Article Text

Abstract
Objectives Methotrexate (MTX) is the mainstay treatment for juvenile idiopathic arthritis (JIA), however approximately 30% of children will fail to respond to the drug. Identification of genetic predictors of response to MTX would be invaluable in developing optimal treatment strategies for JIA. Using a candidate gene approach, single nucleotide polymorphisms (SNPs) within genes in the metabolic pathway of MTX, were investigated for association with response to treatment in JIA cases.
Methods Tagging SNPs were selected across 13 MTX metabolic pathway genes and were genotyped using Sequenom genotyping technology in subjects recruited from the Sparks Childhood Arthritis Response to Medication Study. Response to MTX was defined using the American College of Rheumatology (ACR) paediatric response criteria and SNP genotype frequencies were compared between the worst and best responders (ACR-Ped70) to MTX. An independent cohort of US JIA cases was available for validation of initial findings.
Results One SNP within the inosine triphosphate pyrophosphatase gene (ITPA) and two SNPs within 5-aminoimidazole-4-carboxamide ribonucleotide transformylase gene (ATIC) were significantly associated with a poor response to MTX. One of the ATIC SNPs showed a trend towards association with MTX response in an independent cohort of US JIA cases. Meta-analysis of the two studies strengthened this association (combined p value=0.002).
Conclusions This study presents association of a SNP in the ATIC gene with response to MTX in JIA. There is now growing evidence to support a role of the ATIC gene with response to MTX treatment. These results could contribute towards a better understanding of and ability to predict MTX response in JIA.
This paper is freely available online under the BMJ Journals unlocked scheme, see http://ard.bmj.com/info/unlocked.dtl
Statistics from Altmetric.com
Introduction
Juvenile idiopathic arthritis (JIA) is the most common arthritic disease of childhood, affecting 1 in 1000 children and is an important cause of disability.1 Methotrexate (MTX) is the mainstay treatment in JIA and among those children who respond to MTX (65% to 70%) some can enter prolonged remission and have a much improved quality of life.2 3 Unfortunately, for children who fail to respond, the delay in identifying the optimal treatment, such as biological treatment, at an early stage of disease can lead to long-term joint damage. Treatment response is thought to be a complex trait caused by a combination of genetic and environmental factors.4 Identification of clinical or genetic predictors of response to MTX would be valuable in developing optimal, individualised treatment strategies. Candidate gene studies investigating genes encoding enzymes involved in a drug's metabolism or coding for the drug targets have been successful in identifying genetic factors for treatment response.5
The precise mode of action of MTX is unknown,6 but there is some understanding of its metabolic pathway (figure 1) which gives rise to a number of candidate genes. MTX is a folate analogue and enters the cell via the reduced folate carrier (SLC19A1). Once inside the cell it is polyglutamated, catalysed by the enzyme folylpolyglutamate synthetase (FPGS) (this can be reversed via the enzyme γ-glutamyl hydrolase (GGH)). MTX polyglutamates act on several key enzymes including thymidylate synthase (TYMS) that affects pyrimidine synthesis, dihydrofolate reductase (DHFR) that affects folate synthesis and 5-aminoimidazole-4-carboxamide ribonucleotide transformylase (ATIC) that affects purine synthesis. The pathway most potently inhibited by MTX polyglutamates is the conversion of 5-aminoimidazole-4-carboxamide ribonucleotide (AICAR) to formyl-AICAR by the enzyme ATIC. The latter two pathways are thought to lead to accumulation of adenosine, which is a potent anti-inflammatory mediator. Members of the ATP-binding cassette (ABC) family of transporters play a role in the efflux of MTX from the cell. There are many studies that have reported association of single nucleotide polymorphisms (SNPs) within genes in the MTX metabolic pathway and toxicity or response to MTX in diseases such as rheumatoid arthritis (RA) and psoriasis. However, many of these show inconsistent findings and lack of validation in independent datasets. There have been very few studies in JIA.7 8 Therefore the aim of this study was to perform a thorough investigation of SNPs across 13 MTX pathway genes on the efficacy of MTX in patients with JIA.
