Article Text

Abstract
Objectives Mixed connective tissue disease (MCTD) is an immune-mediated, systemic disorder of unknown aetiology. As the epidemiology of the disease is largely unknown, the authors performed a nationwide cross-sectional retrospective study to assess the prevalence and incidence of MCTD in Norway.
Methods Every adult patient (≥18 years) with MCTD seen at one of the departments of rheumatology was reviewed for inclusion. Only patients who satisfied the following four criteria were included: clinical diagnosis of MCTD verified by a rheumatologist; positive serum anti-ribonucleoprotein antibody test; fulfilment of at least one of three of following criteria sets: the modified Sharp's criteria, the criteria of Alarcón-Segovia and Villareal and those of Kasukawa; and exclusion of other connective tissue diseases.
Results The four inclusion criteria were fulfilled by 147 adult Caucasian patients. The female to male ratio was 3.3 and the mean age at diagnosis of adult-onset MCTD was 37.9 years (95% CI 35.3 to 40.4 years). At the end of 2008, the point prevalence of living adult MCTD patients in Norway was 3.8 (95% CI 3.2 to 4.4) per 100 000 adults. The incidence of adult-onset MCTD in Norway during the period from 1996 to 2005 was 2.1 (95% CI 1.7 to 2.5) per million per year.
Conclusions MCTD has a female predominance and the incidence and prevalence of MCTD is low, and lower than reported figures for polymyositis, dermatomyositis, systemic sclerosis and systemic lupus erythematosus. The prevalence estimates were similar across the three criteria sets of MCTD.
Statistics from Altmetric.com
The concept of mixed connective tissue disease (MCTD) as a separate immune-mediated connective tissue disorder was first introduced by Sharp and co-workers in 1972.1 They described a disorder that was characterised by serum autoantibodies directed against ribonucleoprotein (anti-ribonucleoprotein),2 3 and had distinct clinical features including: Raynaud's phenomenon, puffy hands, arthritis, pleuritis, pericarditis, myositis and interstitial lung disease.4 Some of these features are also seen in systemic lupus erythematosus (SLE), polymyositis and systemic sclerosis, but the complete picture appears to be unique to MCTD. For three decades, the concept of MCTD has been discussed and it is still not clear if it is a distinct disease identity or whether it represents an overlap between other connective diseases. Nevertheless, the concept of MCTD seems to persist.5,–,7
MCTD seems to affect women more frequently than men8 and the disease may start in childhood or in adults. No accurate prevalence or incidence data on adult MCTD have been published,9 but a population-based epidemiological enquiry from Finland indicated a prevalence as low as 0.8 patients per 100 000 adults.10 One report, also from Finland, has suggested that the incidence of MCTD in children is 0.1 patients per million per year.11
The paucity of epidemiological studies may be partly due to the lack of internationally accepted classification or diagnostic criteria for MCTD. The three sets of diagnostic and classification criteria that are most often used are the modified Sharp's criteria,12 the criteria of Alarcón-Segovia and Villareal13 and those of Kasukawa et al.14 Another, less used criteria set is that by Kahn15 (see supplementary file ‘Criteria sets for mixed connective tissue disease’;, available online only).
In 1996, Amigues and co-workers16 performed a comparison of the sensitivity and specificity of the four criteria sets for MCTD. They concluded that the Sharp's criteria12 was most sensitive, but that the criteria of Alarcón-Segovia and Villareal13 and of Kahn15 had better specificity. As there is no consensus on which MCTD criteria to apply, we decided to include the three most commonly used in our nationwide, cross-sectional study on MCTD.
Methods
Patients
All the 16 Norwegian public hospitals that have a department of rheumatology agreed to participate in the study. The inclusion of patients started on 15 March 2005 and ended on 31 December 2008.
The inclusion of adult MCTD patients (aged ≥18 years) was based on the four following criteria: a clinical diagnosis of MCTD verified by a rheumatologist; a positive serum anti-ribonucleoprotein antibody test; fulfilment of at least one of three most commonly used criteria sets for MCTD: the modified Sharp's criteria set,12 the criteria set of Alarcón-Segovia and Villareal13 or those of Kasukawa and co-workers;14 and the exclusion of other connective tissue diseases.
