Article Text

Abstract
Objective To determine the magnitude of all-cause mortality risk in patients with antineutrophil cytoplasmic antibodies-associated vasculitis (AAV) compared with the general population through a meta-analysis of observational studies.
Methods We searched Medline and Embase databases from their inception to April 2015. Observational studies that met the following criteria were assessed by two researchers: (1) clearly defined AAV identified by either the American College of Rheumatology 1990 classification criteria or the 2012 Chapel Hill Consensus Conference disease definitions, and (2) reported standardised mortality ratios (SMR) and 95% CI. We calculated weighted-pooled summary estimates of SMRs (meta-SMRs) for all-cause mortality using random-effects model, tested for publication bias and heterogeneity.
Results Ten studies met the inclusion criteria, comprising 3338 patients with AAV enrolled from 1966 to 2009, and a total of 1091 observed deaths. Overall, we found a 2.7-fold increased risk of death in patients with AAV when compared with the general population (meta-SMR: 2.71 (95% CI 2.26 to 3.24)). Analysis on studies that included only granulomatosis with polyangiitis cases also indicated a similar mortality risk (meta-SMR: 2.63 (95% CI 2.02 to 3.43)). There was no significant publication bias or small-study effect. Subgroup analyses showed that mortality risks were higher in older cohorts, with a trend towards improvement over time (ie, those with their midpoint of enrolment periods that were between 1980–1993 and 1994–1999, vs 2000–2005).
Conclusion Published data indicate there is a 2.7-fold increase in mortality among patients with AAV compared with the general population.
- ANCA
- vasculitis
- mortality
- meta-analysis
- observational studies
Statistics from Altmetric.com
Introduction
Primary systemic vasculitides are a heterogeneous group of rare diseases characterised by the presence of necrotising inflammation of the blood vessel wall. Among the various hypotheses on the immunological mechanisms seeking to explain the nature of these diseases, the antineutrophil cytoplasmic antibodies (ANCA) appear to play a prominent role in the pathological pathways of a group of predominantly small vessel vasculitis, otherwise known as ANCA-associated vasculitis (AAV).1 2 This distinctly pauci-immune form of vasculitis includes granulomatosis with polyangiitis (GPA, formerly Wegener’s granulomatosis), microscopic polyangiitis (MPA) and eosinophilic granulomatosis with polyangiitis (EGPA, formerly Churg-Strauss syndrome).
The spectrum of AAV ranges from isolated organ involvement to life-threatening fulminant disease. The prognosis in untreated systemic GPA was initially poor, with mortality rates of 80% within 1 year and with a mean survival time of 5 months.3 With the introduction of glucocorticoids and cyclophosphamide in the management of AAV in the 1960s, significant advances have been made in survival.4 The 1-year, 5-year and 10-year survival rates in patients with GPA are now reported to range between 81%–95%, 73%–83% and 55%–75%, respectively.5–13 Similar improvements were also noted in MPA and EGPA studies. With treatment, MPA survival rate at 1 year is 80%, 5 years 45%–85% and 10 years ~74%.14–17 Recent EGPA studies have estimated 5-year survival rates at 89%–97%.18 19
Despite improving survival, patients with AAV still remain at a higher risk of death relative to the general population.10 Standardised mortality ratio (SMR) provides an estimate of the true death risk, as it compares the number of observed patient deaths with the number of expected deaths of age-matched and sex-matched individuals from the general population. Several studies have reported an elevated SMR for patients with AAV, ranging from 1.6 to 4.8,9 13 16 20–23 although others have found that contemporary mortality risks were not significantly different from the general population.19 22 24 25 The conflicting results from these reports may be due to biases from small sample sizes and cohort types (eg, community-based vs clinic-based).
The purpose of our study was to estimate all-cause mortality risk of patients with AAV through a systematic review and meta-analysis from observational studies.
