Article Text

Abstract
Purpose To compare the effectiveness of anti-tumour necrosis factor (TNF) agents in biologically naive and ‘switched’ rheumatoid arthritis (RA) patients.
Methods RA patients enrolled in the CORRONA registry newly prescribed adalimumab (n=874), etanercept (n=640), or infliximab (n=728) were stratified based on previous anti-TNF use. Clinical effectiveness at 6, 12 and 24 months was examined using the modified American College of Rheumatology response criteria (mACR20/50/70) and achievement of remission (28-joint disease activity score (DAS28) and clinical disease activity index (CDAI)) in unadjusted and adjusted analyses. The persistence of anti-TNF treatment was examined using Cox proportional hazard models.
Results Among 2242 patients (1475 biologically naive, 767 switchers), mACR20, 50 and 70 responses were similar (p>0.05) for adalimumab, etanercept and infliximab at all time points, as were rates of CDAI and DAS28 remission (p>0.05). Response and remission outcomes were consistently inferior for switched versus biologically naive patients. The adjusted OR for achieving an mACR20 response was 0.54 (95% CI 0.38 to 0.76) in first-time switchers and 0.42 (95% CI 0.23 to 0.78) in second-time switchers versus biologically naive patients at 6 months. The adjusted OR for achieving DAS28 remission were 0.29 (95% CI 0.15 to 0.58) for first-time switchers and 0.26 (95% CI 0.08 to 0.84) for second-time switchers. Persistence was higher in biologically naive patients, for whom persistence was highest with infliximab.
Conclusions No differences in rates of drug response or remission were observed among the three anti-TNF. Infliximab was associated with greater persistence in biologically naive patients. Response, remission and persistence outcomes were diminished for patients who switched anti-TNF.
Statistics from Altmetric.com
Over the past decade, anti-tumour necrosis factor (TNF) therapies have become the most frequently prescribed class of biological agents for the treatment of rheumatoid arthritis (RA) in the USA and Europe. Currently, there are five anti-TNF agents approved by the European Medicines Agency and the US Food and Drug Administration, with varying structures, dosing and pharmacokinetics. Despite these differences, they all block TNF, and two randomised clinical trial (RCT) meta-analyses of three commonly prescribed anti-TNF (adalimumab, etanercept and infliximab) concluded that the three anti-TNF demonstrated comparable efficacy.1 2 However, these meta-analyses have been criticised, and their findings conflict with the results reported in two European registry studies demonstrating that adalimumab and etanercept users have better clinical responses than infliximab users.3 4 Those reports originated from European countries with more restricted access to biological agents and dosage restrictions.
An important caveat to the application of anti-TNF RCT results to RA patients in the clinic is that the vast majority of the RCTs were conducted in biologically naive patients, particularly in those without a previous history of anti-TNF treatment. However, intraclass switching of anti-TNF agents is common in clinical practices in Europe and the USA.5,–,8 Currently, there is inadequate evidence regarding the benefits of this strategy. As a result, switching patients to a different anti-TNF agent is restricted in certain European countries. Comparative effectiveness research using observational data sources has gained broader support in Europe and the USA across clinical disease areas.9,–,11
Comparative effectiveness studies using observational data from registries represent a promising alternative to RCT for comparing interventions and therapies between biologically naive patients and patients who switch anti-TNF.11 This is important because rheumatologists in the USA and many European countries prescribe anti-TNF agents to RA patients with markedly lower disease activity than RCT populations.12,–,14 Given that comparative effectiveness data for US-based cohorts are lacking, the aim of the present study was to compare the clinical effectiveness of specific anti-TNF agents and the strategy of intraclass switching in a large US cohort of RA patients using the Consortium of Rheumatology Researchers of North America (CORRONA) registry. In particular, we sought to compare composite rates of drug response and remission outcomes as well as the persistence of anti-TNF treatment over a 2-year period.
Methods
Data source
The CORRONA registry is an independent prospective observational cohort of patients with arthritis who are enrolled by participating rheumatologists in both academic and private practice sites. As detailed previously,15 16 CORRONA is governed by a board of academically affiliated US rheumatologists. CORRONA has no governance or ownership ties to the pharmaceutical industry. CORRONA receives funding from multiple pharmaceutical manufacturers to support the registry.
