Article Text

Abstract
Background Necroscopic and surgical studies have suggested that giant cell arteritis (GCA) may target the aorta and its main branches. Imaging techniques are able to detect large vessel vasculitis (LVV) non-invasively in patients, but the prevalence of LVV in GCA has not been clearly established.
Objective To assess prospectively the prevalence, characteristics and topography of LVV in patients with newly diagnosed GCA and to determine the associated clinical and laboratory features.
Methods CT angiography (CTA) was performed in 40 consecutive patients with newly diagnosed biopsy-proven GCA. Patients were treatment-naïve or had been treated with corticosteroids for <3 days. Vessel wall thickness and vessel diameter (dilation or stenoses) at four aortic segments (ascending aorta, aortic arch, descending thoracic and abdominal aorta) and at the main aortic branches were evaluated.
Results LVV was detected in 27 patients (67.5%). The vessels involved were as follows: aorta (26 patients, 65%), brachiocephalic trunk (19 patients, 47.5%), carotid arteries (14 patients, 35%), subclavian arteries (17 patients, 42.5%), axillary arteries (7 patients, 17.5%), splanchnic arteries (9 patients, 22.5%), renal arteries (3 patients, 7.5%), iliac arteries (6 patients, 15%) and femoral arteries (11 patients, 30%). Dilation of the thoracic aorta was already present in 6 patients (15%). Cranial ischaemic events were significantly less frequent in patients with LVV (p=0.029). Treatment-naïve patients had a higher frequency of LVV (77% vs 29%, p=0.005).
Conclusions CTA-defined LVV occurs in two-thirds of patients with GCA at the time of diagnosis and aortic dilation is already present in 15%. Previous corticosteroid treatment may decrease CTA-detected LVV.
Statistics from Altmetric.com
Introduction
Giant cell arteritis (GCA) was originally characterised as a granulomatous arteritis involving the carotid artery branches, particularly the superficial temporal arteries. Classic clinical symptoms (headache, jaw claudication, scalp tenderness and visual impairment) are related to the marked cranial tropism of GCA.1 2
Involvement of the extracranial arteries, particularly the aorta and its main tributaries, was first recognised in the late 1930s and sporadically reported thereafter in case reports or retrospective series investigating necropsy or surgical specimens.3,–,10 The clinical relevance of this finding was dismissed until, in a retrospective study, Evans et al reported an increased prevalence of aortic aneurysm in patients with GCA compared with the general population, particularly in the thoracic aorta.11 Subsequent retrospective surveys over extended periods of time (20–50 years) confirmed that aortic aneurysm occurs in 9.5–18% of patients.12,–,15 A recent prospective screening of 54 patients demonstrated aortic dilation in 12 (22.5%) of patients after a median follow-up of 5.4 years.16 Although aortic inflammation is usually asymptomatic, it may lead to delayed dilation with potentially life-threatening complications such as dissection or rupture.15
The prevalence of aortic inflammation in unselected individuals with GCA is not well known. In a systematic necropsy study of 13 patients with GCA, large vessel inflammation (aorta and its main branches) was observed in more than 90% of patients.17 Although the necroscopic nature of this study may generate bias to severity, these findings indicate that large vessel inflammation in GCA might be more frequent than anticipated.
The improving resolution of imaging techniques has facilitated the evaluation of inner vascular territories in patients. CT angiography (CTA), magnetic resonance angiography and18fluorodeoxyglucose-positron emission tomography (FDG-PET) are able to reveal abnormalities highly suggestive of aortic inflammation, as repeatedly published in case reports, small series or retrospective studies.18,–,23 Only two previous studies have tried to assess prospectively the prevalence of aortic involvement at early disease stages in cohorts of more than 20 patients. In the first study, FDG-PET revealed aortic FDG uptake in 51% (thoracic) and 54% (abdominal) of 35 patients. In the second study, helicoidal CT showed aortic thickening in 45.4% of a series of 22 cases.24 25
Symptomatic stenoses of the primary branches of the aorta or more distal arteries have occasionally been reported in single cases or small series but are considered infrequent complications of GCA.26,–,31 Symptomatic vascular stenoses appear to occur less frequently in GCA than in Takayasu arteritis, although this may be influenced by reduced physical activity of elderly individuals, limited lifespan or difficulties in differentiating arteritis complications from atherosclerotic disease. The prevalence of aortic branch inflammation during active disease has not been clearly determined. Only a few prospective studies have analysed aortic branch involvement using FDG-PET or colour duplex ultrasonography (DUS). Frequency ranges from 30% to 74% of patients depending on the vascular territory explored and the technique employed (summarised in table S1 in online supplement).25 32,–,34
In this study we prospectively assessed large vessel involvement in 40 consecutive patients with newly diagnosed GCA using CTA. The aims of this survey were (1) to investigate the prevalence, topography and characteristics of large vessel inflammation and (2) to determine clinical or analytical features associated with large vessel involvement.