Methods
Search strategies
A search was performed by an experienced research librarian (MDW) to identify primary studies and review literature using Medline and Embase databases on the Ovid platform. Records were captured for the full date range for each database through April 2015 (Medline from 1948, Embase from 1980) in any language. Database-specific indexing was used (Medline Medical Subject Headings (MeSH) and Embase subject headings), along with text words in titles and abstracts. Two search concepts were combined with the Boolean operator ‘AND’: (1) ANCA-associated vasculitis (AAV) or vasculitis, and (2) mortality or survival. Conference abstracts were captured with this approach, as they were not specifically excluded as a publication type. The exact search strategy is available as an online supplementary material (or available on request from the corresponding author).
Abstracts for all articles of interest were reviewed for relevance, that is those that reported mortality or survival data in AAV. Full papers of selected abstracts were retrieved and assessed for eligibility based on the inclusion criteria listed below. We also searched the reference lists of identified papers and conference abstracts for additional relevant publications.
All English-language peer-reviewed articles that met the following inclusion criteria were considered eligible: (1) clearly defined AAV identified by either the American College of Rheumatology (ACR) 1990 classification criteria26 27 or the 2012 Chapel Hill Consensus Conference (CHCC) on disease definitions,28 and (2) reported SMRs and 95% CI, or available data to calculate SMRs. In cases of duplicate data used in more than one study, the sample with the most up-to-date data was selected for review.
Data extraction
Two authors (JAT and ND) independently reviewed and assessed the selected articles for eligibility. From eligible studies, JAT and ND extracted data on year of publication, enrolment period, study design, country, population setting, definition of AAV, sample size and demographics, proportion of ANCA positivity, proportion of renal involvement at diagnosis, and survival or mortality data. Gender-specific SMR was also noted, where available. In two studies, we calculated the 95% CI for SMR from available information.9 20 In studies where the overall cohort was divided into time cohorts (by year of enrolment), each time cohort was computed as an individual cohort during meta-analysis.22 24 One study provided 1-year and 5-year SMRs, and the latter was selected for the meta-analyses,24 as the median or mean follow-up times for all studies were greater than 1 year. Any differences between the two authors (JAT and ND) were resolved by consensus together with a third author (JAA-Z).
Quality scores of included studies
We assessed study quality based on a 12-point scale that was adapted from previously published scales for observational studies.29 30 We used a similar scoring system in our previously published meta-analyses on the risk of mortality in rheumatoid arthritis31 32 and systemic lupus erythematosus.33 Points were allocated on an ordinal scale for each of the six items recorded: source of the study population (population based=2 points, clinic/hospital-based=1 point and undefined=0); cohort type (inception cohort=2, non-inception cohort=1 and undefined=0); definition of AAV (ACR or CHCC classification criteria=2, other validated classification criteria=1, and other predefined but non-validated classification criteria=0); ascertainment of death outcome (validated criteria=2, non-validated but clearly defined criteria (eg, death certificates)=1 and not mentioned=0); AAV exposure (≥10 years=2, ≥5 years and <10 years=1, and <5 years=0); and loss to follow-up (≤20%=2, >20% and ≤40%=1, and >40% or not mentioned=0). Studies with scores ≥7 points were considered higher quality and those with ≤6 points were lower quality studies. Two authors (JAT and ND) performed quality scoring independently, with differences resolved by consensus together with a third author (JAA-Z).
