made when other test results gave a convincing explanation for the symptoms, or when the symptoms had completely resolved at 6-month follow-up. An experienced paediatric histopathologist, who was blinded to the results of other diagnostic tests, assessed each biopsy specimen. Stool cultures were evaluated for Salmonella, Shigella, Yersinia, Campylobacter, Clostridium difficile (inclusive of toxin A and B), Giardia lamblia, Entamoeba histolytica and parasites (figure 1).
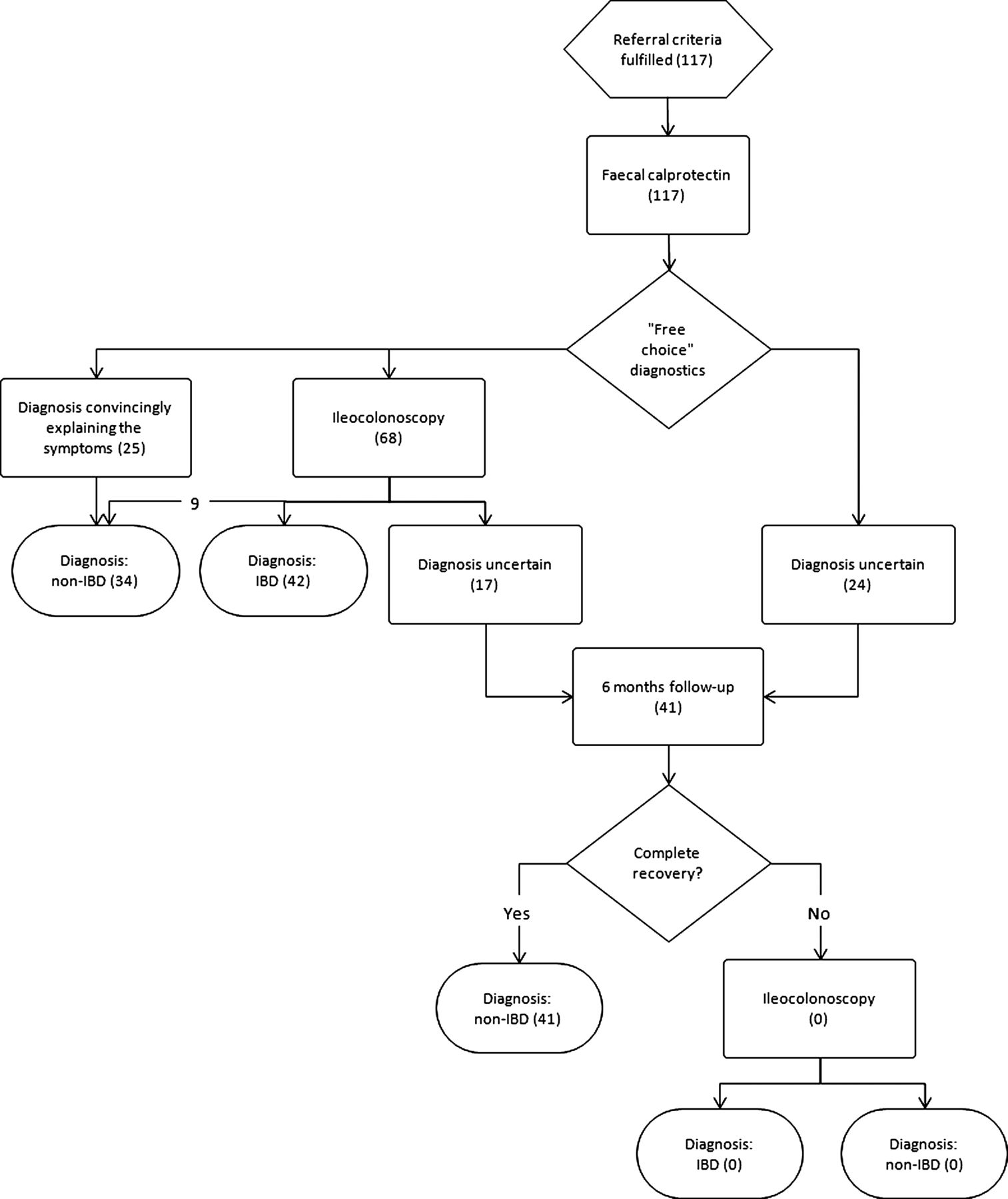
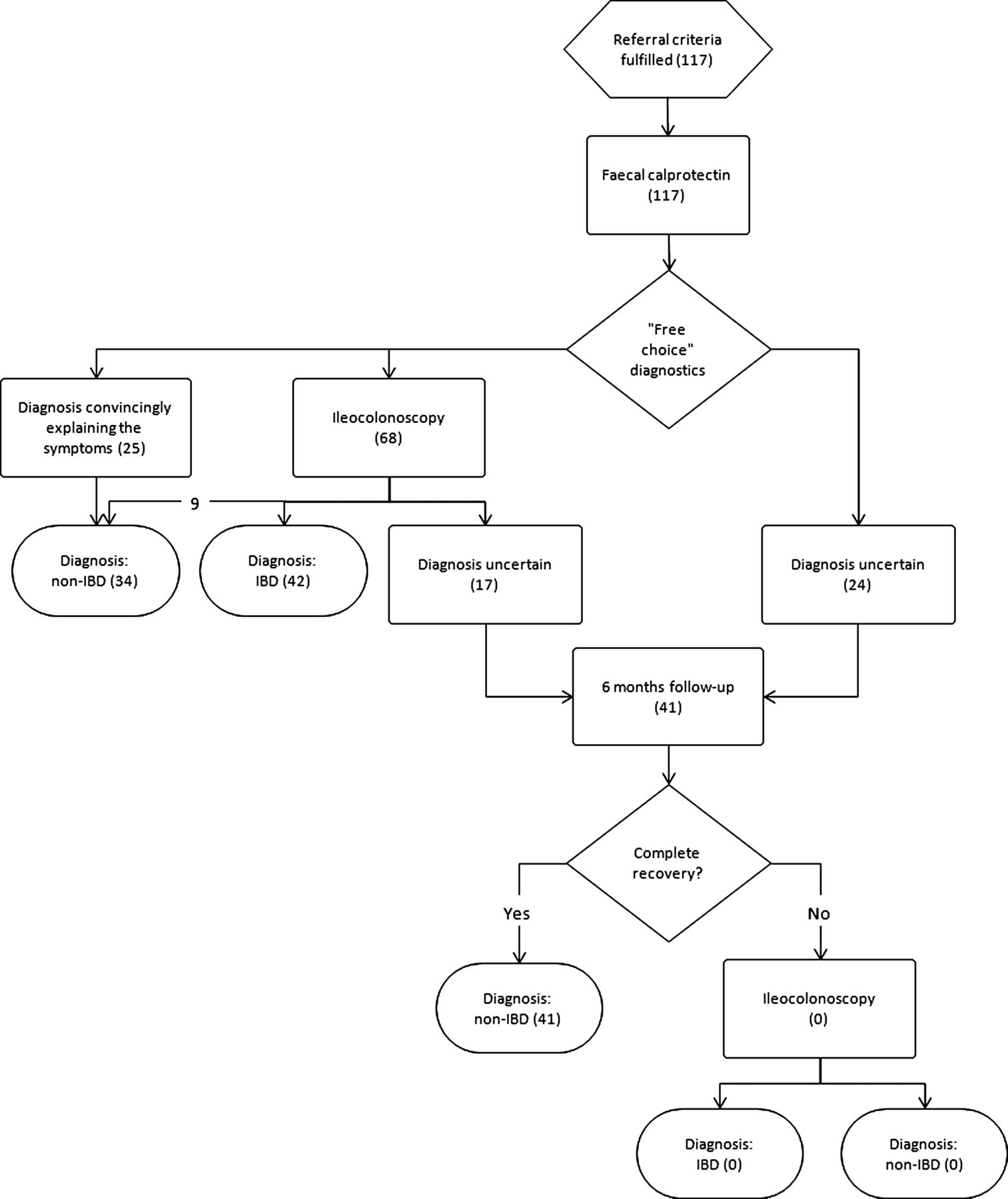{kind=link}
Study design and patient flow (n). IBD, inflammatory bowel disease.
Statistics
Parameters of test reliability including sensitivity, specificity, likelihood ratios and post-test probabilities with their 95% CIs were calculated with the use of the MedCalc statistical software package for biomedical research (V.12.1.4). To compare the specificities of the different diagnostic pathways the McNemar test for paired data was used. Student's t tests and χ2 tests were used to compare baseline characteristics between groups. All tests were two sided and the level of significance used was a p value<0.05. Data were analysed in SPSS (V.19.0 for windows).
Results
Between February 2009 and June 2010, 117 children and teenagers were prospectively included in the study. Patient characteristics are presented in table 1.