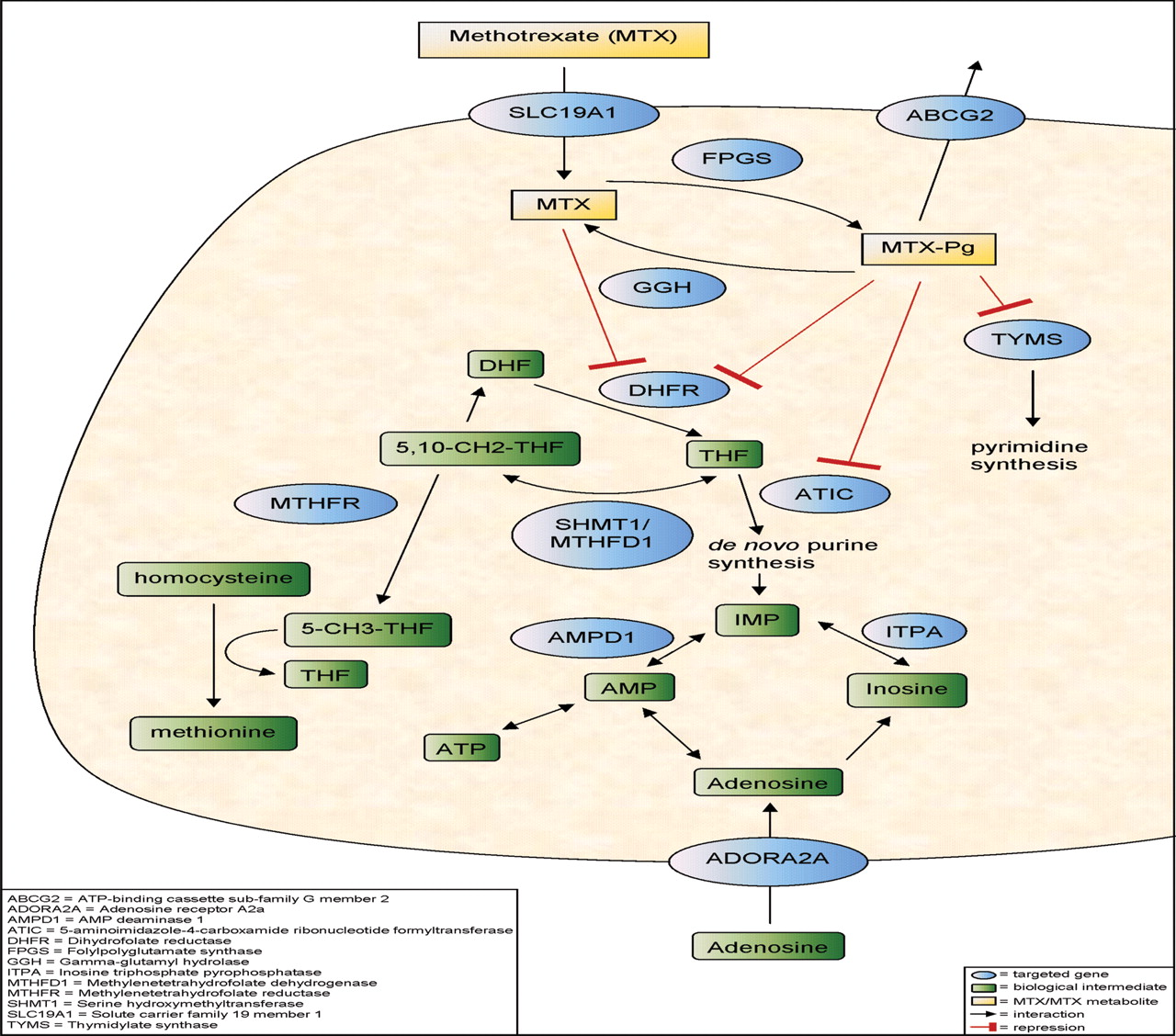
Schematic diagram of the key enzymes and pathways involved in the metabolism of methotrexate (MTX). Genes investigated in this study are highlighted in blue. Modified with permission from PharmGKB. (http://www.pharmgkb.org/do/serve?objId=PA2039&objCls=Pathway).28
Materials and methods
Patients
This work was performed as part of the Sparks CHARMS (for ‘CHildhood Arthritis Response to Medication Study’), which recruits children who fulfil International League of Associations for Rheumatology (ILAR) criteria for JIA9 of all subtypes and who are about to start new disease-modifying medication for active arthritis. The study has full ethical committee approval (Institute of Child Health/Great Ormond Street NHS Trust Ethics Committee) and was fully compliant with the Declaration of Helsinki. Subjects were recruited with fully informed parental consent and child assent where appropriate. Demographic and clinical data were collected at baseline (up to 4 weeks before commencing MTX) and after 6 months of MTX. Weekly MTX was given by either oral or subcutaneous route at 10–15 mg/m2. Data allowing assessment of clinical response to the drug was collected using the validated core set variables and the Definition of Improvement for JIA.10 The variables in the core set are: doctor's global assessment of disease activity (scored on a visual analogue scale of 0–10 with 0=inactive and 10=most severe), parent/patient global assessment of overall well-being (scored on a visual analogue scale of 0–10 with 0=very well and 10=very bad), functional ability (measured by the Childhood Health Assessment Questionnaire),11 number of joints with active arthritis, number of joints with restricted range of movement and the erythrocyte sedimentation rate (mm/h). In the definition of improvement (DOI) for JIA these six items of data are each considered at the start of the therapeutic intervention and after a defined period of time, typically 6 months. The DOI to achieve American College of Rheumatology (ACR)-Ped30 for JIA is when there is at least 30% improvement from baseline in three of any the six variables, with no more than one of the remaining variables worsening by >30%. ACR-Ped50 and ACR-Ped70 for JIA require improvements of 50% or 70% in at least three of the variables, respectively, again with no more than one of the remaining variables worsening by >30%.10 For this study we defined non-responders (NR) as failure to reach even the 30% response improvement (table 1).