In the initial case-finding step, each of the 16 departments of rheumatology reviewed their hospital records to identify patients diagnosed with MCTD according to the International Classification of Diseases (ICD) coding system. All patients in Norway, either admitted to the hospital or seen on an outpatient basis, are registered in the hospitals' data systems, with an ICD-10 diagnosis code. The 10th revised version (ICD10) has been in use in all Norwegian hospitals from 1999 and earlier versions before that. The principal investigator (RG) was notified every time a patient with suspected MCTD and high titre serum anti-ribonucleoprotein antibodies was identified at one of the local rheumatology departments. He then checked if the patient fulfilled one or more of the three MCTD criteria sets. Finally, the records of every patient who fulfilled the first three inclusion criteria were re-examined to exclude other connective tissue diseases.
Patients who satisfied all the four inclusion criteria were given oral and written information about the study and asked to participate. The patients who provided an informed consent were then enrolled in the study.
The clinical assessment of each patient was performed according to a predefined clinical form by one of the investigators. The assessment included standardised questions about symptoms, clinical examination and predefined blood tests.
Laboratory tests
The primary serum antinuclear antibodies and anti-ribonucleoprotein analyses of the patients were performed locally. To avoid potential false-positive anti-ribonucleoprotein tests, we only included patients who had high titre positive anti-ribonucleoprotein antibodies (as defined by their local laboratory). Serum samples collected after inclusion were sent to our reference laboratory at the Institute of Immunology, Oslo University Hospital Rikshospitalet. At the Institute of Immunology, the sera were screened for anti-ribonucleoprotein antibodies by an automated ELISA (EliA RNP; Phadia, Freiburg, Germany).
Data analysis
Completed data forms were sent to the primary investigator at the Department of Rheumatology, Oslo University Hospital Rikshospitalet, for central registration and analysis. Cardiff Teleform 10.1 scanning software was used to import data to the Microsoft Office Access database software and statistical analyses were performed by SPSS, versions 16/17.
Updated geographical population data for Norway was gathered from the Norwegian Statistical Institute (Statistisk sentralbyrå, http://www.ssb.no). In case of incidence, the year at diagnosis was recorded retrospectively. The incidence rate was calculated as the number of patients per million inhabitants per year. As only 18-year-old and older patients were included, we only calculated the incidence of adult-onset MCTD disease.
Results
A total of 147 MCTD patients, 113 (76.9%) women and 34 men (23.1%), aged 18 years and older at the time of the study, met the five inclusion criteria. All these 147 patients agreed to participate. All the patients were Caucasians and 145 of 147 were native Scandinavians. The female to male ratio was 3.3.
The clinical manifestations most frequently reported were Raynaud's phenomenon (present in 99% of patients) and puffy hands (in 93%). Other common manifestations included arthritis (79%), symptoms of oesophageal dysmotility (50%) and self-reported dyspnoea (47%) (figure 1).

An overview of the most common clinical features and serum autoantibodies in the course of the disease in the mixed connective tissue disease population. anti-RNP, anti-ribonucleoprotein.
The time span from the clinical diagnosis of MCTD to study inclusion (defined as the follow-up time before inclusion) ranged from under 1 year to 38 years. The mean follow-up time was 12.8 years (95% CI 11.4 to 14.2 years).
