Article Text

Abstract
Objectives To test whether patients with immune-mediated inflammatory disease (IMIDs), who did not respond to two doses of the SARS-CoV-2 vaccine, develop protective immunity, if a third vaccine dose is administered.
Methods Patients with IMID who failed to seroconvert after two doses of SARS-CoV-2 vaccine were subjected to a third vaccination with either mRNA or vector-based vaccines. Anti-SARS-CoV-2 IgG, neutralising activity and T cell responses were assessed at baseline and 3 weeks after revaccination and also evaluated seprarately in rituximab (RTX) and non-RTX exposed patients.
Results 66 non-responders were recruited, 33 treated with RTX, and 33 non-exposed to RTX. Overall, 49.2% patients seroconverted and 50.0% developed neutralising antibody activity. Seroconversion (78.8% vs 18.2%) and neutralising activity (80.0% vs 21.9%) was higher in non-RTX than RTX-treated patients with IMID, respectively. Humoral vaccination responses were not different among patients showing positive (59.3%) or negative (49.7%) T cell responses at baseline. Patients remaining on mRNA-based vaccines showed similar vaccination responses compared with those switching to vector-based vaccines.
Conclusions Overall, these data strongly argue in favor of a third vaccination in patients with IMID lacking response to standard vaccination irrespective of their B cell status.
- antirheumatic agents
- biological therapy
- COVID-19
Data availability statement
Data are available on reasonable request. N/A.
This article is made freely available for personal use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Key messages
What is already known about this subject?
While it is known that SARS-CoV-2 vaccination achieves protective immunity in the majority of patients with immune-mediated inflammatory diseases, it is currently unknown whether patients not achieving protective immunity while profit from revaccination .
What does this study add?
The study shows that revaccination of non-responders is effective and safe. The vast majority of non-responder patients that have not experienced previous treatment with B cell depleting agents seroconvert and mount protective immunity after SARS-CoV-2 revaccination, while responses are substantially lower in patients pre-exposed to B cell depleting agents. Vaccination responses are achieved in patients with homologous (mRNA-mRNA) as well as heterologous (mRNA-vector) revaccination.
How might this impact on clinical practice or future developments?
These data suggest that fast SARS-CoV-2 revaccination should be considered in patients with immune mediated inflammatory diseases that did not achieve protective immunity after two SARS-CoV-2 vaccinations.
Introduction
Patients with immune-mediated inflammatory diseases (IMIDs) are a vulnerable population during the COVID-19 pandemic.1 Patients with IMID in general2 and particularly those treated with methotrexate,3 mycophenolate, glucocorticoids, abatacept4 and with an even greater magnitude, those receiving B cell depleting agents5 show reduced humoral immune responses to anti-SARS-CoV-2 vaccination. Hence, since a considerable fraction of patients with IMID experiences insufficient vaccination responses, alternative SARS-CoV-2 vaccination strategies need to be considered, that is, the fast re-exposure of patients that did not respond to double vaccination in order to achieve sufficient protection in this vulnerable patient group. Based on these observations and since antibody responses to SARS-CoV-2 vaccines decline even in healthy individuals,6 public health authorities such as the US Food and Drug Administration advocate for booster SARS-CoV-2 vaccination for immunocompromised individuals.
Current data on the efficacy and safety of revaccination of non-responder patients with IMID are limited to two case reports7 8 suggesting that such a strategy may work. The success of revaccination may depend on a functional adaptive immune system, which is particularly blunted in patients that have received B cell depleting agents (rituximab, RTX). A preprint of a study investigating the response to SARS-CoV-2 revaccination in patients exposed RTX showed that a limited number of patients (27%) manage to seroconvert with no difference whether they switched from an mRNA to a vector, based vaccine or whether they stayed on an mRNA-based vaccine.9 Whether and how patients with IMID who are not exposed to RTX but failed to achieve response to SARS-CoV-2 vaccination will respond to revaccination is currently unclear. Furthermore, recent studies in healthy individuals indicated better response to heterologous vector/mRNA vaccination regimens compared with homologous mRNA/mRNA or vector/vector regimens10–13 which brings about the question as to whether a switch of vaccination strategy should be considered in non-responders.