Methods
Patients
All patients diagnosed with biopsy-proven GCA at the Hospital Clínic of Barcelona between November 2006 and March 2011 were evaluated for their potential participation in the study. The inclusion criteria were (1) newly diagnosed biopsy-proven GCA; (2) fulfilment of at least three American College of Rheumatology classification criteria for GCA; and (3) signed informed consent. Exclusion criteria included (1) allergy to iodinated contrast; (2) lack of consent to participate in the study; (3) creatinine clearance <30 ml/min; and (4) treatment with corticosteroids for >3 days at the time of evaluation.
The control group included 32 patients with no chronic inflammatory diseases matched for gender, age (mean 79 years, range 57–89) and traditional cardiovascular risk factors, consecutively selected from patients who underwent CTA during the same time-frame for cancer staging.
Clinical and exploratory findings prospectively recorded at the time of diagnosis were: cranial symptoms (headache, jaw claudication, scalp tenderness), polymyalgia rheumatica, systemic symptoms (weight loss, fever), disease-related cranial ischaemic complications, vascular murmurs, peripheral pulses, bilateral arm blood pressure and presence of extremity claudication. C reactive protein, erythrocyte sedimentation rate, platelet count, haemoglobin and haptoglobin were determined by laboratory automatic systems. Interleukin 6 (IL-6) and tumour necrosis factor α were determined by immunoassay.
Aortic CTA protocol
Aortic CTA was performed at the Centre for Diagnostic Imaging (Hospital Clínic, Barcelona) using two multislice spiral CT scanners (Somatom Sensation 64 and Somatom Definition Flash, Siemens Medical Solutions, Malvern PA, USA)with the following scanning conditions: collimation 0.6 mm, 120 kV, mAs determined by automatic modulation dose and reconstruction slice thickness of 5.0 and 1 mm. 100 ml of non-ionic contrast agent (370 mg I/ml) was injected through the antecubital vein using a power injector at the rate of 4 ml/s. Early arterial and venous scans phases were acquired. We used the bolus-tracking method at the descending aorta level and set 100 HU as the triggering threshold for the arterial phase. The venous phase scan was taken 50 s after finishing the arterial phase.
