Article Text

Abstract
Objective To investigate the potential of ultrasound (US) in the differential diagnosis between rheumatoid arthritis (RA) and psoriatic arthritis (PsA) at metacarpophalangeal (MCP) joints level.
Methods 18 RA patients and 20 PsA patients with clinical involvement of MCP joints were included. All US examinations were performed by two rheumatologists investigating: presence of joint cavity widening (JCW), synovial fluid and/or synovial hypertrophy, peritenon extensor tendon inflammation (PTI) and intra-articular or peri-tendinous power Doppler (PD) signal.
Results A total of 83 MCP joints in 18 RA patients were assessed. In all of these the authors found different degrees of JCW. 15 of 83 (18%) MCP joints showed synovial fluid, whereas 68 of 83 (82%) MCP joints showed synovial hypertrophy. In 72 of 83 (86.7%) MCP joints intra-articular PD was detected. No PTI pattern was found in these patients.
In PsA patients, a total of 82 MCP joints in 20 patients were assessed. 54 of 82 (65.8%) MCP joints showed PTI pattern (p = 0.001). In 50 of these 54 (92.5%) MCP joints extra-articular PD signal was detected (p = 0.001). 28 of 82 (34.1%) MCP joints showed different degrees of JCW. 6 of 28 (21.4%) MCP joints presented synovial fluid, whereas 22 of 28 (78.5%) MCP joints showed synovial hypertrophy. In 8 of 82 (9.7%) MCP joints the JCW and PTI patterns were found contemporaneously.
Conclusions Preliminary results demonstrate that PTI pattern is a higher characteristic of PsA, which suggests a potential role of US in the differential diagnosis between RA and PsA at MCP joints level.
Statistics from Altmetric.com
Introduction
Metacarpophalangeal (MCP) joints are frequently involved in patients with rheumatoid arthritis (RA) and psoriatic arthritis (PsA).1 2 Their inflammatory involvement concurs to determine the disease activity and leads to joint damage.1 2
To date, there is a consistent body of evidence supporting the validity of high-resolution ultrasound (US) to provide for sensitive assessment of joints and soft tissue inflammation in patients with chronic arthritis.3,–,6 Despite US being shown to be a valuable tool in daily rheumatological practice, the sonographic findings have yet to be included in the diagnostic criteria of chronic inflammatory arthropathies.7
RA and PsA are chronic inflammatory diseases characterised by several similarities and several differences. Although US has been demonstrated to be useful in the assessment of inflammatory process at joint level in both conditions,3,–,6 there is a lack of evidence supporting its role in the differential diagnosis.
As the recent availability of US systems with very high-frequency probes allows for the detection of detailed morphostructural abnormalities and minimal blood flow changes at superficial soft tissues level,8 it was decided to investigate the potential of US in the differential diagnosis between RA and PsA at MCP joints level.
Methods
Patients
Eighteen patients with diagnosis of RA (four men and 14 women) and 20 patients with diagnosis of peripheral PsA (12 men and eight women) with clinical involvement of at least one MCP joint were included in the present study. Diagnoses were made according to the American College of Rheumatology (formerly the American Rheumatism Association) and European Spondyloarthropathy Study Group classification criteria respectively.
Clinical examination aimed to detect tenderness and/or swelling at MCP joints level was performed by an expert rheumatologist (FS). Patients younger than 18 years of age, and those with other concomitant inflammatory diseases (particularly osteoarthritis or gout), history of hand fracture or surgery or presence of severe hand deformities were excluded from the study. Additionally, no PsA patients with skin and nail manifestations at hand level, or distal interphalangeal joint involvement were included. All patients were attending the outpatient and inpatient clinics of the Rheumatology Department of the Università Politecnica delle Marche (Ancona-Italy). The mean ± SD for the age and disease duration were: 51 years ± 8.7 and 36 months ± 18.5 for RA patients and 43 years ± 8.6 and 23 months ± 15.7 for PsA patients respectively.
Study design
All US examinations were performed and interpreted by consensus by two experienced rheumatologist sonographers (EF and MG), blinded to the clinical data. Patients were asked not to talk about their clinical condition with the US examiners. Prior to the study, the investigators reached a consensus on the US scanning technique to adopt and on interpretation of US findings.