We, therefore, prospectively recruited patients with IMID (both RTX exposed and non-exposed) that did not respond to two doses of the SARS-CoV-2 vaccine to evaluate the humoral and cellular immune response after homologous or heterologous anti-SARS-CoV-2 revaccination.
Methods
Participants
This prospective study included patients with IMID (only rheumatic diseases) who failed to develop SARS-CoV-2 spike protein antibodies (OD450nm<1.1 in the Euroimmun anti-SARS-CoV-2 spike S1 protein ELISA) at least 4 weeks after the full vaccination with the mRNA vaccine BNT162b2 (Pfizer/Biontech) or the vector vaccine ChAdOx1 (AstraZeneca). Patients with a history of SARS-CoV-2-specific antibodies or PCR-confirmed SARS-CoV-2 infection before vaccination were excluded. All patients remained under stable treatment throughout the whole study period. The IMID non-responders were recruited from a large longitudinal COVID-19 study at the Deutsche Zentrum Immuntherapie that has been initiated in February 2020 and monitors anti-SARS-CoV-2 antibody responses over time.14 Demographic, disease-specific and vaccination data were recorded in all participants.
Procedure
Patients received either BNT162b2 or ChAdOx1 nCoV-19 vaccine. The vaccination centre of the city of Erlangen provided the vaccines for this study free of charge through the Central Pharmacy of the University Hospital of Erlangen. IgG antibodies were tested by a commercial ELISA (Euroimmun, Lübeck, Germany) with a cut-off OD450nm of 1.1. For neutralisation activity, a CE-In Vitro Diagnostics-certified SARS-CoV-2 surrogate virus neutralisation assay (cPASS, Medac, Wedel, Germany) was used with a cut-off of 30% inhibition. The detection of SARS-CoV-2 specific T-cells was conducted via an IFN-γ ELISpot Assay (T-SPOT.COVID, Oxford Immunotec), a response was considered positive when the number of spots was ≥8 spot forming units (SFUs) above the negative control. A detailed description of laboratory assessments is provided in online supplemental file. IgG antibodies, neutralising capacity and T-cells responses were measured before and 3 weeks after the revaccination.
Supplemental material
Statistical analysis
We summarised participant characteristics using means, SDs, quantiles or proportions as appropriate. We used McNemar’s test to compare paired categorical observations and Fisher’s exact test to compare proportions. To compare the proportion of patients with a humoral response after the third vaccination by categories of T-cell response before the third dose we used the Cochran-Mantel-Haenszel test in order to account for a possible differential effect caused by RTX treatment. Two-sided p values less than 0.05 were considered significant without adjustment for multiple testing. Missing data were assumed to be missing completely at random and not imputed.
Patient and public involvement
The study was primarily motivated by frequent inquiries from patients with IMID on the subject matter but undertaken without any direct public involvement.
Results
Patient characteristics
Sixty-six patients with IMID were included, 33 of whom were exposed to RTX. Most patients had rheumatoid arthritis (45.5%), followed by systemic vasculitis (21.2%) and connective tissue disease (19.7%). Fifty-eight patients had been fully immunised with two doses of mRNA vaccine BNT162b2, the remaining eight patients had been fully immunised with the vector vaccine. Patients receiving RTX had received a median (IQR) of 7 (4–7.5) cycles and the last treatment cycle had been given a median (IQR) of 4.5 (3–8) months before the third vaccination. The median (IQR) CD19 cell count in the RTX-treated patients was 0/mm3 (range 0–68). Details of demographics and clinical characteristics of patients are depicted in table 1.