Statistical analysis
We calculated the meta-SMR for all-cause mortality in AAV, which is a weighted-pooled summary estimate of SMRs (weighted by the sample size of each study) using HEpiMA statistical software, V.2.1.2.0.34 A GPA meta-SMR was determined from study cohorts that included only GPA cases, excluding MPA and EGPA. Separate meta-SMRs were also calculated for men and women. Initial calculations were performed using SMRs from the individual studies on a log scale to approximate a normal sampling distribution. The resulting pooled values were then transformed back to the SMR scale. Results from the pooled statistics were based on the random-effects model. Statistical heterogeneity was assessed using the I2 statistic, which indicates the proportion of variation in effect size due to heterogeneity.35 Source of heterogeneity was determined by subgroup analysis. To do so, all included studies were stratified accordingly: population setting (population-based vs hospital/clinic-based samples), cohort type (inception vs non-inception), midpoint of enrolment periods (1980–1993, 1994–1999 and 2000–2005) and centre (single-centre vs multicentre). Furthermore, a univariate meta-regression analysis was then used to study and interpret the difference in meta-SMRs between the subgroups.36 The time cut-offs for our enrolment period analysis were chosen as such because of the increased usage of ANCA testing in the mid-1990s, and because in the early 2000s there was a paradigm shift in treatment strategies, with an emphasis on improving the safety profile of induction therapy.37
We evaluated the robustness of the results using jackknife sensitivity analysis, by repeated meta-SMR analyses with removal of a single study in succession each time.38
Assessment of publication bias/small-study effect
We constructed a funnel plot in which a measure of the study size is plotted as a function of the measure of interest.39 We used the log of the SMRs from individual studies as well as the log of precision (1/variance). This was done to detect publication bias (ie, bias resulting from the greater likelihood of studies with positive results to be published compared with negative results) or the small-study effect (ie, a tendency for treatment effect estimates in small studies to differ from those in larger studies).40 In the absence of publication bias and small-study effect, the distribution of the data points will be symmetric. Furthermore, we used Egger’s regression as an objective, quantitative test statistic to test for the presence of asymmetry in the data.41
Results