CORRONA data collection began in 2002; data collected to 11 March 2008 are included in the current analyses. Up to 2008, there were 83 sites across 33 states in the USA, and approximately 200 rheumatologists have enrolled a total of 19 902 patients, including 16 696 with RA. Approximately 22% of the sites were academic sites and 78% were private sites. The geographical distribution of patients in the registry across the USA was the northeast region 34%, midwest region 24%, south region 28% and west region 14%. Patients were enrolled into the CORRONA registry at the time of a routine clinic visit. Enrolment into the CORRONA registry remains active. Both patient and physician questionnaires are filled out during routine clinical encounters. Completed questionnaires are faxed or mailed to a central processing site. Approvals for data collection and analyses were obtained for academic and private practice sites from local and central institutional review boards, respectively.
Study population
Among the 16 696 patients with RA enrolled in the CORRONA registry, 2530 were newly prescribed an anti-TNF agent with at least one follow-up visit between 4 February 2002 and 11 March 2008. No disease activity or comorbidity exclusion criteria were required for RA patients enrolled into the consortium registry. For the purposes of this study, the 162 RA patients in remission at baseline, defined by a clinical disease activity index (CDAI)17 score of 2.8 or less or a disease activity score based on 28 joints (DAS28) and erythrocyte sedimentation rate (ESR) less than 2.6 were excluded from the study population. Patients with a previous history of the use of a non-TNF agent (N=126) were also excluded, resulting in 2242 RA patients included in this analysis. Among these 2242 patients, 1475 were biologically naive, 616 were first switchers and 151 were switching to their second or more biological agent. A flowchart describing the study population in greater detail can be found in supplementary figure S1 (available online only).
Measures and data collection
Data were collected during the study period from physician assessment and patient questionnaires completed during clinical encounters. Patients were followed as frequently as every 3 months. For this dataset, the mean time between visits was 4.7 months and the median time between visits was 3.8 months. Non-biological and biological disease-modifying antirheumatic drugs (DMARD), including anti-TNF agents, were recorded at the time of the clinical encounter. Data elements also documented at the time of a clinical encounter that are relevant to the current analysis included 28 tender and swollen joint counts, physician and patient global assessments of disease activity, patient assessment of pain, the modified health assessment questionnaire (HAQ) assessing physical function and ESR. Across the 2242 patients, data on tender and swollen joint counts were complete in 2210 (98.6%) patients. All components of the CDAI were completed for 2069 (92.3%) patients. Acute phase reactant data were recorded from laboratory tests obtained within 10 days of the clinical encounter, but collection of laboratory data was not mandated by the registry protocol. ESR values were available for 1210 (54%) patients. Insurance data was available for 73.5% of patients. Completeness was high for data required for the CDAI (>92%).
Drug exposure cohorts
Patients initiating adalimumab, etanercept and infliximab were stratified into one of three cohorts. Biologically naive patients initiating an anti-TNF agent were defined as patients with no lifetime history of treatment with anakinra, other anti-TNF agents, abatacept or rituximab. First-time switchers were defined as patients initiating an anti-TNF agent with a history of previous treatment with a different anti-TNF agent. Second-time switchers were defined as patients with a history of previous treatment with two different anti-TNF agents. Within each of the three cohorts, comparisons among the three individual anti-TNF agents (adalimumab, etanercept and infliximab) were performed.
Registry outcomes
Responsiveness to anti-TNF therapy was assessed using the modified American College of Rheumatology (ACR) 20, 50 and 70 response criteria without the requirement for an acute phase reactant to maximise the amount of patient data available for analysis. These measures have been previously defined and validated.18 19 A modified ACR20 response required a 20% or greater improvement in tender and swollen joint counts, as well as in two or more of the following four ACR response components: physician global assessment, patient global assessment, patient global pain and modified HAQ. The modified ACR50 and 70 responses were calculated using the same criteria, but requiring at least 50% and 70% improvement, respectively. Disease remission outcomes were defined as a DAS28–ESR score less than 2.620 and a CDAI score, which does not require an acute phase reactant, of 2.8 or less.17 Continuation or persistence of treatment with the newly prescribed anti-TNF agent was defined as the duration of time from anti-TNF initiation to discontinuation.