The following pathological US findings: presence of joint cavity widening (JCW), due to synovial fluid and/or synovial hypertrophy, hypoechoic swelling surrounding the extensor digitorum tendon and intra-articular or peri-tendinous power Doppler (PD) signal, were investigated at the dorsal aspect of clinically inflamed MCP joints in all patients. These targets were chosen because they are frequently involved sites in RA and PsA, and US allows for a sensitive detection of intra-articular and peri-articular superficial soft tissue inflammation. In order to have normal MCP joints as a comparator, the sonographers had access to a core set of US images displaying representative examples of the non-inflamed dorsal aspect of the MCP joints.
As the study was focused on soft tissues, bone abnormalities (ie, erosions and/or osteophytes) were not assessed.
The study was conducted according to the Declaration of Helsinki and local regulations. The institutional ethics committee approved the study and informed consent was obtained from all patients.
US assessment
The US examinations were performed using a MyLab 70 XVG (Esaote S.p.A., Genoa, Italy) equipped with 6–18 MHz broad band multifrequency linear transducer (within the focal area the transducer has an axial resolution of 30 μm and a lateral resolution of 60 μm) and Doppler frequency between 7.1 and 14.3 MHz.
Clinically involved MCP joints were scanned using a multiplanar technique, adopting the indications provided by the EULAR guidelines for musculoskeletal ultrasound in rheumatology.9
The dorsal aspect of the MCP joints was examined by US with the patient seated with hands lying in prone position on the examination table. Both longitudinal and transverse scans were performed by slightly moving the transducer from radial to ulnar and from proximal to distal sides on dorsal aspect to enable maximum coverage of the anatomical surface area. Moreover, plenty of gel was used, in order to avoid compression of the tissues under examination. Figure S1 shows the main scanning planes and the corresponding US images (see online supplementary figure S1).
US greyscale imaging parameters were set in order to obtain maximal contrast between all the structures under examination. PD settings were standardised at the following values: pulse repetition frequency: 750 Hz, persistence: 4, wall filter: 3 and Doppler frequency between 9.1 and 11.1 MHz. Colour gain was set just below the level at which colour noise appeared underlying bone (no flow should be visualised at the bony surface). To confirm that the PD signal represented real blood flow and not an artefact, the spectral Doppler was used.
For the identification of synovial fluid and synovial hypertrophy, the OMERACT preliminary definitions were adopted.10 Particular attention has been paid at the assessment of inflammatory process located at extensor digitorum tendon and soft tissues level. Peritenon extensor tendon inflammation (PTI) pattern was interpreted as: an US abnormality characterised by hypoechoic swelling of the soft tissue surrounding the extensor digitorum tendon, with or without peri-tendinous PD signal.
Statistical analysis