Patient characteristics
IBD was confirmed in 42 patients (36%). Twenty-four were diagnosed with Crohn's disease, 16 with ulcerative colitis and two with IBD unclassified. There were no differences in age and sex between the groups with confirmed IBD and non-IBD. The paediatricians, who were blinded to the faecal calprotectin result, referred 68 children and teenagers for endoscopy on the basis of a high index of suspicion for IBD. They were evaluated according to the Porto criteria with gastroscopy and ileocolonoscopy (97% ileal intubation) with segmental biopsies for histological evaluation. One child was diagnosed with Crohn's disease after a negative gastroscopy and ileocolonoscopy but positive magnetic resonance enterography.
Table 2 shows the diagnoses of patients without IBD. The majority of these patients did not need endoscopy to exclude IBD and had other tests including stool analyses for bacteria, ova and parasites, gastroscopy, abdominal ultrasound, CT scan, Meckel scan, serology and dietary measurements leading to the diagnosis. Thirty-two children and teenagers were diagnosed with functional abdominal pain and were followed for at least 6 months to confirm this diagnosis. Seven of these patients had elevated calprotectin (range 97–400 µg/g stool) and 11 underwent endoscopy (including ileocolonoscopy) with negative results. Sixteen patients without IBD had abdominal ultrasound, six CT enteroclysis and three abdominal MRI as part of their diagnostic workup. Seven patients had no definite diagnosis despite several tests and had spontaneous recovery of their ailments during follow-up.
Non-inflammatory bowel disease diagnoses (n=75)
Median time between faecal sampling for calprotectin and endoscopy was 22 days (range 0–79) in the confirmed IBD group and 42 days (0–164) in the non-IBD group (p=0.105).
Diagnostic accuracy
The pretest probability of IBD in our study population was 36%. Calprotectin (cut-off point 50 μg/g) was elevated in all children and teenagers with IBD (sensitivity 100%, 95% CI 92% to 100%), and in 20 out of 75 patients without IBD (specificity 73%, 95% CI 62% to 83%). Table 3 shows that a value above the cut-off point (in the absence of gastrointestinal infection) gives a specificity of 81% (95% CI 69% to 90%).
Added value of the ‘clinical eye’ or faecal calprotectin testing in a population of children and teenagers suspected of having inflammatory bowel disease
Scenario analysis
When the decision to schedule patients for endoscopic evaluation is left to the paediatrician's discretion (as was the case in our study), 38% of the children and teenagers subjected to ileocolonoscopy had a negative result (table 4). If the decision for referral were to be solely based on the faecal calprotectin result, 32% of the children subjected to ileocolonoscopy would have had a negative result. Basing referral on a positive faecal calprotectin result in the absence of gastrointestinal infection would have resulted in 22% negative ileocolonoscopies and no missed IBD cases. The reduction of negative endoscopies is significant (p=0.001).
Scenario analysis
Discussion
Implications of key findings
To our knowledge, this is the first phase III study that evaluated the usefulness of faecal calprotectin in routine paediatric practice. The analytical eye of the paediatrician selected 68 children and teenagers for endoscopy to confirm IBD, of which 26 (38%) had a negative result. A referral based on a faecal calprotectin level above 50 μg/g without excluding a gastrointestinal infection would wrongly select 20 out of 62 patients (32%). When patients with proven gastrointestinal infections are excluded beforehand the number of IBD-negative endoscopies would be significantly reduced to 22% (12 out of 54 suspected patients) without missing one case of IBD.
Comparison with other studies
We recently published a diagnostic meta-analysis1 in which we summarised the best available evidence on the diagnostic accuracy of faecal calprotectin for screening. We included the reports of six adult studies and seven phase II studies in children and teenagers. We concluded that calprotectin is accurate when screening for suspected IBD in adults but less so in children. The pooled sensitivity and specificity in children and teenagers was 0.92 (95% CI 0.84 to 0.96) and 0.76 (95% CI 0.62 to 0.86), respectively. Gastrointestinal infections, especially bacterial infections with Shigella, Yersinia or Salmonella, can mimic the onset of IBD in children and teenagers and cause increased faecal calprotectin levels. Since the publication of our meta-analysis two new paediatric phase II studies have been published.6 ,7 In these studies a fully paired design was used in which all included children were subjected to endoscopic evaluation. In ‘real life’, when another diagnosis than IBD is more likely, paediatricians may wish to avoid this invasive and uncomfortable procedure. The major difference between the Diamanti study and ours was a remarkably high pretest probability of 60% that can be explained by the tertiary care setting in which a highly selected group of patients with suspected IBD was seen. In our study the pretest probability was 36%. In the Henderson study the patients with a high calprotectin result and no endoscopy were not evaluated and followed up.