Baseline demographics and clinical characteristics of patients with IMID
Humoral immune response to revaccination
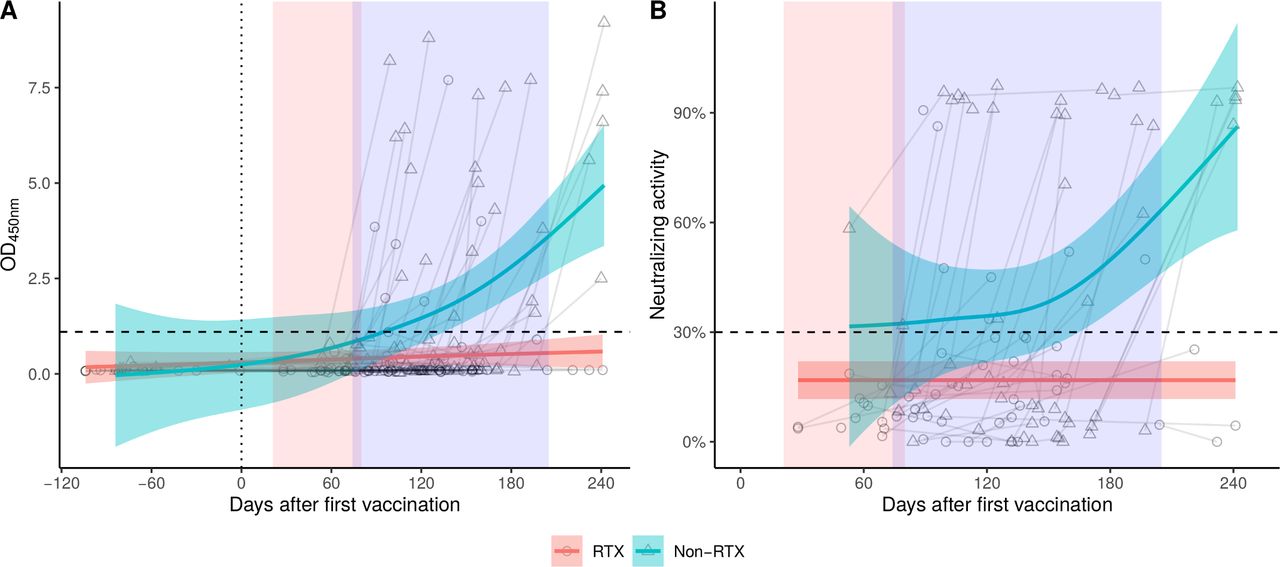
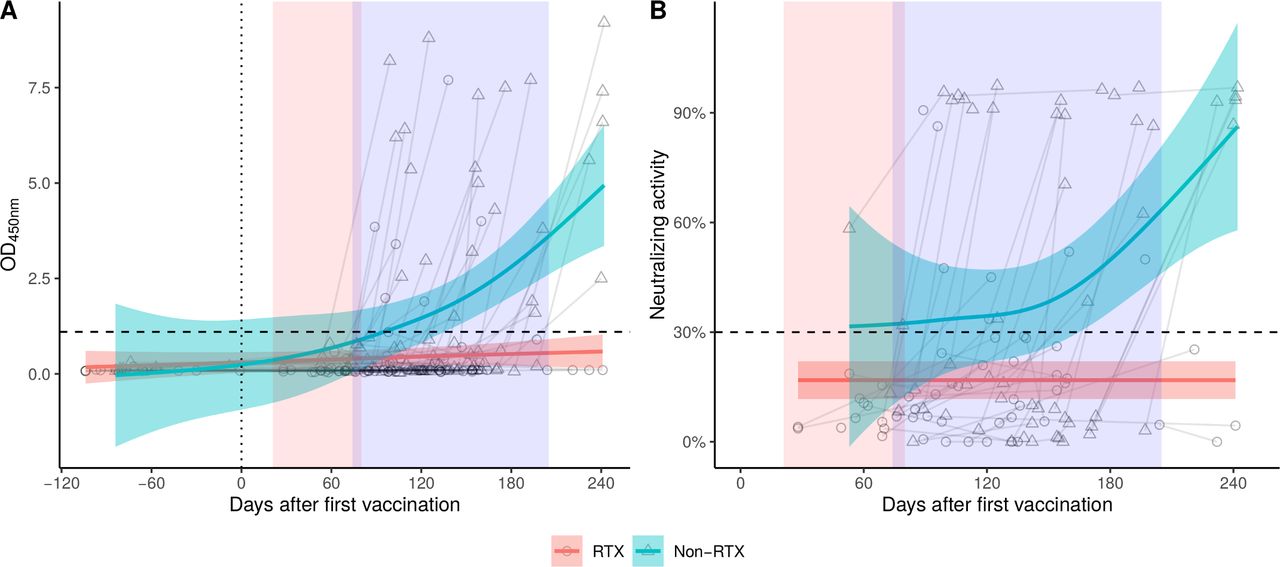
After revaccination, 32/65 patients (49.2%) seroconverted and developed positive anti-SARS-CoV-2 IgG antibodies (p<0.0001 compared with baseline). This increase was largely driven by the non-RTX pretreated group, in which 26/33 (78.8%) patients achieved seroconversion, while in the RTX pretreated group, only 6/33 (18.2%) patients responded (p<0.0001, table 2). Neutralising antibodies were present in 31/62 patients (50%) after the third vaccination (p<0.0001 compared with baseline). 24/30 (80.0%) of patients in the non-RTX pretreated group had neutralising antibodies compared with only 7/32 (21.9%) among patients pretreated with RTX (p<0.0001). The time course of antibody and neutralising activity levels are depicted in figure 1. The correlation between the time from last RTX administration and antibody response was low (Spearman’s r=0.31, p=0.093).
{kind=link}
The time course of humoral response to revaccination showing optical densities corresponding to SARS-Cov2 S1 IgG antibody levels (A) and per cent neutralising activity (B). Red and blue shaded areas indicate the respective periods during which second and third vaccinations were administered. Horizontal dotted lines indicate the corresponding cut-off values for the antibody and neutralisation assays. Curves with 95% confidence bands indicate the mean values over time for rituximab (RTX, red) and non-RTX (non-RTX, turquoise) groups.