Statistical analysis
Patient clinical and demographic characteristics were compared within the three strata of previous anti-TNF exposure by specific agent. For continuous measures, means and SD were estimated and analysis of variance was used to assess the statistical significance of any differences among the groups. For dichotomous measures, percentages were estimated and Fisher's exact test was used to assess the significance of differences among groups.
For modified ACR20, 50 and 70 response, patients who discontinued the newly prescribed anti-TNF agent were categorised as non-responders (ie, no modified ACR20 50 or 70 response or no DAS28–ESR or CDAI remission) for any study visit after discontinuation, using intention-to-treat analyses with non-responder imputation approach as previously applied.13 21 Unadjusted ACR response rates were determined at 6, 12 and 24 months following the start of the newly prescribed anti-TNF using 3-month time windows for capturing study visits. Unadjusted and adjusted OR comparing response rates among anti-TNF agents were estimated using multivariable logistic regression models and were reported with estimated 95% CI. Covariates associated with either anti-TNF agent selection or response to treatment were considered as possible confounders and included patient demographics, disease activity and severity measures, previous medication usage, history of comorbidities and years since anti-TNF agent initiation Sensitivity analyses were carried out applying a completer's analysis approach. Similar methodology was employed to assess remission based on the DAS28–ESR and CDAI cut points defined above.
Treatment persistence was estimated using survival analysis methods. Time from initiation to discontinuation of the anti-TNF or to last follow-up visit was estimated based on the initiation visit dates and discontinuation (or last follow-up) dates. Unadjusted Kaplan–Meier survival curves were estimated for each of the three study cohorts, as well as individually for anti-TNF agents within each cohort. Log rank tests were used to test the null hypothesis of no differences among the Kaplan–Meier survival curve estimates. Proportional hazard assumptions were assessed graphically by comparing survival curves estimated by Cox regression models and Kaplan–Meier estimates and by assessing the log–log survival plots. Cox proportional hazard regression models estimated unadjusted and adjusted HR of discontinuation.
For each of the study outcomes, comparisons were performed among the three cohorts (biologically naive, first-time switchers and second-time switchers), and among the three anti-TNF agents stratified within the biologically naive and first-time switcher cohorts. For the primary analysis of persistence, we used the visit dates of reported initiation and visit dates of reported discontinuation. An analysis was also carried out in which we used dates as described above for those who indicated starting or discontinuing ‘at the visit’ but for those indicating ‘since last visit’ we substituted the date halfway between visits with little change in results. Comparisons of the three anti-TNF agents among second-time switchers were not performed due to small sample sizes within this cohort. We also performed sensitivities that incorporated major changes in dose/frequency in the survival analyses and imputed non-response for major dose/frequency escalations. We distinguished high versus low dose/frequency for adalimumab as 40 mg weekly versus every 2 weeks, and for infliximab using the cutpoint of of greater than 6 mg/kg every 8 weeks or equivalent based on a previously published cutpoint.22
To allow comparison with other registries and RCT, crude response and remission rates were stratified on the basis of whether or not patients met the eligibility criteria from three major published controlled trials.12 As the registry records 28-joint counts, we estimated 28-joint count equivalents for the RCT 66-joint count requirements based on the 28-joint validation methodology previously described.12 For the 66-joint count threshold of six or more tender and swollen joints, we applied the estimated 28-joint count equivalent of four of more joints such that patients who were deemed RCT eligible had four or more swollen joints, four or more tender joints and 45 min or more of morning stiffness at the time of registry enrollment. Power calculations varied across study outcomes for 6-month modified ACR outcomes. In biologically naive patients, we had 93% power to detect an OR of 2.0. For DAS28 remission at 6 months we had 76% power to detect an OR of 2.25.