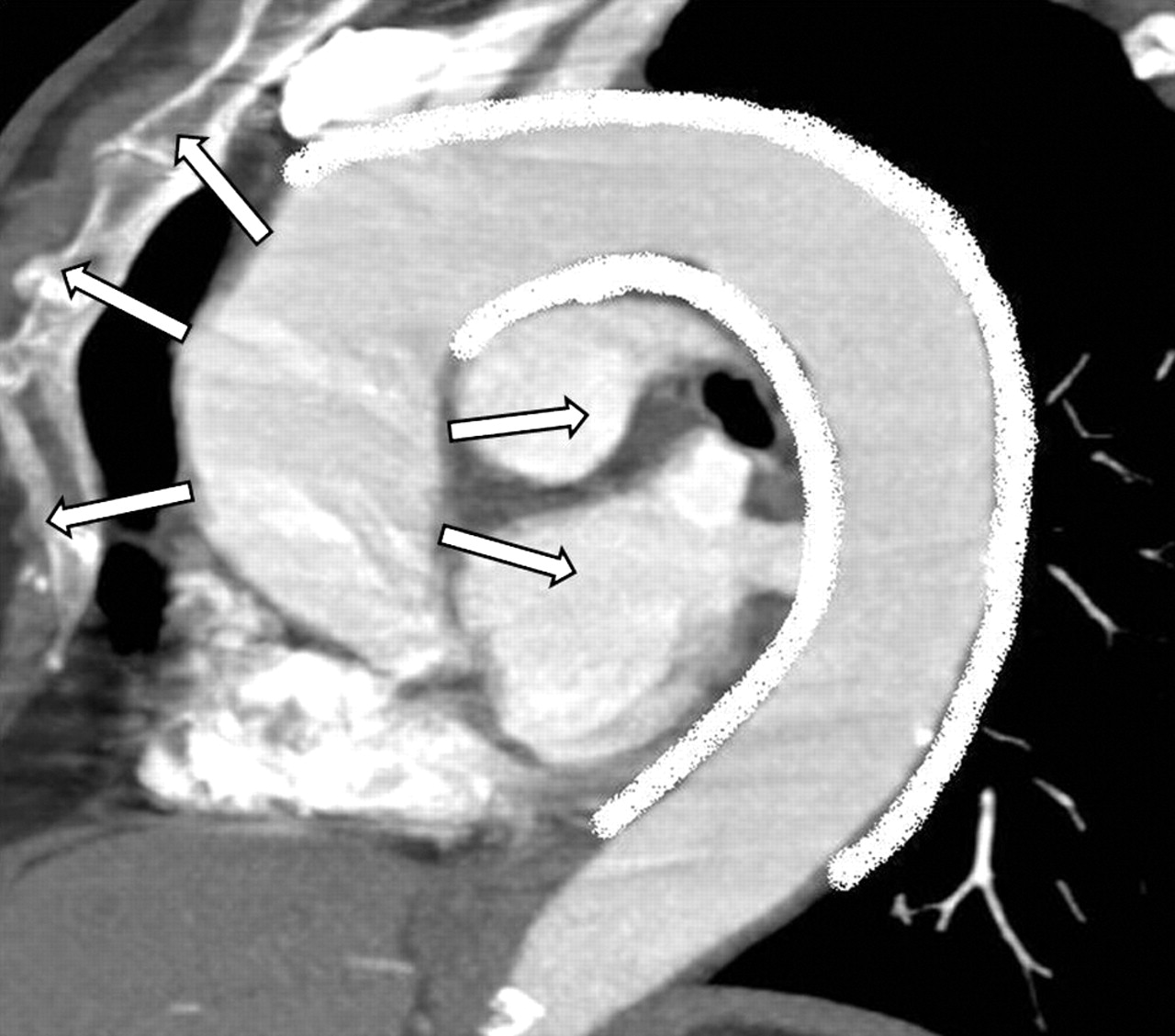
Aortic thickening suggestive of aortitis and aortic dilation were the pathological findings recorded. Aortitis was defined as circumferential aortic wall thickness ≥2 mm with or without contrast enhancement of the vessel wall observed in zones without adjacent atheroma (figure 1). Aortitis was considered possible when aortic thickening ≥2 mm was not concentric.

(A) CT angiography (CTA) image of the descending thoracic aorta (DTA) showing circumferential thickening of the vessel wall (arrows). (B) Late venous phase CTA image of the DTA showing contrast enhancement on the peripheral aortic wall layers (white arrow) but not in the intimal layer (black arrow). (C) CTA image showing a normal DTA vessel wall (control patient).
Four aortic segments (ascending thoracic aorta, aortic arch, descending thoracic aorta and abdominal aorta) were evaluated. Measurements were taken at the middle third of the ascending aorta, the distal portion of the aortic arch and the middle third of the descending thoracic aorta. The abdominal aorta was measured below the renal arteries.
