Article Text

Abstract
Background Glucocorticoids are the cornerstone treatment of polymyalgia rheumatica (PMR) but induce adverse events.
Objectives To evaluate the efficacy and safety of first-line tocilizumab in PMR.
Methods In a prospective open-label study (ClinicalTrials.gov: NCT01713842), 20 glucocorticoid-free patients fulfilling Chuang's PMR criteria, with symptom onset within the last 12 months and a PMR activity score (PMR-AS) >10, each received three tocilizumab infusions at 4-week intervals, without glucocorticoids, followed by oral prednisone from weeks 12 to 24 (0.15 mg/kg if PMR-AS ≤10 and 0.30 mg/kg otherwise). The primary end point was the proportion of patients with PMR-AS≤10 at week 12.
Results Baseline median PMR-AS was 36.6 (IQR 30.4–43.8). At week 12, all patients had PMR-AS≤10 and received the low prednisone dosage. Median PMR-AS at weeks 12 and 24 was 4.5 (3.2–6.8) and 0.95 (IQR 0.4–2), respectively (p<0.001 vs baseline for both time points). No patient required rescue treatment. Positron emission tomography-CT showed significant improvements. The most common adverse events were transient neutropenia (n=3) and leucopenia (n=5); in one patient, the second tocilizumab infusion was omitted due to leucopenia.
Conclusions Tocilizumab monotherapy is effective in recent-onset PMR. Randomised controlled trials are warranted.
Trial registration number NCT01713842.
- Polymyalgia Rheumatica
- Treatment
- Disease Activity
- Magnetic Resonance Imaging
- DMARDs (biologic)
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Glucocorticoids are the therapeutic mainstay in polymyalgia rheumatica (PMR).1 ,2 However, their adverse effects (ie, osteoporosis, diabetes and hypertension) are of particular concern in elderly patients.3 ,4 Among other tested drugs,5 ,6 only methotrexate7 was effective. Tocilizumab is a humanised antibody to the soluble interleukin-6 receptor that may be effective in PMR.8–10
The PMR activity score (PMR-AS)11 relies on five variables: morning stiffness (in minutes), elevation of the upper limbs (rated 0–3), physician's global assessment and pain intensity on 10-point visual analogue scales (VASs) and C reactive protein (CRP) level in mg/dL; the erythrocyte sedimentation rate (ESR) can replace CRP.12 PMR-AS<7 defines low-disease activity and PMR-AS >17 high-disease activity.11 ,12 However, for making treatment decisions in everyday practice, PMR-AS ≥10 was the best cut-off13 to define a flare14 and guide glucocorticoid dosage adjustments.15
We performed a 24-week, open-label, longitudinal, prospective study of the safety and efficacy of tocilizumab in recent-onset PMR (Tolerance and Efficacy of Tocilizumab in Polymyalgia Rheumatica study).
Patients and methods
Study design, setting and participants
The protocol was registered on Clinicaltrials.gov (NCT01713842). Tocilizumab was given as three intravenous infusions, at baseline then 4 and 8 weeks later, in a dosage of 8 mg/kg. The primary end point was evaluated at week 12.
From weeks 12 to 24, patients were to receive prednisone, in a low dosage of 0.15 mg/kg/day if their PMR-AS was ≤10 and in the standard dosage of 0.3 mg/kg/day otherwise. The PMR-AS was determined every four weeks; if ≤10, the prednisone dosage was decreased by 1 mg every two weeks and if >10 the dosage was increased from low to standard or, in patients already on the standard dosage, by 5 mg (figure S1 shows the study design).
Setting and participants
Patients were recruited at two university hospitals in France. Inclusion criteria were PMR meeting Chuang's criteria,16 with onset within the past 12 months, active disease defined as PMR-AS>10 and either no history of glucocorticoid therapy for PMR or glucocorticoid therapy for no longer than 1 month stopped at least 7 days before inclusion; informed consent to the study; age 50–80 years; any non-steroidal anti-inflammatory drug (NSAID) therapy stopped at least 2 days before inclusion; ESR≥40 mm/h or CRP≥10 mg/dL; and no evidence of other inflammatory rheumatic or connective disease. Exclusion criteria were clinical symptoms suggesting giant-cell arteritis; immunosuppressive therapy; uncontrolled dyslipidaemia or cardiovascular disease; chronic infection; evidence of hydroxyapatite crystal disease or chondrocalcinosis or severe osteoarthritis of the hip and/or shoulder; symmetrical peripheral arthritis; active thyroid disease and drug-related myalgia.17
Data collection
At each visit, the patients completed three 100 mm VASs, for fatigue, global disease activity and pain; and the short form 36 (SF36) quality-of-life questionnaire. The absence of giant-cell arteritis was checked.