Limitations of this study
Although phase II studies give cause to overestimate diagnostic accuracy, the validity of a phase III study like ours is also compromised. As not all patients underwent the reference test, uncertainty remains about the correct diagnosis in some patients. We therefore decided to add another prognostic dimension to the reference standard, namely, the clinical course of patients. IBD is not a self-limiting disease and will usually become clinically manifest within a few months after the first diagnostic suspicion, in this study the moment of enrolment. Patients who remained free of disease for 6 months were believed not to have IBD. This ‘delayed type’ diagnosis may not be ideal, but is the best achievable solution closely connected with the reality of clinical care.8
Faecal calprotectin can give false-positive results when patients use non-steroidal anti-inflammatory drugs9–11 or proton pump inhibitors.12 We did not collect information about the use of these drugs in the study population, which could be the reason why some children with functional abdominal pain had elevated faecal calprotectin. In a cross-sectional study of school-aged children with functional abdominal pain and irritable bowel syndrome, slightly elevated calprotectin concentrations were found in their stools compared with control children.13 However, the concentrations were clearly in the lower range (65±75 μg/g) while the majority of confirmed IBD cases in our population had concentrations way above 500 μg/g on their first presentation.
Applicability of findings to paediatric care
Pretest probability of IBD in our study population was 36%. The study population was a combination of patients from secondary and tertiary care hospitals, where the emphasis is usually on ‘ruling in’: increasing the probability of IBD before carrying out more expensive, time-consuming and invasive procedures; establishing a firm diagnosis; and starting appropriate treatment. A diagnostic test with a high specificity is therefore preferred.14 In this study we tested the ‘ruling out’ properties of faecal calprotectin in paediatric practice. We found that a normal calprotectin level reduces the probability of IBD to zero. In other words, the diagnosis of IBD can be ruled out with confidence. The paediatrician does not need to refer the patient for endoscopic evaluation but can provide reassurance or adopt a ‘watchful waiting’ strategy.
C-reactive protein (CRP) is a far less reliable test to rule out IBD than calprotectin. In a recently published paper a large number of children and teenagers with newly diagnosed IBD proved to have normal CRP levels.15
The conclusions of this study cannot simply be translated into the practice of the general practitioner or family doctor. IBD prevalence in the general population is much lower. In the first-line setting the number of false-positive calprotectin results will therefore increase, exposing too many patients without IBD to unnecessary endoscopic procedures. At present there is no evidence of how the test performs in primary care. If studies conducted in primary care find a high diagnostic accuracy of the faecal calprotectin test, it will be an important step forward in how IBD is diagnosed.
Conclusion
A diagnostic strategy in general paediatric practice of using a simple clinical case definition for suspected IBD in combination with a positive faecal calprotectin result increases the specificity to detect IBD and reduces the need for referral to a paediatric gastroenterology centre with a very low risk of missing any cases. At the same time normal calprotectin levels confidently rule out intestinal inflammation and further investigations can be tailored appropriately without referring the patient for endoscopy. This is good news for patients (less invasive tests) and clinicians (shorter waiting lists for endoscopy).
Acknowledgments
We thank the members of the North Netherlands Paediatric IBD Consortium (Gieneke Gonera-de Jong, Wilhelmina Hospital, Assen, the Netherlands; Jan Uitentuis, Medical Center Leeuwarden, the Netherlands; Obbe F Norbruis, Isala Clinics, Zwolle, the Netherlands; Lidy AT van Overbeek, Scheper Hospital, Emmen, the Netherlands; Stefan van Dorth, De Tjongerschans Hospital, Heerenveen, the Netherlands; and Herman J. Waalkens, Martini Hospital, Groningen, the Netherlands) for recruiting their patients and facilitating this study. We thank Dr Stijn Verhulst for reviewing the statistical calculations.
References
Footnotes
-
Contributors Specific author contributions: EVV: wrote the manuscript; PFR: conceived and designed the study, performed data review and analysis with EVV, ABS, WRC and ACMK. All members of the North Netherlands Pediatric IBD Consortium mentioned in the acknowledgments provided patients for this study. All authors have approved the manuscript.
-
Competing interests None.
-
Ethics approval Institutional review board.
-
Provenance and peer review Not commissioned; externally peer reviewed.