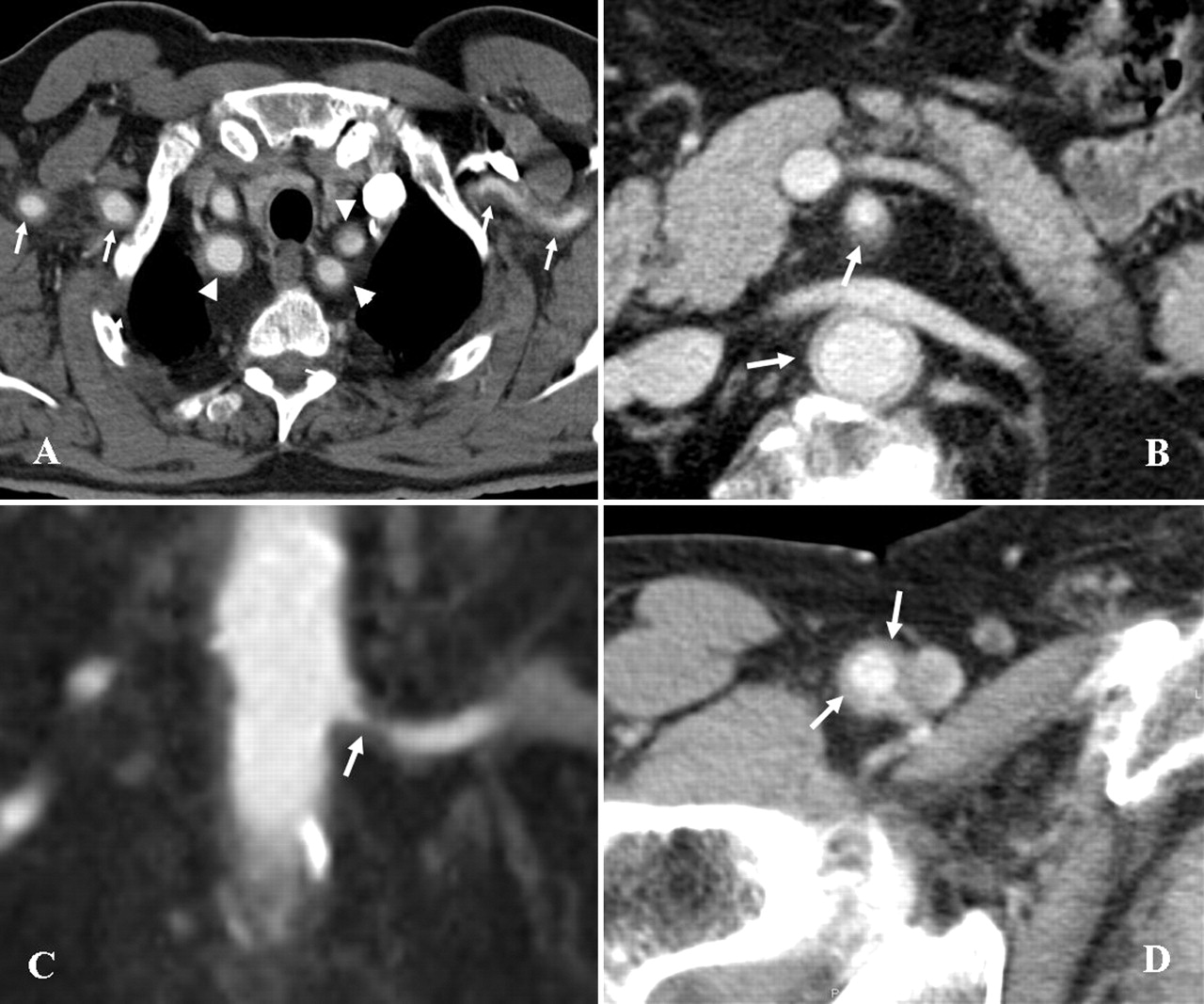
The aortic tributaries including the brachiocephalic trunk, carotid, subclavian, axillary, splanchnic (coeliac and mesenteric), renal, iliac and femoral arteries were also evaluated. Radiological findings considered included circumferential wall thickness, contrast enhancement of the artery wall, arterial diameter and the presence of stenoses. Arteritis was considered to be present when the thickness of the artery wall was >1 mm (figure 2).

(A) CT angiography (CTA) image showing vessel wall thickening of the axillary arteries (arrows) and supra-aortic trunks (arrow heads). (B) CTA image showing circumferential contrast enhancement and thickening of the aortic and superior mesenteric artery walls. (C) CTA image of thickening of the left renal artery wall causing lumen stenosis. (D) CTA image of the right femoral artery showing vessel wall thickening.