Results
Demographic and clinical characteristics
The study population consisted of 2242 RA patients; 1475 patients were biologically naive before initiating anti-TNF therapy, 616 had switched to a second anti-TNF agent (termed ‘first-time switchers’) and 151 had switched to their third anti-TNF agent (termed ‘second-time switchers’). The baseline characteristics based on anti-TNF agent among the biologically naive and first-time switchers are displayed in table 1. Infliximab users were more likely to be older and have Medicare insurance compared with the other biologically naive patients. Among first-time switchers, adalimumab users were more likely to be disabled and were exposed to a greater number of previous DMARD. Among the second time switchers (adalimumab n=103, etanercept n=21 and infliximab n=27), users of etanercept were more likely to be women (data not shown). When examining patients based on overall switching status and not by specific agent, disease duration and the number of previous DMARD, both increased as the number of anti-TNF switches increased. Similarly, higher (worse) modified HAQ, patient global and patient pain scores, and larger proportions of patients reporting disability were observed with more anti-TNF switches. Of note, the overall mean DAS28–ESR (4.5) and CDAI (21.5) scores were within the defined ranges of moderate disease activity levels (data not shown).
Baseline characteristics of the study cohort stratified by previous exposure to anti-TNF and newly prescribed anti-TNF agent
Anti-TNF treatment
The median dose of infliximab, exclusive of the loading protocol, was 5.5 mg/kg every 8 weeks in biologically naive patients, 5.6 mg/kg every 8 weeks in first-time switchers and 7.1 mg/kg every 8 weeks in second-time switchers. The majority of patients prescribed adalimumab received 40 mg every other week (86.5% of biologically naive patients, 75.4% of first-time switchers and 53.7% of second-time switchers). Among patients prescribed etanercept, dose escalation information was not collected because the two approved dosing options (ie, 25 mg twice weekly and 50 mg once weekly) are considered equivalent.
Response and remission rates by newly prescribed anti-TNF agent
Achievement of modified ACR20 occurred in 26.8–35.4% of biologically naive anti-TNF users at 6 months (table 2). At 12 months the rates were 26.7–32.4%. Response rates using the modified ACR50 and modified ACR70 were 15.0–26.5% and 10.0–12.3%, respectively. In adjusted analyses, the likelihood of achieving modified ACR20, 50 or 70 response outcomes was not significantly different among the three anti-TNF agents in biologically naive patients (table 2). Also in biologically naive patients, remission rates based on the CDAI were 15.1–16.6% at 6 months and 12.8–20.7% at 12 months. DAS28 remission rates were slightly higher (23.2–27.1% at 6 months and 27.8–32.1% at 12 months). Within the biologically naive patients, no differences in the likelihood of achieving remission among specific anti-TNF agents were observed using the CDAI and DAS28 remission definitions (table 2). Similar patterns of response and remission were observed in first-time switchers (see supplementary table S1, available online only). Response and remission results at 24 months were consistent in both biologically naive patients and first-time switchers (data not shown). For the modified ACR20/50/70 outcomes, as well as the DAS28/CDAI remission outcomes, consideration of dose/frequency escalation as ‘non-responders’ as a secondary analysis failed to demonstrate any consistent patterns in biologically naive patients across the three anti-TNF agents (table 3).
Crude response and remission rates at 6 and 12 months among adalimumab, etanercept and infliximab users in those who were biologically naive
Secondary analysis of response and remission rates in biologically naive patients: dose escalation imputed as non-response
Unadjusted response and remission rates by switching status
In the full study cohort without any stratification by disease activity, achievement of a modified ACR20 response occurred in 30.5%, 28.5% and 23.4% of biologically naive patients at 6, 12 and 24 months, respectively (table 4). Respective modified ACR20 response rates were 19.9%, 14.7% and 13.9% in first-time switchers and 17.3%, 18.7% and 15.7% in second-time switchers. The modified ACR 50 and modified ACR70 response rates were similarly higher in biologically naive patients than in both first and second-time anti-TNF switchers. Lower remission rates were also observed among anti-TNF switchers versus biologically naive patients for both DAS28–ESR and CDAI remission (table 4).