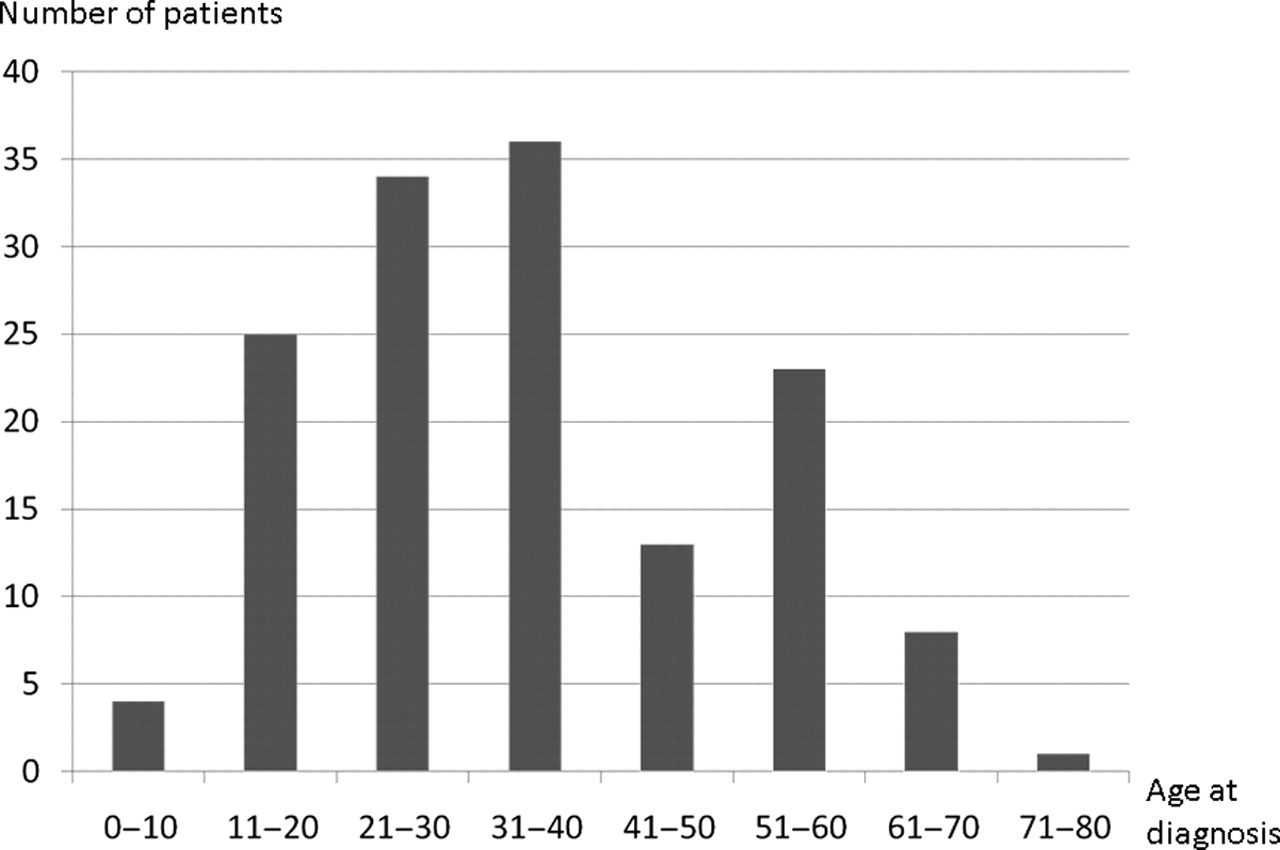
The year of diagnosis was available in 145 patients (98.6%). Fifteen patients (10.2%) were diagnosed before 18 years of age and were thus defined as juvenile MCTD. The mean age of diagnosis in the 15 juvenile patients was 13.0 years (95% CI 11.6 to 14.4 years). Four of the youngest patients included in the study were 9 years old when they were diagnosed with MCTD. The remaining 132 patients with adult-onset MCTD had a mean age at diagnosis of 37.9 years (95% CI 35.3 to 40.4 years).
It was possible to determine the time point of the first disease manifestation in 143 (97.3%) of the patients. The mean age of the patients at the first disease manifestation was 31.5 years (95% CI 28.9 to 34.1 years), whereas the mean age at diagnosis was 35.1 years (figure 2). Debut of symptoms before the age of 18 years was noted in 26 patients, but only 15 of those were later diagnosed as juvenile MCTD.

The age distribution of the mixed connective tissue disease patients at time of diagnosis.
The clinical featured were similar and the sex ratio was not statistically different between the adult and juvenile MCTD patients, with the female to male ratio at 3.7 in the juvenile and 3.5 in the adult patients.
The year by year incidence of MCTD diagnosed in Norway since 1972 (when the disease concept was first introduced by Sharp et al)1 is presented in figure 3. The mean annual incidence of adult-onset MCTD between 1996 and 2005 was 2.1 (95% CI 1.7 to 2.5) per million.

Number of mixed connective tissue disease patients diagnosed by year.
The point prevalence of all living MCTD patients 18 years or older in Norway at the end of the inclusion period (31 December 2008) was 3.8 (95% CI 3.2 to 4.4)/100 000 and the point prevalence of adult-onset MCTD was 3.4 (95% CI 2.8 to 4.0)/100 000.