Aortic dilation was defined by a diameter of >4 cm in the ascending aorta, ≥4 cm in the rest of the thoracic aorta and ≥3 cm in the abdominal aorta.35 36 Loss of physiological progressive diameter reduction of the aorta was also considered as dilation.35 36 Abnormal dilation of the aortic branches was considered when aneurysm formation was detected or when the physiological progressive reduction of the diameter was not observed.
CTA assessment and measurements were performed by the same radiologists (PA and MS) who were blinded to the diagnosis. Interobserver agreement was 97.5%. After discussion, consensus was achieved in 100% of cases.
Statistical analysis
The Mann–Whitney U test and Student t test, when applicable, were used for quantitative data. The Fisher exact test was applied to contingency tables. Bonferroni correction was applied to multiple comparisons within each category of variables.
Results
Clinical and laboratory findings
During the recruitment period, 71 patients were diagnosed with biopsy-proven GCA. Thirty-one patients had exclusion criteria (4 had allergy to iodinated contrast, 5 refused participation and 22 had received corticosteroid treatment for >3 days), so 40 patients (27 women and 13 men, 2:1 gender ratio) were included in the final analysis. The mean age was 79 years (range 57–92 years). Twenty-two patients were evaluated before the initiation of glucocorticoid treatment and 18 patients had been treated for ≤3 days at the time of imaging. Initial treatment consisted of prednisone 1 mg/kg/day (up to 60 mg/day) in 12 patients and intravenous methylprednisolone megadoses (250 mg/6 h) in six patients because of visual symptoms. The mean glucocorticoid dose received at the time of imaging was 120 mg (range 60–1120). The clinical data and laboratory results at diagnosis are summarised in table S2 in the online supplement.
Prevalence, characteristics and topography of large vessel involvement
Thirty-four of the 40 patients (80%) had abnormal CTA including aortitis (defined or possible), aortic dilation or inflammation of the aortic branches. Defined large vessel vasculitis (LVV) (including the aorta and/or any tributary) was detected in 27 patients (67.5%). No dilation was observed in the aortic branches.
Aortic involvement (aortitis and/or dilation) was present in 28 patients (70%). Defined aortitis was seen in 26 (65%). In seven additional patients, aortitis was considered possible because the aortic wall focally reached a thickness of ≥2 mm, but this was not concentric. The descending aorta and aortic arch were the areas more frequently affected. These were concomitantly involved in 23 patients (88% of those with defined aortitis). Aortitis in the ascending aorta was observed in only 12 patients (46% of those with defined aortitis). Inflammation of the abdominal aorta was observed in 19 patients (73% of those with defined aortitis) (table 1). Interestingly, all patients with aortitis in the abdominal aorta also had thoracic aortic involvement. Ten patients had panaortitis and only two patients had involvement of a single aortic segment. Detailed frequencies of defined aortitis in the various aortic segments and distribution of aortic involvement in individual patients are summarised in table 1 and in figure S1 in the online supplement, respectively.
Topography of large vessel involvement in the study cohort
Aortic dilation was found at the time of diagnosis in six patients (15%). It was restricted to the thoracic aorta, mainly in the ascending segment or the aortic arch. Five of them had both aortitis and dilation, but only in three patients were dilation and aortitis co-localised (see figure S1 in online supplement).
Only one of the matched controls showed radiological signs suggestive of aortitis in the descending thoracic aorta. This patient was subsequently assessed and had no clinical or laboratory features suggestive of systemic vasculitis. None of the controls had significant aortic dilation, but in three of them the descending thoracic aorta did not undergo physiological diameter reduction. Atherosclerotic lesions were similarly present in patients and controls.
Differences in the thickness of the aortic wall between patients and controls were statistically significant (table 2).