Response criteria and numbers for the UK and US cohorts of patients with juvenile idiopathic arthritis (JIA)
Venous blood samples were taken when the child required blood sampling for routine clinical care. This study uses the first 197 children in CHARMS on whom full core set variable clinical data and DNA samples were available.
For validation of the initial findings, DNA from a replication cohort of 210 children with polyarticular or oligoarticular JIA from Cincinnati Children's Hospital Medical Centre, who had also been treated with MTX and analysed pre treatment and at 6 months, were available. SNPs were genotyped using the Affymetrix Genome-Wide Human SNP Array 6.0 (Affymetrix, Santa Clara, California, USA). The study had full ethical committee approval (Cincinnati Children's Hospital Medical Center Institutional Review Board (CCHMC IRB)) and was fully compliant with the Declaration of Helsinki. In this patient cohort improvement of arthritis was defined using active joint count alone. Levels of improvement at 30%, 50% and 70% were defined, and non-responders (NR) were those who did not reach a 30% response improvement (table 1). For the analysis we compared the most extreme phenotypes, so compared allele and genotype frequencies between the best responders (ACR-Ped70 0r 70% improvement in joint count) and the worst responders (NR).
SNP selection
A total of 13 genes known to be in the MTX pathway were selected for SNP genotyping (figure 1). These were ABCG2, ADORA2A, AMPD1, ATIC, DHFR, FPGS, GGH, ITPA, MTHFD1, MTHFR, SHMT1, SLC19A1 (RFC) and TYMS. Pairwise tagging SNPs for each gene were selected using HapMap release 22 (http://www.hapmap.org) and the tagger function in Haploview version 4.112 (http://www.broadinstitute.org/haploview/haploview), using an r2 cut-off ≥0.8 and minor allele frequency (MAF) ≥0.05 within 10 kb upstream and downstream of each gene. In all, 127 SNPs were selected for genotyping.