Standard descriptive statistics, including proportions for US findings, were expressed as mean and SD for demographic data. Comparison between US findings and clinical diagnosis was performed by χ2 analysis. A p value under 0.05 was considered statistically significant. All statistical analysis were preformed using MedCalc, version 10.0 for Windows XP.
Results
Table S1 (see online supplementary table S1) shows the demographic and clinical data of the patients.
Rheumatoid arthritis
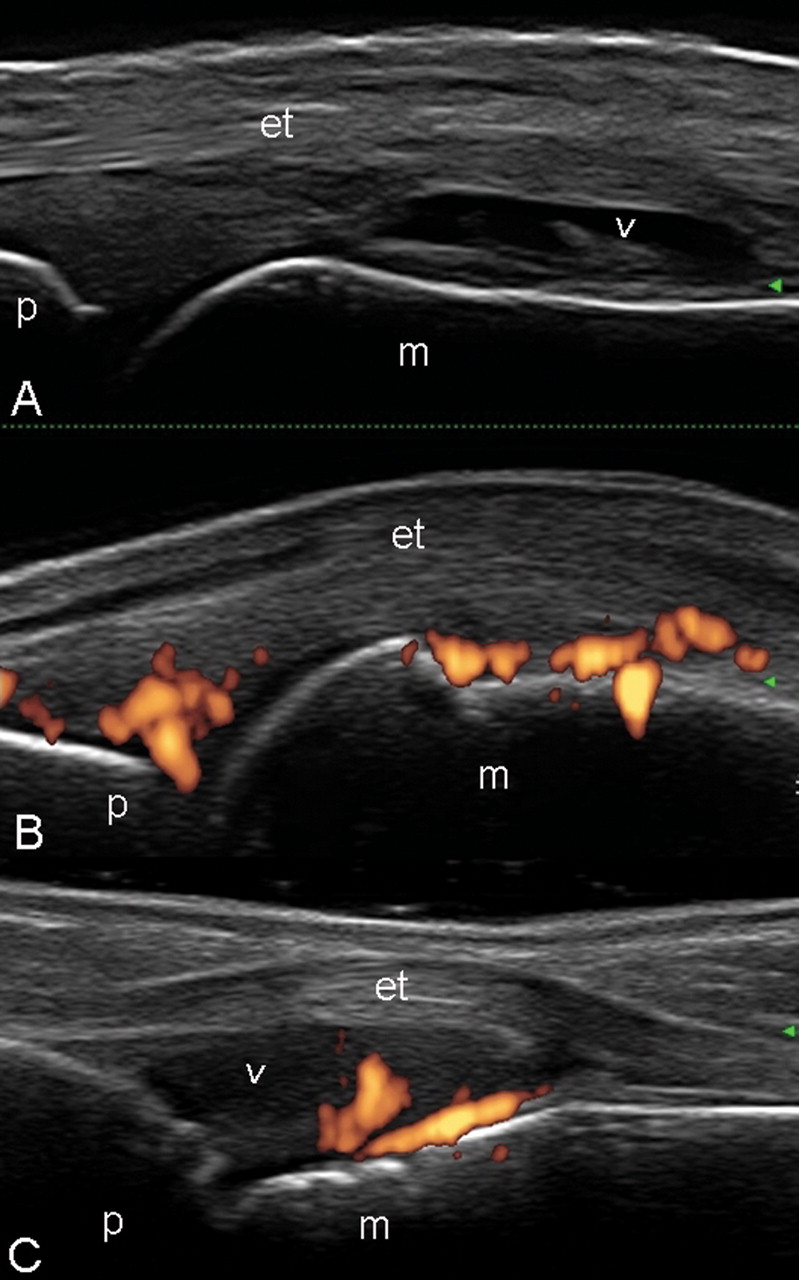
Ninety-one clinically involved MCP joints of a total of 144 MCP joints in 18 RA patients were assessed by US. Eight MCP joints were excluded as no US signs of inflammation were found (table 1). In the remaining 83 MCP joints (100%), different degrees of JCW were found (figure 1A–C). In 15 out of 83 (18%) MCP joints synovial fluid was found, whereas 68 out of 83 (82%) MCP joints presented synovial hypertrophy (figure 1A). In 72 out of 83 (86.7%) MCP joints intra-articular PD was detected (figure 1B–C) (p = 0.01). No PTI sonographic pattern was found in these patients.

Rheumatoid arthritis. Metacarpophalangeal joints. Dorsal longitudinal scan. A. Joint cavity widening with proliferative tissue within the synovial membrane (arrowhead) and without power Doppler signal. B. Intra-articular power Doppler signal prevalent at fat pad level. C. Synovitis with presence of synovial hypertrophy (arrowhead) and intra-articular power Doppler signal near to the bone profile. et, extensor digitorum tendon; m, metacarpal bone; p, proximal phalanx.
Comparison between US findings and clinical diagnosis
Psoriatic arthritis
Eighty-eight clinically involved MCP joints of a total of 160 MCP joints in 20 PsA patients were assessed by US. Six MCP joints were excluded as US did not find signs of inflammation (table 1). In 54 out of 82 (65.8%) MCP joints a PTI pattern was found as the only US sign of inflammation (figure 2A–D) (p = 0.001). In 50 out of these 54 (92.5%) MCP joints, an extra-articular PD signal was detected (p = 0.001).

{kind=link}
{kind=link}
Psoriatic arthritis. A–B. Metacarpophalangeal joint on dorsal longitudinal scan and transverse scan (C–D) showing the peritenon extensor tendon inflammation (PTI) pattern. The greyscale US assessment (A) shows a hypoechoic swelling surrounding the extensor digitorum tendon (*) associated with subcutaneous oedema. Note that the power Doppler signal is distributed surrounding the extensor digitorum tendon (B–D). E–F, Metacarpophalangeal joint on dorsal longitudinal scan showing both joint cavity widening (circle) and hypoechoic swelling surrounding the extensor digitorum tendon. Note moreover the intra-articular and peri-tendinous distribution of power Doppler signal. et, extensor digitorum tendon; m, metacarpal bone; p, proximal phalanx.
Twenty-eight out of 82 (34.1%) MCP joints showed different degrees of JCW (p = 0.56). Six out of 28 (21.4%) MCP joints presented synovial fluid (p = 0.068), whereas 22 out of 28 (78.6%) MCP joints showed synovial hypertrophy (p = 0.71). In all of these MCP joints an intra-articular PD was detected. In eight out of 82 (9.7%) MCP joints, the JCW and PTI patterns were found together with intra-articular and peri-tendinous PD respectively (figure 2E–F).