The vast majority of the patients (97.3%) fulfilled at least two of the three MCTD criteria sets (figure 4). In total, 142 of the patients (96.6%) fulfilled the modified Sharp's criteria for MCTD,12 132 (89.8%) fulfilled the criteria of Alarcón-Segovia and Villareal,13 while 127 (86.4%) fulfilled the criteria set of Kasukawa et al14 (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
The mixed connective tissue disease population fulfilling various combinations of criteria sets. ASC, Alarcón-Segovia criteria; KC, Kasukawa criteria; SC, modified Sharp's criteria.
The point prevalence showed no statistical difference between the three criteria sets. Using the modified Sharp's criteria12 the point prevalence was 3.7 (95% CI 3.1 to 4.3)/100 000, whereas using the criteria sets of Alarcón-Segovia and Villareal13 it was 3.5 (95% CI 2.9 to 4.1) and that of Kasukawa et al14 it was 3.3 (95% CI 2.7 to 3.9)/100 000.
We observed a distinct geographical variation in the prevalence of MCTD in Norway. The point prevalence of adult MCTD in the Northern Norway Regional Health Authority (with a population of 0.46 million) was estimated at 1.7 (95% CI 0.3 to 3.0)/100 000, whereas the prevalence in the Southern and Eastern Norway Regional Health Authority (with a population of 2.67 million) was estimated at 4.5 (95% CI 3.6 to 5.4)/100 000. The prevalence of MCTD in the Western Norway Regional Health Authority (population 1.0 million) and in the Central Norway Regional Health Authority (population 0.67 million) were 2.9 (95% CI 1.7 to 4.1)/100 000 and 3.7 (95% CI 2.0 to 5.4)/100 000, respectively. In the North Norway Regional Health Authority, 100% of the patients fulfilled all three criteria, whereas in the Southern and Eastern Norway Regional Health Authority, 75% fulfilled all three criteria, 22% fulfilled two criteria and 3% fulfilled one criterion (table 1).
The MCTD population and the three criteria sets after geographical distribution in Norway
Discussion
Norway is a country with a relatively homogenous population, easy access to a free public health service, computer-based hospital registries and a national registry of citizens. It is thus a country that is suitable for performing epidemiological studies. Our results suggest that the frequency of MCTD is higher than previously reported,10 but that the incidence and prevalence of the disease appears to be lower than previously reported figures for polymyositis/dermatomyositis,17 18 systemic sclerosis,19 20 SLE21,–,23 and primary Sjögren's syndrome.24,–,27
Until this study, no accurate prevalence or incidence estimates of MCTD have been available in adult patients.9 A population-based epidemiological enquiry from Finland in 199010 looked at cases identified by nationwide sickness insurance schemes to receive specially reimbursed medication, and found a point prevalence of MCTD as low as 0.8/100 000. The calculations were based on a clinical diagnosis of MCTD and no disease criteria were used. The discrepancy may be explained by the different study designs and that our study was performed nearly 20 years later.
The present study supports the notion of a female predominance in MCTD, with a female to male ratio of 3.3. This number is comparable to the 3.6 ratio found by Lundberg and Hedfors28 in a study in which they evaluated 32 Swedish patients fulfilling the Alarcón-Segovia criteria set. It is, however, very different from the 10.8 ratio that was reported by Burdt et al8 in a cohort of 47 MCTD patients from Missouri, USA, using the Kasukawa et al criteria set.14 We do not know why there is such a discrepancy in the sex ratio between the studies, but believe that the difference in study design might be important. Our study was structured as an epidemiological study, whereas the study by Burdt et al8 was a long-term follow-up study. It is possible that male patients are more likely to be lost to follow-up. Some of the difference might also be ethnicity difference, as nine out of 47 patients (19%) in the cohort of Burdt et al8 were of African-American ancestry.
No comparison of the MCTD criteria set forth by Sharp,12 Alarcón-Segovia and Villareal13 and Kasukawa et al14 has ever been performed in an epidemiological setting. We thus found it interesting to apply all the three criteria sets in our nationwide study. Our data showed that three of every four MCTD patient (75.5%) fulfilled all the three criteria sets and there was no statistical significance in prevalence rates between the three criteria sets. The latter indicates that previously published epidemiological data using either one of the three criteria sets may be comparable. It must be stated that the current study is, of course, not suited to evaluate the sensitivity and specificity of these criteria.