Unadjusted response and remission rates and adjusted likelihoods of achieving response/remission over time stratified by anti-TNF switch status
Adjusted response and remission comparisons based on switching status
After adjustment for differences in baseline characteristics, the likelihood of achieving a modified ACR20, 50 or 70 response was consistently reduced in first-time switchers versus biologically naive patients at 6, 12 and 24 months (table 4). For example, using biologically naive patients as the reference group, the adjusted OR for first-time switchers in achieving a modified ACR20 response was 0.54 (95% CI 0.38 to 0.76) at 6 months, 0.44 (95% CI 0.30 to 0.66) at 12 months and 0.54 (95% CI 0.31 to 0.93) at 24 months. For second-time switchers, a reduced likelihood of response was also observed, although CI crossed unity at some time points.
A similar pattern of response was observed for clinical remission (table 4). At 6 months, the adjusted OR for achieving DAS28–ESR remission was 0.21 (95% CI 0.08 to 0.56) for first-time switchers and 0.29 (95% CI 0.07 to 1.22) for second-time switchers versus biologically naive patients.
Similarly, using the CDAI remission definition, first-time switchers (OR 0.57, 95% CI 0.36 to 0.90) and second-time switchers (OR 0.09, 95% CI 0.01 to 0.71) were significantly less likely to achieve remission when compared with biologically naive patients at 6 months (table 4). Reduced likelihoods of achieving DAS28–ESR and CDAI remissions were also observed at 12 and 24 months, although with wider CI. Sensitivity analyses applying a completer's analysis approach instead of non-responder imputation yielded comparable results (data not shown).
Persistence of treatment with newly prescribed anti-TNF
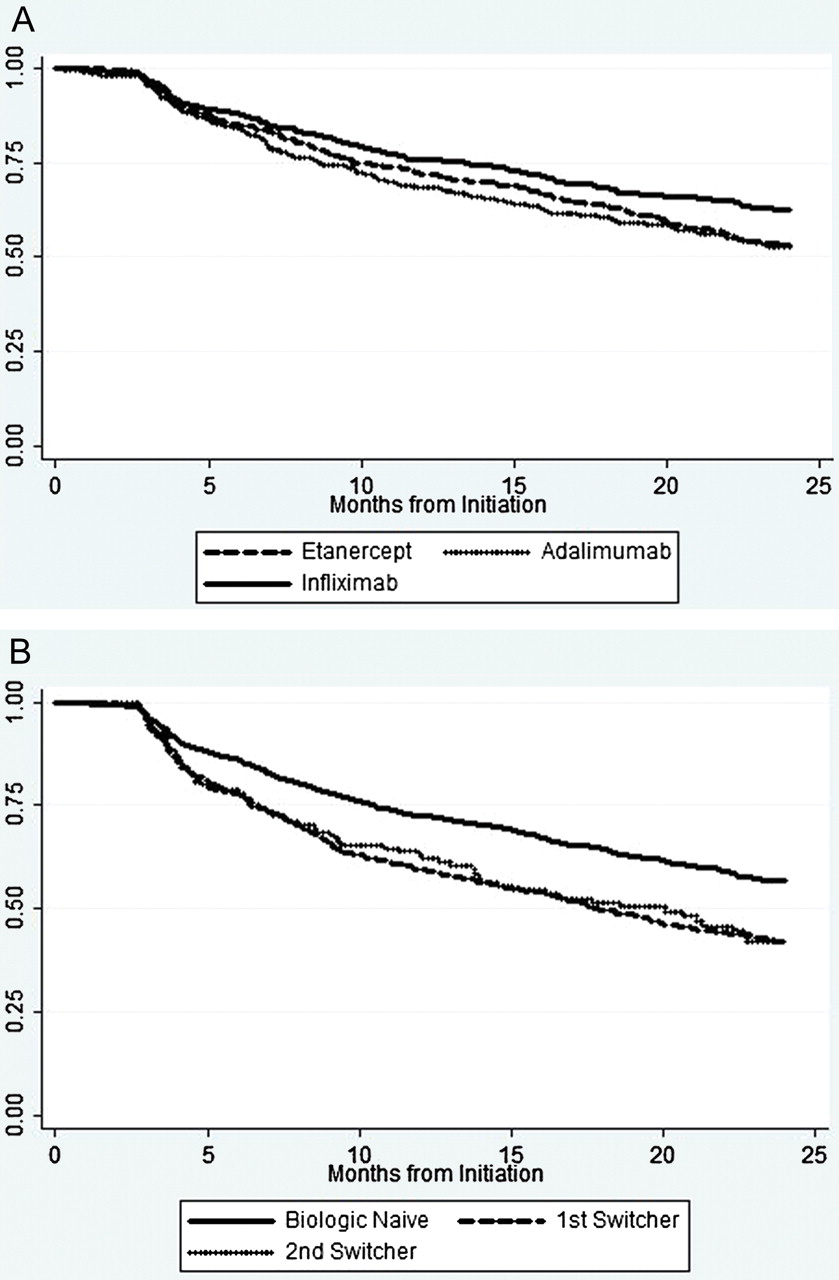
Based on Kaplan–Meier curve estimates (figure 1A,B), the proportions of biologically naive patients with persistence of the new anti-TNF treatment to 12 and 24 months were 76% and 63%, respectively, with infliximab versus 72% and 53% with etanercept, and 68% and 53% with adalimumab (table 5). In adjusted analyses, discontinuation was more likely in biologically naive