We screened 570 abstracts published over the last 38 years (324 Medline and 238 Embase and 8 from reference lists). A total of 58 studies were retrieved for detailed evaluation and 10 studies met the inclusion criteria (figure 1 and table 1). Forty-eight studies were excluded: 43 did not provide SMRs or data to calculate them, 3 were review papers and 2 included only patients with renal vasculitis. The complete list of references reviewed is available on request from the corresponding author.
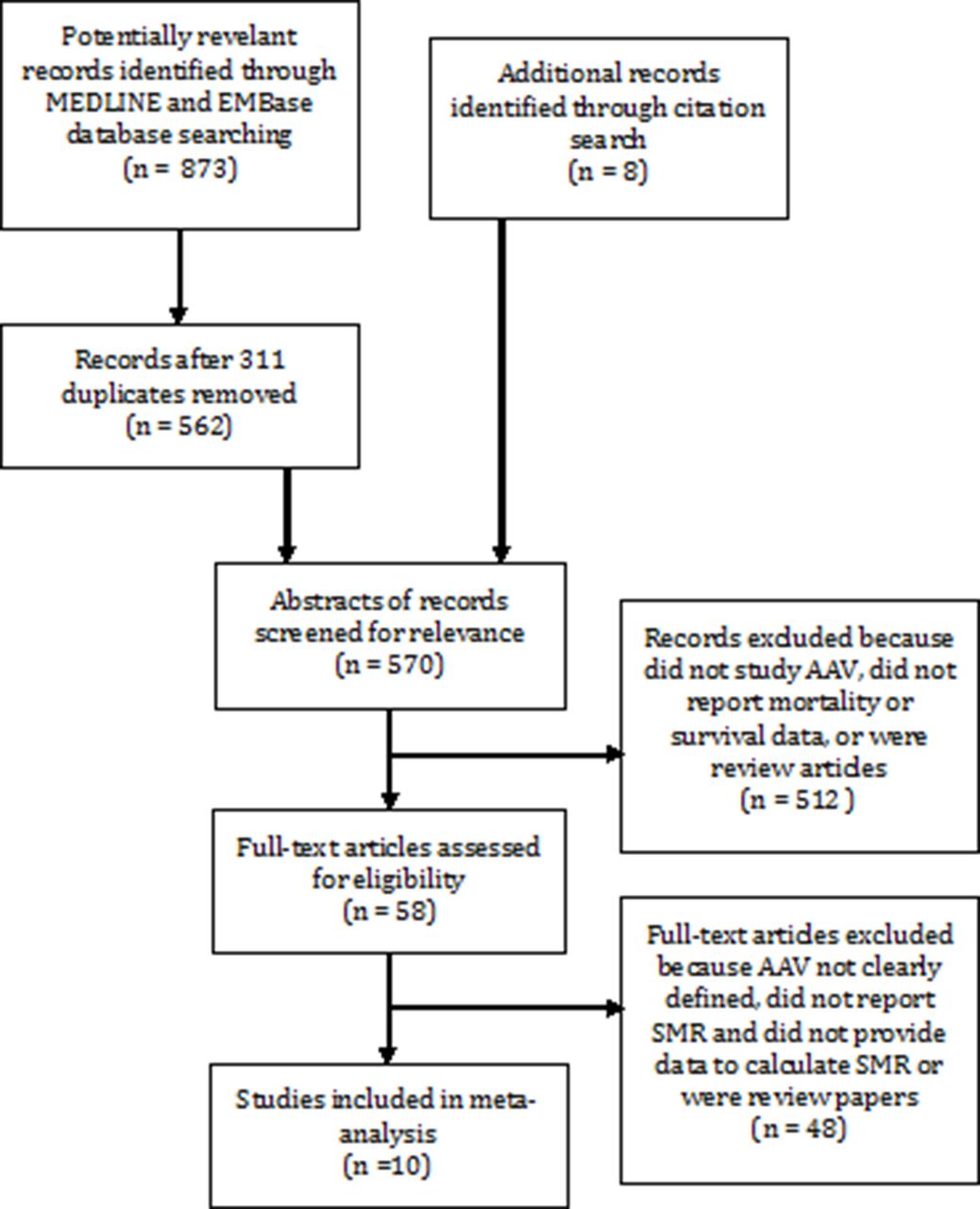
Flow chart of study selection from literature search. AAV, ANCA-associated vasculitis; ANCA, antineutrophil cytoplasmic antibodies; SMR, standardised mortality ratio.
Summary of studies included in meta-analysis
The 10 studies included 3338 patients with AAV (2619 with GPA, 501 with MPA, 185 with EGPA and 33 with renal limited vasculitis) enrolled from 1966 to 2009, and a total of 1091 observed deaths.9 13 16 19–25 Three were population-based studies (n=1691), whereas seven were hospital/clinic-based studies (n=1647). Four of these studies included only patients with GPA (n=1987).
There were 14 unique cohorts available for the meta-analysis. Overall, the mortality risk in patients with AAV was significantly increased when compared with the general population (meta-SMR: 2.71 (95% CI 2.26 to 3.24)) (see figure 2). Analysis on patients with GPA alone also showed a similar increase in risk of mortality (GPA meta-SMR: 2.63 (95% CI 2.02 to 3.43)). Five studies reported sex-specific mortality estimates with no differences in mortality risks between sexes (meta-SMR: 3.36 (95% CI 2.10 to 5.38) and 3.11 (95% CI 2.21 to 4.36) for women and men, respectively).

Meta-analysis of 10 studies on all-cause mortality in patients with ANCA-associated vasculitis. ANCA, antineutrophil cytoplasmic antibodies; GPA, granulomatosis with polyangiitis; meta-SMR, weighted-pooled summary estimates of standardised mortality ratios.
There was significant heterogeneity among the studies (I2=84.4%, 95% CI 72.6 to 96.3). Subgroup analyses showed that a number of factors might have influenced the mortality risk. Meta-SMRs were higher in population-based studies, in non-inception cohorts, in multicenter studies, and in cohorts enrolled prior to 2000 (table 2). All subgroups showed significantly increased mortality risk compared to the general population, although we observed a decreasing mortality trend in newer cohorts. Despite the differences in mortality within subgroups, only “center” was significantly associated with the observed heterogeneity using meta–regression analysis (p=0.05).