Genotyping
SNP genotyping was performed using the Sequenom iPlex MassARRAY platform according to the manufacturers instructions (Sequenom, San Diego, California, USA. http://www.sequenom.com/). Only samples and SNPs exceeding a 90% success rate were used in the analysis.
For the US replication cohort SNPs were genotyped using the Affymetrix Genome-Wide Human SNP Array 6.0.
Statistical analysis
Genotype frequencies were compared between non-responders and the best responders to MTX (ACR-Ped70 or 70% improvement in joint count) using the trend test and allelic ORs with 95% CIs were calculated using PLINK13 (http://pngu.mgh.harvard.edu/∼purcell/plink/index.shtml). Meta-analysis was performed using STATA (Stata, College Station, Texas, USA). A test for heterogeneity between cohorts was carried out using the Breslow–Day test and a meta-analysis of the two cohorts was performed using the Cochran–Mantel–Haenszel test.
Results
We present results from the first 197 children in CHARMS on whom full core set variable clinical data and DNA samples were available, with replication of genetic findings in a US cohort (210 children). The numbers for each response definition for the two cohorts are summarised in table 1 and the demographic data summarised in table 2. Note that all children who reach ACR-Ped70 automatically also reach ACR-Ped30 and ACR-Ped50, while those who achieve ACR-Ped50 also achieve ACR-Ped30. Subtype distribution and disease activity was as expected for use of MTX in JIA and in line with previous studies.3 As expected, there was a higher prevalence of women in both cohorts. Disease duration has been recently reported as linked with MTX response14: the median time of disease duration prior to starting MTX in these two cohorts was around 1 year.
Demographics of UK and US cohorts of patients with juvenile idiopathic arthritis (JIA)
Results for all SNPs are shown in supplementary table 1. Of the 127 SNPs genotyped in the CHARMS UK cohort, 10 SNPs failed SNP QC, leaving 117 SNPs for analysis. There was an average coverage of all genes after QC of >89%. Of the 117 SNPs analysed, 3 SNPs were found to be significantly associated with MTX response (p<0.05). Two of the SNPs (rs12995526 and rs4673990) lie within the ATIC gene and are associated with an increased risk of having a poor response to MTX (OR 1.79, 95% CI 1.07 to 3.0 and OR 1.69, 95% CI 1.01 to 2.83, respectively) (table 3). The third associated SNP, rs2295553, lies within the inosine triphosphate pyrophosphatase gene (ITPA) and also conferred an increased risk of having a poor response to MTX (OR 1.73, 95% CI 1.03 to 2.89) (table 3).
SNPs significantly associated with response to MTX (p<0.05) in UK CHARMS dataset
Significantly associated SNPs were assessed in a validation cohort (US cases) where genotype data was available for two of the three most significantly associated SNPs, the ITPA SNP, rs2295553, was not genotyped on the Affymetrix array and there were no proxies (r2>0.8) for this SNP.
Of the two ATIC SNPs, one SNP had been directly genotyped and showed no evidence for association with MTX response (OR 0.76, 95% CI 0.48 to 1.21), the other SNP, rs13005416, is a complete proxy for rs12995526 and showed a trend towards association with MTX response (OR 1.62, 95% CI 1.01 to 2.59) (table 4).