Unexpectedly, we observed geographical variations in the frequency of MCTD in Norway. In fact, the prevalence in the Southern and Eastern Norway Regional Health Authority by 4.5 (95% CI 3.6 to 5.4)/00 000 was 2.7 times higher than in the Northern Norway Regional Health Authority (1.7; 95% CI 0.3 to 3.0). We believe that this difference may, at least partly, be explained by variation in the accessibility of specialist health care. Many of the patients in northern Norway will have a travelling distance to their department of rheumatology (which are located in the cities of Tromsø and Bodø) that is much longer than the distance to the nearest centre for patients living in other parts of Norway. It is also possible that more cases of MCTD, due to longer distances to primary health care and less stable staff of general practitioners, go unnoticed in northern Norway. Finally, there may be regional differences in the process of classifying individual patients as MCTD, SLE or overlap connective tissue disease. Having said this, we can, of course, not exclude the possibility that there is a real geographical variation in the occurrence of MCTD in Norway.
The aim of the study was quite ambitious, to identify all MCTD patients in Norway and get a real estimate of the prevalence and incidence of the disease. Because the public healthcare system in Norway takes care of almost all patients diagnosed with connective tissue disease at public hospital clinics, we were able to use the local hospital registries for case finding and then screen every patient who had a clinical MCTD diagnosis and was seen at one of the departments of rheumatology during the inclusion period. This hospital-based strategy obviously has some potential weaknesses: First, it misses MCTD patients diagnosed and treated by other medical specialties. We do believe that this is a minor problem in Norway, because the vast majority of patients with suspected connective tissue diseases are referred to one of the public departments of rheumatology. Second, the selected strategy misses the patients who were primarily diagnosed with MCTD, but had a disease that developed into SLE, inflammatory myositis or systemic sclerosis before our inclusion period started. Finally, it misses MCTD patients who were lost to follow-up or died before the start of the inclusion period. As a result of these limitations, it is not unlikely that a population-based survey would have revealed a higher disease frequency than the one we have estimated here. Our prevalence and incidence calculations should thus be regarded as a minimum estimates.
Further research in the concept of MCTD is clearly necessary and we hope to be able to follow these patients to answer some of the key questions in the next few years.
Acknowledgments
The authors thank Torhild Garen, Department of Rheumatology, Oslo University Hospital-Rikshospitalet for assistance in gathering data.
References
Supplementary materials
Web Only Data
Files in this Data Supplement:
Footnotes
↵* The members of the PAHNORI Study Group are listed at the end of the paper.
-
Funding This study was supported by grants from the Norwegian Rheumatism Association and the Scandinavian Rheumatology Research Foundation.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval This study was conducted with the approval of the Regional Committee for Research Ethics in the Southern and Eastern Norway Regional Health Authority and the Norwegian Social Science Data Services.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
PAHNOR1 Study Group Åse Stavland Lexberg, Department of Rheumatology, Buskerud Hospital, Drammen, Norway; Kari Time, Haugesund Sanitetsforeningens Revmatismesykehus, Haugesund, Norway; Alvilde Sofie Strand Dhainaut, Department of Rheumatology, St Olavs Hospital, Trondheim University Hospital, Trondheim, Norway; Liv-Turid Bertelsen, Department of Rheumatology, Haukeland University Hospital, Bergen, Norway; Øyvind Palm, Lamya Samir Noori Garabet, Department of Rheumatology, Østfold Hospital, Moss, Norway; Karen Irgens, Department of Rheumatology, Ålesund Hospital, Ålesund, Norway; Andrea Becker-Merok, Department of Rheumatology, Institute of Clinical Medicine, University of Tromsø, Tromsø, Norway; Jan Leidulf Nordeide, Department of Rheumatology, Førde Central Hospital, Førde, Norway; Villy Johnsen, Department of Rheumatology, Sørlandet Hospital, Kristiansand, Norway; Sonja Pedersen, Department of Rheumatology, Nordland Hospital, Bodø, Norway; Anne Prøven, Department of Rheumatology, Martina Hansens Hospital, Baerum, Norway; Sven Gøran Sidenvall, Department of Rheumatology, Innlandet Hospital, Kongsvinger, Norway.