Overall mortality and sensitivity analyses for the 10 studies (14 unique cohorts) in patients with AAV
The results of the jackknife sensitivity analysis are shown in table 3. The meta-SMR remained significantly increased with every sequential study exclusion, with the point estimates ranging from 2.6 to 2.9 and the corresponding 95% CI remaining >1 in all analyses. This suggested that the meta-SMR result was robust and not skewed by a single dominant study.
Sensitivity analysis using the jackknife approach
The funnel plot is shown in figure 3. Each plot represents individual cohorts and the solid line is the log of the meta-SMR. The distribution of our data points was symmetrical; therefore, we concluded that there was no significant publication bias or small-study effect. The Egger’s test for presence of asymmetry in the data was not significant (p=0.308).

{kind=link}
{kind=link}
{kind=link}
Funnel plot of 14 cohort evaluating publication bias of mortality studies in ANCA-associated vasculitis. ANCA, antineutrophil cytoplasmic antibodies.
Discussion
This is the first systematic review and meta-analysis of observational studies assessing the mortality risk in patients with AAV. We found a 2.7-fold increased risk of death in patients with AAV when compared with the general population, with no differences between sexes. Analysis on studies that included only GPA cases also indicated a similar mortality risk. Of interest, mortality risks were higher in earlier cohorts, that is, those with their midpoint of enrolment periods that were between 1980–1993 and 1994–1999, relative to those between 2000–2005, with a trend towards improvement over time.
Our meta-analyses did not show any significant difference in mortality between women and men. Individual studies have reported contrasting mortality risks between genders, with some favouring women16 22 and others favouring men.9 13 25 It was interesting to note that in the study by Holle et al, young patients with AAV (median age: 31.7 years) were almost six times more likely to die than the age-matched general population, with the entire risk contributed by young men (SMR: 8.87 (95% CI 4.05 to 16.8)) as there were no deaths among the 80 women within the same cohort.22 The authors postulated that the higher mortality risk in young men was due to a higher frequency of renal involvement at diagnosis.
The secular decline in mortality risks was an interesting observation. Although the overall comparison between the cohorts was non-significant, there was a trend towards significance when we compared the earliest with the most recent cohorts (1980–1993 vs 2000–2005, p=0.06). A similar finding was reported in a recent mortality study in patients with GPA.42 In that study, 465 patients with GPA were followed over a 20-year period, and the authors found significantly improved HRs for mortality between an early cohort (1992–2002) and a late cohort (2003–2013) (4.34 (95% CI 2.72 to 6.92) vs 2.41 (95% CI 1.74 to 3.34), respectively, p=0.04). We hypothesise that this observation may have resulted from therapeutic improvements, earlier diagnosis with increased availability of ANCA testing and increased physician awareness, as well as improved overall patient care in terms of cardiovascular disease (CVD) risk modification, drug toxicity prevention strategies and cancer surveillance. Significant changes in the past decade on the way we treat patients with AAV include the use of pulsed cyclophosphamide and rituximab as less toxic therapeutic options.43–45 There were insufficient data to directly assess impact of treatment strategies on mortality in this meta-analysis. Future studies will be needed to confirm the improvement in mortality.
We found a significant difference in reported mortality risks from multicentre studies compared with single-centre studies. In fact, single-centre studies had the lowest meta-SMR of 1.89 (95% CI 1.17 to 3.07). The observed mortality difference between single-centre and multicentre studies was likely due to clinical differences in the respective patient populations, particularly in terms of the proportion and severity of renal involvement. Unfortunately, we were unable to test this hypothesis given that not all of the primary studies adequately described this type of data.