Aortic wall thickness and aortic diameter in patients with giant cell arteritis and controls
The aorta, brachiocephalic trunk, subclavian, carotid, axillary and renal arteries and splanchnic territory were assessed in all patients while the iliac and femoral arteries were evaluated in 39 and 36 patients, respectively. Acquired images of the iliac or femoral arteries did not reach the standards required for accurate evaluation in the remaining patients. CTA-defined aortic branch inflammation could be detected in 23 patients (57.5%) and was less frequent than aortitis. The brachiocephalic trunk, subclavian and carotid arteries were the most frequently involved aortic tributaries. Detailed frequencies of aortic branch involvement are summarised in table 1. None of the patients had signs or symptoms derived from aortic branch inflammation. No aortic branch abnormalities were observed in controls.
Clinical or laboratory features associated with large vessel inflammation.
The main clinical and laboratory findings of the study cohort according to the presence of LVV are summarised in table 3. For comparison purposes, a subcategory of widespread LVV was created. This defined individuals with involvement of three or more of the following vascular territories: ascending thoracic aorta and/or aortic arch, descending thoracic aorta, abdominal aorta, subclavian and carotid arteries, iliac and/or femoral arteries.
Clinical and laboratory findings in patients with giant cell arteritis with and without large vessel vasculitis (LVV)
No significant differences in age or gender were found between patients with or without LVV. The duration of disease symptoms until diagnosis was significantly more prolonged in patients with widespread LVV than in the remaining patients. Cranial ischaemic events, particularly ocular manifestations, were less frequent in patients with LVV. No differences in other classic GCA manifestations were observed. Interestingly, CTA signs of LVV were more frequent among treatment-naïve patients (table 3).
Traditional cardiovascular risk factors did not differ among patients with or without LVV, except for dyslipidaemia which tended to be less frequent in patients with widespread LVV. Statin or aspirin intake was less frequent among the subset of patients with widespread LVV.
Interestingly, early aortic dilation was significantly more frequent in men than in women (5 vs 1, p=0.01), as previously observed for patients with GCA after long-term follow-up.16 No differences in cardiovascular risk factors were apparent in patients with or without dilation (data not shown).
Discussion
This is the first study to assess prospectively the prevalence, topography and characteristics of CTA findings suggestive of large vessel inflammation in a sizeable series of 40 newly diagnosed patients with biopsy-proven active GCA. Overall, CTA-defined large vessel arteritis was found in 67.5% of patients, mainly affecting the aorta (65% of patients) but also its main tributaries (57.5%). The thoracic aorta (especially the aortic arch and descending thoracic aorta) and the supra-aortic arteries were the territories most frequently involved.
The prevalence of aortitis was higher in our series than in the two previously published prospective studies using FDG-PET and helicoidal CT, respectively (see table S1 in online supplement).24 25 CTA may be more sensitive than FDG-PET for detecting signs suggestive of aortitis, and has additional advantages including the ability to detect structural abnormalities such as stenosis or dilation. In fact, aortic dilation exclusively involving the thoracic aorta was already observed in 15% of our patients. Moreover, CTA is able to detect atheroma plaques which are frequent in the aorta, iliac and femoral arteries of elderly individuals. Atherosclerosis may have an inflammatory component which may be difficult to distinguish from vasculitis by FDG-PET, as previously recognised.37 Accordingly, and contrary to our findings, the study by Blockmans et al25 found a slightly higher prevalence of FDG uptake in the abdominal aorta where atherosclerotic involvement is more frequent compared with the thoracic segment.
The prevalence of aortitis in our study was also higher than that reported by Agard et al using helicoidal CT, in spite of the fact that we used a more stringent definition of aortitis.24 Several reasons may account for this difference. The study by Agard et al was performed 10 years before its publication when CT imaging was not so well developed and was less accurate. Moreover, the study allowed inclusion of patients treated for a maximum of 4 weeks. It is likely that, in the present study, more developed technology, a larger patient cohort, exclusion of patients treated for >3 days and predefined accurate measurements at different aortic segments have provided a more precise assessment of the prevalence of aortitis in newly diagnosed patients.