ATIC SNPs investigated for association with response to MTX in the US Cincinnati dataset
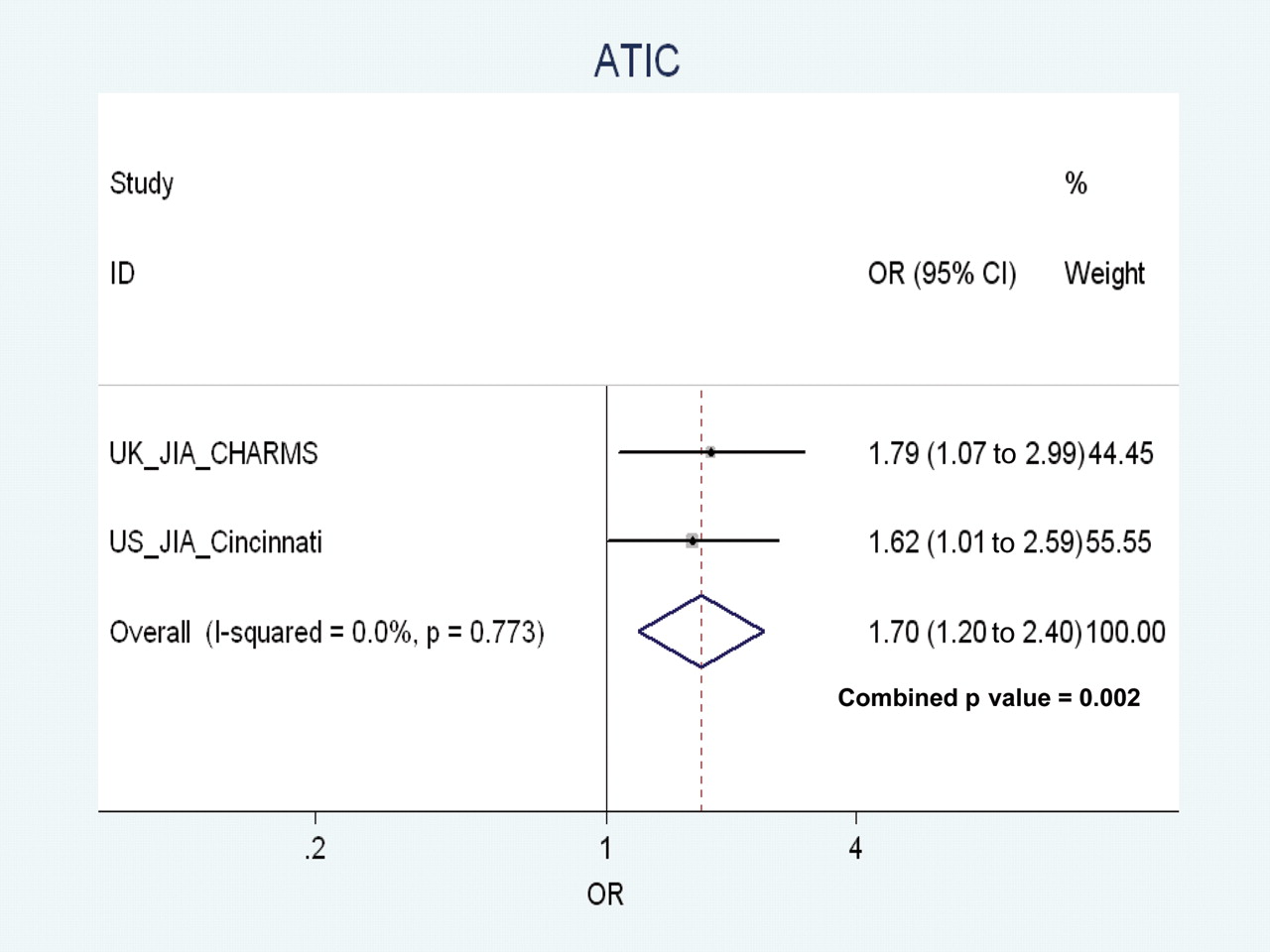
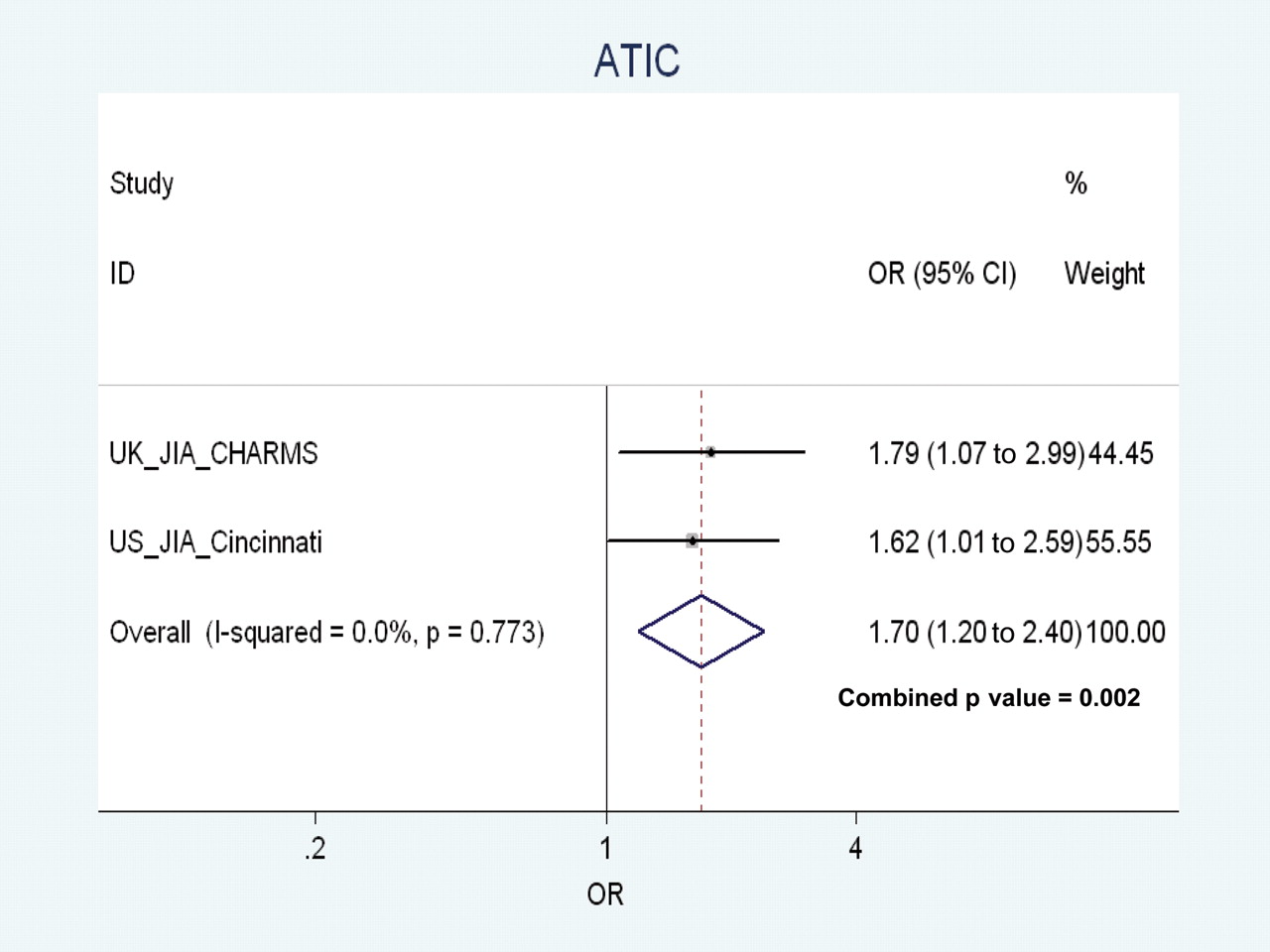
The sample sizes of the discovery cohort and the validation cohort are relatively small and so the results for rs1295526 (and its proxy rs13005416 in the US cohort) were combined in a meta-analysis. This strengthened the evidence of an association of the ATIC SNP with a poor response to MTX, with a combined p value of 0.002, a pooled OR 1.7, 95% CI 1.2 to 2.4. There was no significant evidence for heterogeneity between the studies (p=0.77) (figure 2).