Unexpectedly, there was a trend towards higher mortality in the non-inception cohorts when compared with inception cohorts, although this did not reach statistical significance. One might expect higher mortality to be associated with inception cohorts as they capture the entire natural history up until the end of follow-up. However, inception cohorts may not follow patients for sufficiently long periods of time to capture late mortality risks, that is, deaths due to long-term disease or treatment-related complications such as cancer, cardiovascular disease or chronic renal failure. Non-inception cohorts by design would include prevalent as well as incident cases, and late mortality may be captured as the observation time begins at any point of the natural history. Unfortunately, we were unable to compare mean disease duration for the inception versus non-inception cohorts given that some reported mean times (n=5), some median times (n=6) and others none provided (n=2).
It was also interesting to note the trend for increased risk of death in studies that were population-based compared with those that were hospital/clinic-based. The risk estimates from population-based studies were more consistent, whereas there was wider variability in the estimates from hospital/clinic-based studies. The variability in the latter subgroup was not unexpected, given the likelihood of biases inherent in selected or referral cohorts. We suggest that further research in population-based cohorts is necessary to add to the current pool of knowledge.
Our study has several limitations. A common issue with meta-analyses is the comparability of the cohorts and the appropriateness of the comparison. We included cohorts that were clinically different in terms of enrolment period, AAV subgroups, classification criteria, follow-up, disease severity and study design. We adopted the random-effects model to incorporate the between-study heterogeneity into the analysis and provided an objective measure of the heterogeneity in the form of I2. Significant heterogeneity was detected, as expected in meta-analyses of observational studies.40 From the univariable meta-regression analysis, ‘center’ and ‘enrolment period’ were possible explanations for the heterogeneity (p=0.05 and p=0.06 (cohorts 1980–1993 vs 2000–2005), respectively). Furthermore, we performed a limited multivariable meta-regression analysis using these two variables. However, both variables were not significant predictors in the multivariable model. For this reason, our findings suggest that study centre is associated with between-study heterogeneity, but its effects may be confounded by enrolment period.
The remaining between-study heterogeneity may be partially explained by the variability of renal involvement in the study cohorts. However, the lack of uniformity in the definition of ‘renal involvement’ in the studies did not allow for grouping into a categorical ‘renal characteristic’, which would be necessary for meta-regression analysis. In addition, we were also unable to include ‘quality score’ in our meta-regression analysis as we only had one study scored as a lower quality study (≤6).
Current available data allowed us to report a meta-SMR on GPA, but not MPA or EGPA. A report on SMRs for each disease subcategory would be more clinically relevant than an overall SMR for AAV as they are clinically distinct diseases. However, the SMR for AAV may serve as a reference point for future studies seeking to compare mortality risk differences over time.
In our meta-analysis, the SMR evaluated the mortality risk adjusted only for age and gender but did not account for other confounders. However, there is no method for adjusting the results of meta-analyses using SMRs. Meta-analyses on studies assessing risk factors or predictors of mortality in AAV are required to address these issues.
In summary, our meta-analysis indicated that there was a 2.7-fold increase in mortality among patients with AAV compared with the general population. The pooled SMR for only patients with GPA was elevated at 2.6 times the general population. The risk of death was elevated for both male and female patients with AAV, with no significant difference between the genders. Furthermore, there was a trend towards improvement in mortality risks over time, which warrants further investigation. There is a need for longitudinal studies in contemporary cohorts to evaluate mortality benefits of modern therapies.
Acknowledgments
The authors would like to thank Mary-Doug Wright (MDW), who has been responsible for the literature search, and Lynn Nowoselski for her work editing this manuscript. Dr J Antonio Avina-Zubieta is the British Columbia Lupus Research Scholar, a Schola from The Micheal Smith Foundation for Health Research and a Research Scientist from the Arthritis Research Canada.
References
Footnotes
Contributors JAT and JAA-Z conceived and designed the study. JAT and ND screened titles and abstracts for inclusion and extracted the data. All authors were responsible for data analysis and interpretation. JAT drafted the manuscript. All authors contributed to critical review of the manuscript and have read and approved the final manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.