patients receiving adalimumab (OR 1.42, 95% CI 1.12 to 1.80) or etanercept (OR 1.27, 95% CI 1.00 to 1.61) versus infliximab. Additional modelling to address dosing titration suggestive of incomplete response was performed, and examined time to drug discontinuation or dose/frequency escalation. These models demonstrated a different pattern. Relative to infliximab (HR 1.0) among biologially naive patients, the HR for discontinuation/dose escalation for etanercept was 0.77 (95% CI 0.63 to 0.96) and for adalimumab 1.11 (95% CI 0.90 to 1.37), reflecting the impact of dose/frequency escalation. No differences among the three agents were observed among first-time switchers (table 5). As demonstrated in figure 1B, patients who switched drugs remained on their anti-TNF agent for shorter time periods than biologically naive patients.

{kind=link}
Drug persistency for (A) specific anti-TNF agents in biologically naïve patients and (B) biologically naïve patients versus those switched to anti-TNF agents. TNF, tumour necrosis factor.
The unadjusted persistence rates and adjusted likelihood of drug discontinuation based on anti-TNFα switching status*
Patients meeting commonly applied RCT eligibility criteria
Response and remission rates differed based on disease activity (see supplementary table S2, available online only). Among patients who met three commonly applied RCT eligibility criteria for enrollment in RCT, modified ACR20 response rates were higher at all time points (43.8%, 38.2% and 30.6% at 6, 12 and 24 months) compared with respective rates in patients who had less severe disease and were thus not RCT eligible (19.1%, 17.1% and 15.2%). Consistent stratification patterns were observed for modified ACR50 and modified ACR70 response rates (see supplementary table S2, available online only). Conversely, RCT-ineligible patients (ie, those with lower disease activity) were more likely to achieve CDAI remission (14.0%, 14.0% and 12.8% at months 6, 12 and 24) than the RCT-eligible patients with more active disease (10.9%, 10.4% and 11.4% at months 6, 12 and 24). Similar findings were observed using the DAS28–ESR remission criteria (data not shown).