{kind=link}
{kind=link}
Meta-analysis of rs12995526 and its proxy, rs13005416 in the UK CHARMS (for ‘CHildhood Response to Medication Study’) and US Cincinnati datasets. Forest plot displaying ORs and 95% CIs for each of the two studies (UK and US) and the weighting for each study according to sample size. The combined OR from the two studies (1.7) is displayed as a diamond with the peaks denoting the upper and lower limits of the CIs (1.2 to 2.4). The combined p value for association with methotrexate (MTX) response was 0.002. The Breslow–Day test was performed to test for heterogeneity between the two studies, and showed no evidence for heterogeneity (p=0.77).
Discussion
The ultimate aim of therapies for the treatment of JIA is to attain complete control of the disease, to prevent joint damage, maximise a child's physical and psychological well-being and prevent any long-term consequences related to the disease or treatment.1 MTX has transformed the prognosis of children with active JIA,6 however for the third of children who fail to respond to MTX the delay in finding the appropriate treatment may be crucial in terms of their disease outcome, with the risk of joint damage and potential permanent disability. Consequently, identifying predictors of MTX response would be a major advancement in the treatment of JIA.
Candidate gene studies have been previously successful in identifying genes with significant contributions to drug response; genes encoding enzymes involved in the drug metabolism or coding for the drug targets have been shown to be important.5 For example, the association of SNPs within VKORC115 and CYP2C916,–,18 with warfarin dose variability. The latter gene encodes the main metabolising enzyme for the anticoagulant and the former is the warfarin drug target. These findings have since been validated in genome-wide association studies.19 20 Thus it could be hypothesised that investigating SNPs within genes in the MTX metabolic pathway may help to identify genetic factors for MTX response. Only two published studies to date have investigated MTX pathway genes in response to MTX in JIA.7 8 Both these studies investigated individual polymorphisms within MTX pathway genes that have been previously investigated for response to treatment in other diseases that are treated with MTX, such as RA and psoriasis. In this study, rather than just analyse the previously reported SNPs, we took the approach of screening the whole gene using a tagging SNP approach. This was a more thorough approach and enabled us to have >89% coverage of the genes investigated.
Of the two previous studies investigating response to MTX in patients with JIA, the first looked at the two polymorphisms (C677T and A1298C) in the MTHFR gene, which is probably the best studied gene in the MTX metabolic pathway. The SNPs have previously shown evidence of association with MTX response and adverse drug reactions in cancer and adult RA.21 This study found the 677T allele to be associated with greater toxicity and the 1298C allele with better efficacy.7 In our study we have not investigated toxicity but there was a trend towards the 677T allele being associated with a good response to MTX. We had not directly genotyped the A1298C SNP but the SNP, rs4846049, which had an r2=0.93 with the A1298C SNP, showed no evidence for association with response to MTX. The second study in JIA tested SNPs within AMPD1, ATIC, ITPA, MTHFD1 and MTHFR for association with response to MTX in JIA. The MTHFR 1298A-677C haplotype analysis showed carriage of two copies of the 1298A-677C haplotype was associated with good response to MTX.8
Our study found significant evidence for association of three SNPs, two within the ATIC gene and one within ITPA, with response to MTX. Multiple testing is an issue and if we performed a Bonferroni correction for the number of SNPs tested none would remain significant, so instead we have taken the approach of validating any significant findings in an independent cohort. Replication of any genetic association finding is vital in establishing confidence in a discovery but this can be challenging in the field of pharmacogenetics for a number of reasons, firstly the issue of small sample sizes in many of these studies. Collecting large sample sizes for pharmacogenetic studies is much more difficult compared to collecting disease case-control cohorts due to the more detailed clinical and phenotypic data required.5 Secondly it is only recently that a standard measure of how a child responds to a particular treatment in JIA has been developed10 and so studies started before that time may have used slightly different response criteria and so results may be difficult to compare. Finally different SNPs could be studied, again making comparison between studies difficult.