The PTI pattern was detected in seven out of 10 (70%) patients with less than 18 months of disease duration (mean: 13.2 months; DS: 3.67).
Discussion
Differential diagnosis between RA and PsA can be made comfortably using clinical and topographic data. Additionally, there are several studies postulating remarkable differences between both conditions from different viewpoints. For instance, histopathological analysis of synovial tissues showed that PsA tissues had significantly less lining layer thickness and greater vascularity than RA.11 Some MRI studies have demonstrated a clear link between enthesitis and synovitis in individual swollen joints in PsA, but not in RA.5 12 Following this line, McGonagle et al developed the concept of the ‘enthesis organ’,13 which comprises the enthesis and also adjacent fibrocartilages and synovial membranes. Although enthesitis is typically viewed as a focal insertional disorder, MRI and US findings have demonstrated the presence of more diffuse inflammatory changes involving areas distant from the insertion sites.14 15 Taking into account these pieces of information and the possibility of performing an accurate assessment of intra-articular and extra-articular morphostructural and blood flow changes using PD US, the hypothesis was tested that US detection of extra-articular tissue involvement could be characteristic of PsA rather than RA. To this end, the dorsal aspect of MCP joints was chosen, due to the intimate relationship between enthesis organ, extensor digitorum tendon and synovial membrane.
To date, some studies studying RA and PsA patients have been performed,16,–,20 but these exclusively focused on demonstrating different US findings in these conditions. Frediani et al demonstrated a higher prevalence of quadriceps enthesitis in PsA than RA patients.16 Similar findings have been suggested by Falsetti et al, studying the heel fat pad and the Achilles tendon.18 19 Most recently, Jevtiv et al studied the fingers of 11 RA and 13 PsA patients using MRI, showing extrasynovial inflammatory changes affecting the peri-articular soft tissue structures in at least half the patients with PsA.21 Fournié et al, demonstrated similar findings in 84% using PD in symptomatic PsA fingers.5 To the best of the authors' knowledge, this is the first study that exploits a possible role of the US in differential diagnosis between RA and PsA.
In the present study, no relevant statistical differences between RA and PsA could be found in terms of presence/absence of JCW, synovial fluid and/or synovial hypertrophy, whereas PTI pattern was not found in patients with RA, suggesting a potential diagnostic value of this US pattern for the identification of patients with PsA.
The data obtained in the present study must be interpreted in light of the following aspects. First, the detection of such involvement may depend on the US equipment and requires very high frequency probes and Doppler frequency. Second, only the dorsal aspect of clinically MCP joints involved was investigated. Finally, the study was conducted in a small number of patients.
In spite of this, the preliminary study suggests that a careful assessment of the peritenon extensor tendon and the respective surrounding soft tissues should be part of the standard US approach to study MCP joints, especially in patients with undifferentiated arthritis. In these patients a clearly evident PTI sonographic pattern should suggest a PsA.
Additionally, it was noted that the PTI pattern was frequently observed in patients with short time of disease duration (mean: 13.2 months; SD: 3.67). According to this observation, it is believed that the inflammatory process in PsA could begin at the soft tissue level surrounding the extensor digitorum tendon, successively involving the synovial membrane, by the intimate continuity of these structures frequently undergoing stress mechanisms, 22 whereas an isolate synovitis could be detected in the late stages of PsA disease.
Although there is no US study that can support this hypothesis, previous reports stressed the fact that the extra-articular tissue involvement seems to be characteristic of spondyloarthritis rather than RA.23 24 Particular attention also should be paid to the flexor digitorum tendons, which are frequently involved in PsA and demonstrated characteristic US findings with respect to those seen in RA.5
In conclusion, preliminary results demonstrate that PTI pattern is a higher characteristic of PsA, which suggests a relevant potential role for US in the differential diagnosis between RA and PsA at MCP joints level. Additional research studying larger cohorts and aimed at investigate validity issues including accuracy and reproducibility are required to confirm these preliminary results.
References
Supplementary materials
Web Only Data
Files in this Data Supplement:
{kind=link}
Footnotes
-
Competing interest None.
-
Patient consent Obtained.
-
Ethics approval This study was conducted with the approval of the Comitato Etico dell'Azienda Sanitaria Unica Regionale di Ancona.
-
Provenance and peer review Not commissioned; externally peer reviewed.