CTA-defined aortitis is highly prevalent in GCA. It is plausible that histological aortitis is even more prevalent since CTA may not be able to detect mild inflammatory changes. However, according to a previous prospective survey,16 aortic dilation only occurs in approximately one-quarter of patients after 5.4 years of follow-up, indicating that initial aortic inflammation may be necessary but not sufficient to elicit aortic expansion and that additional factors are required for the development of aortic aneurysm. Interestingly, early dilation, as well as dilation occurring during follow-up, was more frequent in men, suggesting that gender-associated factors may play a significant role. Intriguingly, in this and other studies,14 16 24 38,–,40 aortic dilation was more frequent in the ascending aorta while, according to the present study, aortitis is more prominent in the descending aorta. Previous studies have demonstrated increased stiffness and decreased elasticity in inflamed aortas.41 42 A stiff descending aorta may act as a functional coarctation, and the ascending aorta, subjected to high pressure, may consequently undergo progressive dilation. Haemodynamic factors might then play an important role in the development of aortic aneurysms over time (figure 3).
{kind=link}
{kind=link}
{kind=link}
Haemodynamic factors potentially contributing to ascending aortic dilation. Stiffness due to strong inflammatory involvement of the descending thoracic aorta may perform as a functional aortic coarctation.
With regard to aortic branch involvement in GCA, four prospective studies have been published, three using colour DUS and the abovementioned study by Blockmans et al using FDG-PET.24 25 32,–,34 Details of the vascular beds explored and the findings obtained in these studies are summarised in table S1 in the online supplement. Compared with these studies, we found a slightly lower prevalence of CTA-defined vasculitis in peripheral territories, suggesting that CTA may be less sensitive for detecting inflammatory involvement of smaller arteries than ultrasound or FDG-PET. However, given the relatively small patient numbers in all existing studies, differences may have occurred by chance. Interestingly, we found involvement of renal or splanchnic arteries in three (7.5%) and nine (22.5%) patients, respectively. Involvement of these territories was not reported in previous studies. Although these may have not been specifically evaluated, our findings suggest that CTA may be more suitable than ultrasound or FDG-PET for assessing visceral artery inflammation.
When analysing factors associated with LVV, a negative association was observed with the presence of cranial ischaemic complications. A negative association between imaging-detected or symptomatic LVV and visual impairment has previously been observed by some investigators14 29 34 43 but not by others.11 12 16 25 32 This may indicate two extremes in the spectrum of vascular involvement in GCA: predominantly cranial arteritis versus predominantly LVV.
Interestingly, among other associated factors, we found that the extent of LVV was decreased in patients who had received corticosteroid treatment, even for the short period of time allowed for entry into the study, suggesting the efficacy of corticosteroid treatment in limiting LVV. Moreover, in patients receiving treatment with statins or aspirin, widespread LVV tended to be significantly less frequent. A negative correlation between aortic aneurysm and statin treatment has previously been observed.16 These observations raise the hypothesis of whether the anti-inflammatory properties of these drugs may limit the extent of vascular involvement and need to be confirmed in larger series.
In conclusion, this prospective study demonstrates a high prevalence of CTA-defined inflammatory involvement of the aorta and its main branches in GCA. At a time when diagnostic and classification criteria for systemic vasculitis are being revisited,44 our findings and those of previously published studies24 25 32 34 45 support the usefulness of imaging techniques in detecting signs of large vessel inflammation. Prospective follow-up studies are needed to determine the response of LVV to treatment and the relationship between initial LVV inflammation and subsequent aortic dilation or symptomatic large vessel stenosis.40 Moreover, the clinical impact of LVV on disease recurrence or mortality and the cost-effectiveness of routine examinations are important aspects to be determined.
Acknowledgments
The authors thank Anna Jordán, Carmen Ligero, Dr Berta Torres, Dr Miguel A Plasín, Inés Villagrasa and Susana Pastor for their valuable help with the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
↵* SP-G and PA contributed equally to this work.
-
Competing interests None.
-
Ethics approval The study was approved by the Ethics Committee of Hospital Clinic, Barcelona, Spain.
-
Patient consent Obtained.
-
Funding The study was funded by Ministerio de Ciencia e Innovación (SAF 08/04328 and SAF11/30073) and Marató TV3 06/0710. S Prieto-González was a post-residency research award recipient from Hospital Clínic. MC Cid and G Espígol-Frigolé were supported by Instituto de Salud Carlos III.
-
Provenance and peer review Not commissioned; externally peer reviewed.