In this study we have attempted to validate our initial findings in an independent cohort of patients with JIA collected in the US. Genome-wide association study data on a cohort of children who also have data on MTX response was available for analysis. Unfortunately the SNP in ITPA had not been genotyped on the SNP array and there were no proxy SNPs (r2>0.8). There was no evidence for association of any SNP within the ITPA gene in this cohort. Therefore this finding still requires validation in an independent dataset. One of the two SNPs in ATIC, which were associated with response to MTX in the UK CHARMS cohort, showed validated association in this independent US cohort. Combined meta-analysis of the CHARMS and US cohorts further strengthened this association with a combined p value of 0.002, pooled OR 1.74 95% CI 1.23 to 2.46). The US cohort used a different definition of response, based on joint count alone because core set criteria were not available.
There is evidence for association of a SNP in ATIC with response to MTX in a study of adult patients with RA; rs2372536 (347C>G) is located within exon 5 of the gene, and it is a threonine to serine substitution at position 116 of the ATIC gene. There have been three studies to date investigating association of this SNP with MTX response in RA. In two studies carriers of the minor GG genotype were associated with good response to MTX,22 23 however in the third study the major CC genotype carriers were associated with good clinical response to MTX.24 It has been proposed that these conflicting results may be due to differences in the population (early onset versus established RA) and in study design (longitudinal data versus cross sectional data). This SNP has also been investigated for association with MTX response in JIA cases, however, no association was found.8 In this study we did not directly genotype this SNP, but genotyped rs4672768 which has an r2=1 with rs2372536. There was no significant evidence for association of this SNP with MTX response. Another SNP, rs4535042, in the 5′ untranslated region (UTR) of the ATIC gene was also associated with a poor response to MTX in a Serbian RA cohort, however, this SNP has not been genotyped in this study and is not on HapMap so LD with our most associated SNP cannot be determined.25 In a recent investigation of the MTX pathway genes in a cohort of patients with RA the intronic ATIC SNP, rs12995526, which we found associated with poor response to MTX in JIA was also associated with poor response to MTX in RA with similar effect sizes (p=0.04 OR 1.51 95% CI 1.0 to 2.28).26
Taking all of this data into consideration, there is growing evidence to support the role of the ATIC gene in the response to MTX treatment. ATIC is the enzyme that is most potently inhibited by MTX polyglutamates, it is involved in the conversion of AICAR to formyl-AICAR. AICAR and its metabolites inhibit two enzymes important in adenosine metabolism causing intracellular accumulation of adenosine (figure 1). Adenosine is a potent anti-inflammatory mediator and it is thought that it is this pathway which is important in the mode of action of MTX.27 It could be hypothesised that defects in ATIC could lead to decreased enzyme activity and affect AICAR accumulation and adenosine release.
In conclusion, we have found preliminary evidence that a genetic variant in ATIC, a key MTX pathway gene, is associated with MTX response in JIA. The C allele of SNP, rs12995526 is associated with poor response to MTX, and this finding is confirmed in an independent cohort of JIA cases. Additional validation is necessary and further investigations will be required to identify the causal variant. Prospective studies will be required to determine the predictive value of these genetic risk factors.
Acknowledgments
We thank the patients and their families for participation in this study, ward and clinic staff for help in collecting samples, Paul Gilbert and other members of the laboratory team for sample handling.
References
Supplementary materials
Web Only Data
Files in this Data Supplement:
Footnotes
LRW and WT contributed equally to this work
-
Funding Sparks CHARMS is funded by Sparks UK and the Big Lottery Fund UK. The study is on the UK Medicines for Children Research Network (MCRN) portfolio. This work was supported by the Arthritis Research Campaign: arc grant reference no: 17552. The US cohort collection and genotyping were supported by NIH (NIAMS N01AR42272, P30AR47363 and P60AR47784).
-
Competing interests The authors have no competing interests to disclose.
-
Ethics approval This study was conducted with the approval of the Institute of Child Health/Great Ormond Street NHS Trust Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.