Humoral and cellular immune responses before and after revaccination
Cellular immune response to revaccination
A T-cell response was present in 59.3% of all patients at baseline. After revaccination, this overall increased to 73.3% (p=0.08) (table 2). The prevalence of T-cell responses was higher in RTX-pretreated patients before the third vaccination (68.8%) and significantly (p=0.0039) thereafter (86.7%). The increasing proportion of T-cell response after the third dose was largely attributable to RTX-treated patients. T cell responses to SARS-CoV-2 at baseline were not associated with subsequent antibody development (p=0.08 by Cochran-Mantel-Haenszel test stratified by RTX use, online supplemental table 1).
Comparison of homologous and heterologous vaccination strategies
When separately analysing the seroconversion rates in patients receiving homologous (mRNA-mRNA) versus heterologous vaccinations, we did not find significant differences between the two strategies (homologous: 40% seroconversion, heterologous: 55% seroconversion) (online supplemental table 2). Also, concerning neutralising capacities (40% vs 56.8%) and T cell responses (65.2% vs 78.4%) no differences between the two vaccination strategies were found.
Safety of revaccination in non-responders
Analysis of the tolerability of SARS-CoV-2 revaccination showed good safety. Overall 38/66 (58%) participants reported no side effects. The most frequently reported complaints were fatigue (25.8%), pain at the injection site (22.7%), headache (10.6%) and myalgia (9.1%) (online supplemental table 3).