Discussion
In this large US registry study, the majority of RA patients prescribed anti-TNF agents had low or moderate disease activity, demonstrating markedly lower disease activity than previously reported in the pivotal anti-TNF RCT and European registries.3 4 23 For both biologically naive and switched patients, we observed no differences in drug response or remission outcomes among adalimumab, etanercept and infliximab users. However, the likelihood of achieving both response and remission outcomes were consistently greater for biologically naive patients than anti-TNF switchers. Persistence was noted to be higher for biologically naive patients, with the highest persistence noted for infliximab users. These comparative effectiveness results derived from a multi-centred US registry differ from the results reported in two large European registries.3 4
The dosing patterns in our US-based registry were different than dosing patterns reported in the European registries. In particular, the dose of infliximab was approximately 3.5 mg/kg in the Danish registry and 3 mg/kg in the Dutch registry, whereas the mean dose was approximately 5.5 mg/kg in our study.3 4 Similarly, dose escalation from adalimumab 40 mg every 2 weeks to weekly was more common in our US registry than European registries. These dosing differences further emphasise the potential limitations of applying the results of European-based registry results to RA patients in the USA21 and vice versa. In particular, this difference in dose escalation of infliximab, and possibly also adalimumab, may explain the conflicting comparative effectiveness results from our US registry and the two European registry studies.3 4
In fact, our study results are consistent with the two published RCT meta-analyses, concluding that there was no difference in the efficacy among the three anti-TNF drugs. However, these meta-analyses have been criticised for lacking statistical power and for including study arms of infliximab with drug dosages not frequently prescribed, especially in European countries.1,–,4 The Dutch Rheumatoid Arthritis Monitoring (DREAM) register reported significantly greater reductions in DAS28 and HAQ–DI for both adalimumab and etanercept versus infliximab.4 These findings were further supported by the nationwide Danish Biologics (DANBIO) registry, in which patients receiving either adalimumab or etanercept were more likely to achieve a ACR50, ACR70 and European League Against Rheumatism (EULAR) moderate/good response than patients prescribed infliximab.3 In both studies, drug persistence was also lowest for infliximab. However, as previously noted, the median dosage and frequency of administration of infliximab in these two studies were markedly different from our experience in the US-based CORRONA registry. Alternatively, we may have failed to detect a difference due to a type II error. Therefore, these important differences may partly explain differences in study results derived from US registries, European registries and RCT.
The effectiveness of anti-TNF switching for incomplete responders to a first anti-TNF agent has also been examined primarily in European studies. Investigators using the South Swedish Arthritis Treatment Group (SSATG) register examined drug responsiveness and remission outcomes in patients receiving their second or third anti-TNF agent, and found diminished ACR response and DAS28 remission rates in patients who switched versus first-time users.8 The largest published study of treatment response among anti-TNF switchers was the European-based open-label clinical trial of adalimumab, the Research in Active Rheumatoid Arthritis (ReAct) trial.24 Among patients who had a history of treatment with etanercept and/or infliximab, use of adalimumab resulted in robust ACR response and remission rates, but these proportions were lower among adalimumab-treated patients who switched. A recent systematic review, based primarily on a small number of European registry studies, concluded that responses to a subsequent anti-TNF agent were diminished when the switch was due to lack of efficacy.25 To our knowledge, no comparative effectiveness studies from US registries have been published for anti-TNF switching in RA patients.
Drug persistence studies of anti-TNF agents in RA patients have also been published, and may be the outcome measure most strongly influenced by a nation's healthcare system and drug access policies. Persistence has been reported as a surrogate measure of drug effectiveness, but is also influenced by tolerability, toxicity, cost and relative availability. When comparing persistence across individual agents, investigators using the German biological agent registry as well as the British Society for Rheumatology Biologics Register in the UK did not find differences in persistence among the three anti-TNF agents.6 26 In contrast, the DANBIO and DREAM registries, as well as a Swedish registry, observed that the risk of discontinuation was higher for infliximab users than adalimumab or etanercept users.27 In contrast, the results from a recent study from a US administrative claims database were consistent with our study, showing higher persistence rates for infliximab as combination therapy with methotrexate.28 Similar to our study, another US study reported that dose escalation is frequently prescribed in US patients with RA treated with infliximab.29 Our results are also consistent with earlier studies demonstrating reduced drug persistence among anti-TNF switchers versus first time users.30
In contrast to multiple European registry studies, we observed that the disease activity level on anti-TNF initiation in our US-based registry was substantially lower. The majority of both biologically naive and anti-TNF switched patients had low or moderate disease activity at baseline before anti-TNF initiation. In contrast, the mean baseline disease activity (DAS28) in various European RA biological agent registries are consistently greater than 5.1.3,–,7 23 31 In fact, these baseline characteristics in the European registries more closely resemble RA patients enrolled in anti-TNF RCT. As demonstrated in our study, drug response is strongly influenced by the disease activity eligibility criteria routinely applied in RCT. These differences in patient characteristics and dosing patterns between European and US-based RA populations prescribed biological agents may in fact influence comparative effectiveness results, reinforcing the complementary importance of both US and European registries.23
Our study has numerous strengths. This study represents one of the largest comparative effectiveness studies of specific anti-TNF agents and anti-TNF switching, derived from a large US-based registry of RA patients with physician-derived outcome measures. We examined three different outcome domains—drug response, remission achievement and persistence on drug—to develop an integrated assessment of drug utilisation and effectiveness of specific anti-TNF agents as well as anti-TNF switching. This work focused on the ‘real world’ effectiveness of agents in US patients, who are markedly different to RCT subjects in terms of comorbidities and RA disease activity.12 Our study complements the reports from European registries with improved generalisability to US-based RA patients with lower disease activity and greater access to biological agents. Finally, we were able to examine and adjust for clinical factors that influenced drug response, remission achievement and persistence, as the CORRONA registry prospectively collects these data from the treating rheumatologist at the time of the office visit.