Discussion
Our data show that revaccination is highly effective to mount humoral immune responses in patients with IMID that have previously not responded to double vaccination. These data are important and reassuring for patients with IMID, as previous data have shown that vaccination responses are blunted and one out of 10 patients with IMID does not develop neutralising antibodies after the first and second SARS-CoV-2 vaccination.2 About half of the patients profited from a revaccination, with seroconversion, the presence of neutralising activity and enhanced T cell responses. Importantly these data do not reflect a ‘booster’ effect, meaning revaccination of individuals that have responded to first and second vaccination, but gradually lost their immune response later on. These data exclusively refer to patients that failed to develop humoral immunity to first and second vaccination.
The efficacy of revaccination in non-responders was primarily dependent on whether patients received previous RTX. Hence, seroconversion rates were limited in RTX-treated non-responders (20%) while they were high (80%) in patients not exposed to RTX indicating that revaccination in B cell competent non-responders is highly effective. Similar results were observed for neutralising antibody activity. Notably, T cell responses were not influenced by RTX, as the vast majority (86%) of RTX-treated patients developed T cell immunity against SARS-CoV-2 after revaccination. The enhanced T cell responses in RTX exposed participants could be based on the known suppressive function of regulatory B cells on T cells, which is resolved on B cell depletion.15 To date, a protective effect of SARS-CoV-2 specific T cells has not been conclusively shown, however, there is no reason to believe that such T cells response would not contribute to viral defence .Of note, SARS-CoV-2-specific T cell responses have shown to cross-react across SARS-CoV-2 strains further supporting their protective role.16
We also had the opportunity to study the vaccination regimen. Thus, re-exposure to mRNA vaccine in patients not responding to full vaccination with an mRNA vaccine was as effective as the switch to vector-based vaccines. These data suggest that there is no need to switch the vaccine regimen in non-responders, as the third dose of the same vaccine still allows significant seroconversion and neutralising activity.
Taken together, these data show that patients with IMID not responding to SARS-CoV-2 vaccination profit from revaccination and mount significant protective immunity. These findings also underline the importance of testing of SARS-CoV-2 antibody status in vaccinated patients with IMID in order to identify those with insufficient responses requiring revaccination. Since about 10% of patients with IMID do not adequately respond to full vaccination,2 antibody testing in patients with IMID seems reasonable if done done at least 14 days after the second vaccine dose. Monitoring of vaccination responses to identify non-responders and their subsequent rapid re-exposure to a third vaccine dose might therefore help to achieve better protection of patients with IMID from SARS-CoV-2 infection.
Data availability statement
Data are available on reasonable request. N/A.
Ethics statements
Patient consent for publication
Ethics approval
Ethical approval (#157_20 B) to conduct this study was granted by the Institutional Review Board of the University Hospital Erlangen. Written informed consent was obtained from the study participants.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Johannes WJ Bijlsma
DS, KT and FF contributed equally.
Contributors Study design: DS, KT, BM, GK and GS. Sample collection: DS, AK, AR, VS, DB, JK and KM. Experiments and data analysis: DS, KT, KS, FF, KT and TH. Data interpretation: DS, KT, FF and GS. Writing of the manuscript: DS, KT, FF and GS. Critical proof reading of the manuscript: all authors. GS accepts full responsibility for the work and/or the conduct of the study, had access to the data and controlled the decision to publish.
Funding The study was supported by the Deutsche Forschungsgemeinschaft (DFG-FOR2886 PANDORA and the CRC1181 Checkpoints for Resolution of Inflammation). Additional funding was received by the Bundesministerium für Bildung und Forschung (BMBF; project MASCARA), the ERC Synergy grant 4D Nanoscope, the IMI funded project RTCure, the Emerging Fields Initiative MIRACLE of the Friedrich-Alexander-Universität Erlangen-Nürnberg, and the Else Kröner-Memorial Scholarship (DS, no. 2019_EKMS.27). KS was supported by the Hector foundation (project M2102).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.