This study also has limitations. Unlike RCT, the timing of the study visits was based on clinic visits, and was requested at intervals of approximately 3 months. Nevertheless, the mean study interval between study visits was approximately 4.5 months, which compares favourably with the intervals reported from the majority of RA registries. In addition, acute phase reactant data were not available for all patients in the study. As a result, we applied previously validated outcome measures not requiring acute phase reactants such as modified ACR outcomes and CDAI remission definition.17 In fact, the CDAI has recently been shown to be less influenced than the DAS28 by changes in ESR in the normal range, which can inflate remission rates.32 Finally, given the modest representation of the CORRONA registry relative to the entire US population of RA patients prescribed anti-TNF, there are limitations to the generalisability of our findings.
In conclusion, the results of this US-based study indicate that similar rates of drug response and remission were achieved across the three anti-TNF agents, with more robust effectiveness consistently observed for those who were biologically naive versus patients who switched therapies. Moreover, biologically naive patients prescribed anti-TNF had higher persistence as compared with switchers. Among biologically naive patients, infliximab was associated with greater persistence than the other two agents. Additional comparative effectiveness studies are required to determine if switching to another biological class with a different mechanism of action would improve outcomes compared with intraclass switching strategies. Given the marked differences in disease activity and severity among patients initiating biological agents in the USA versus various European countries, comparative effectiveness studies from both populations are needed to inform their respective patient populations.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Funding Within the previous 2 years, Abbott, Amgen, BMS, Centocor, Genentech, Lilly and Roche have supported CORRONA through contracted subscriptions to the database. Centocor, as part of its subscription contract, proposed the current research study and was involved in the early design, as well as manuscript review and comment for this study. The final analysis plan, the study results and interpretations of the study data were those of the non-Centocor authors. The manuscript was written by the first author with content and editorial input from all co-authors.
-
Competing interests JG receives salary support from research grants from the National Institutes of Health (NIH) (K23AR054412), the Arthritis Foundation and the Arthritis National Research Foundation. He serves as chief scientific officer for CORRONA and has served on advisory boards for Centocor, Genentech, and UCB. GR has a research contract with CORRONA. DD is an employee of Janssen Services LLC. LH was supported by grant no K23AR053856 from the National Institute of Arthritis and Musculoskeletal and Skin Diseases. DF receives funding from Abbott, Actelion, Amgen, BMS, BiogenIdec, Centocor, Corrona, Genentech, Gilead, GSK, Human Genome Sciences, Merck, NIH, Nitec, Novartis, Roche, UCB, Wyeth and Xoma. He also serves as director of publications for CORRONA. AG is executive vice president of CORRONA. He is a consultant to Abbott, Amgen, Nicox, Pfizer, Roche, Savient, Takeida and UCB. He is a speaker for Abbott, Amgen, BMS, Pfizer and Roche. In addition, he and/or his spouse are stockholders in Abbott, Amgen, BMS, J&J and Pfizer. RDH is an employee of Centocor Ortho Biotech Services LLP. MK has no competing interests. JMK receives research support from Amgen, Abbott, Centocor, BMS, Genentech, HGS, Pfizer, Roche and UCB as well as honoraria from Abbott, Centocor, BMS, Roche and Genentech.
-
Ethics approval Approvals for data collection and analyses were obtained for academic and private practice sites from local and central institutional review boards, respectively.
-
Provenance and peer review Not commissioned; externally peer reviewed.