B-mode ultrasonography, MRI of the shoulders and pelvic girdles and 18fluorodeoxyglucose positron emission tomography/CT (PET-CT) were performed at baseline then 2 and 12 weeks later.
Outcomes and follow-up
The prespecified primary end point was the proportion of patients whose PMR-AS was ≤10 at week 12. Secondary end points included the PMR-AS response and the PMR-AS (ESR) response (used to eliminate bias due to the direct effect of tocilizumab on CRP), at weeks 2, 4, 8, 12, 16, 20 and 24. Changes in shoulder and hips-girdle imaging findings from baseline to weeks 2 and 12 were evaluated using semi-quantitative scores. We assessed changes from baseline to each evaluation time point in VAS scores, SF36 scores, CRP level and ESR.
Adverse events were recorded at each visit from baseline to week 24 according to the Medical Dictionary for Regulatory Activities. Data were collected until the end of prednisone therapy; clinical events, time to prednisone discontinuation and median prednisone dose were recorded.
Statistical analysis
We estimated the required sample size based on the CI of the proportion of patients in remission (PMR-AS≤10) at week 12. Including 20 patients and assuming a 75% (15/20) remission rate would produce a CI of 50.6–90.4, indicating a >50% true remission rate.
We described continuous variables as median and IQR and categorical variables as n (%). To compare values between two time points, we chose the Wilcoxon signed-rank test for paired data and the McNemar test for categorical data.
The potential glucocorticoid-sparing effect of tocilizumab was assessed by comparing the prednisone dosage at week 24 to the cumulative prednisone dosage indicated by the British Society for Rheumatology (BSR) recommendations1 (0.30 mg/kg/day for 3 weeks then taper in the absence of giant-cell arteritis symptoms to 12.5 mg/day for 3 weeks then 10 mg/day for 4–6 weeks then 1 mg decrease every six weeks). We performed a sensitivity analysis using the initial dosage and taper recommended by the BSR,1 that is, 15 mg/day irrespective of body weight.
We used SAS, V.9.3 (SAS Institute, Cary, North Carolina, USA) for all analyses.
Results
Patient characteristics
The analysis included 20 patients who received at least one tocilizumab infusion (see online supplementary figure S2), 13 males and 7 females, with a median age of 66.9 years (62.0–72.5) and a median disease duration of 99 days (67–163). Median baseline PMR-AS was 36.65 (30.45–43.85); 18 (90%) patients had shoulder and pelvic girdle pain with morning stiffness for a median of 180.0 (75.0–180.0) min. Systemic manifestations were fever (2/20 patients), >5% weight loss (3/20) and serum gamma-glutamyl transpeptidase elevation (9/20 patients). No patient had rheumatoid factors or peripheral arthritis.
Supplementary figures
Of the 20 patients, 19 met Chuang's criteria and 1 had a low ESR but elevated CRP (>40 mg/dL). Provisional American College of Rheumatology (ACR)/European League Against Rheumatism (EULAR) criteria were met by 18 (90%) patients, whereas 2 had no bilateral shoulder aching at inclusion. The global score without ultrasound was 6 in each of the 17 patients and 5 in 1 patient. With ultrasound, 15 (75%) had bilateral shoulder bursitis and all 20 had a score ≥6.18
All 20 patients had recent-onset disease, with a symptom duration <5 months in 15 patients (median 99 days; 25th–75th percentiles, 67–163). At inclusion, 7/20 (35%) patients had taken glucocorticoid therapy, always for <1 month and with discontinuation at least 7 days before inclusion; 9/20 (45%) had taken NSAIDs.
Efficacy
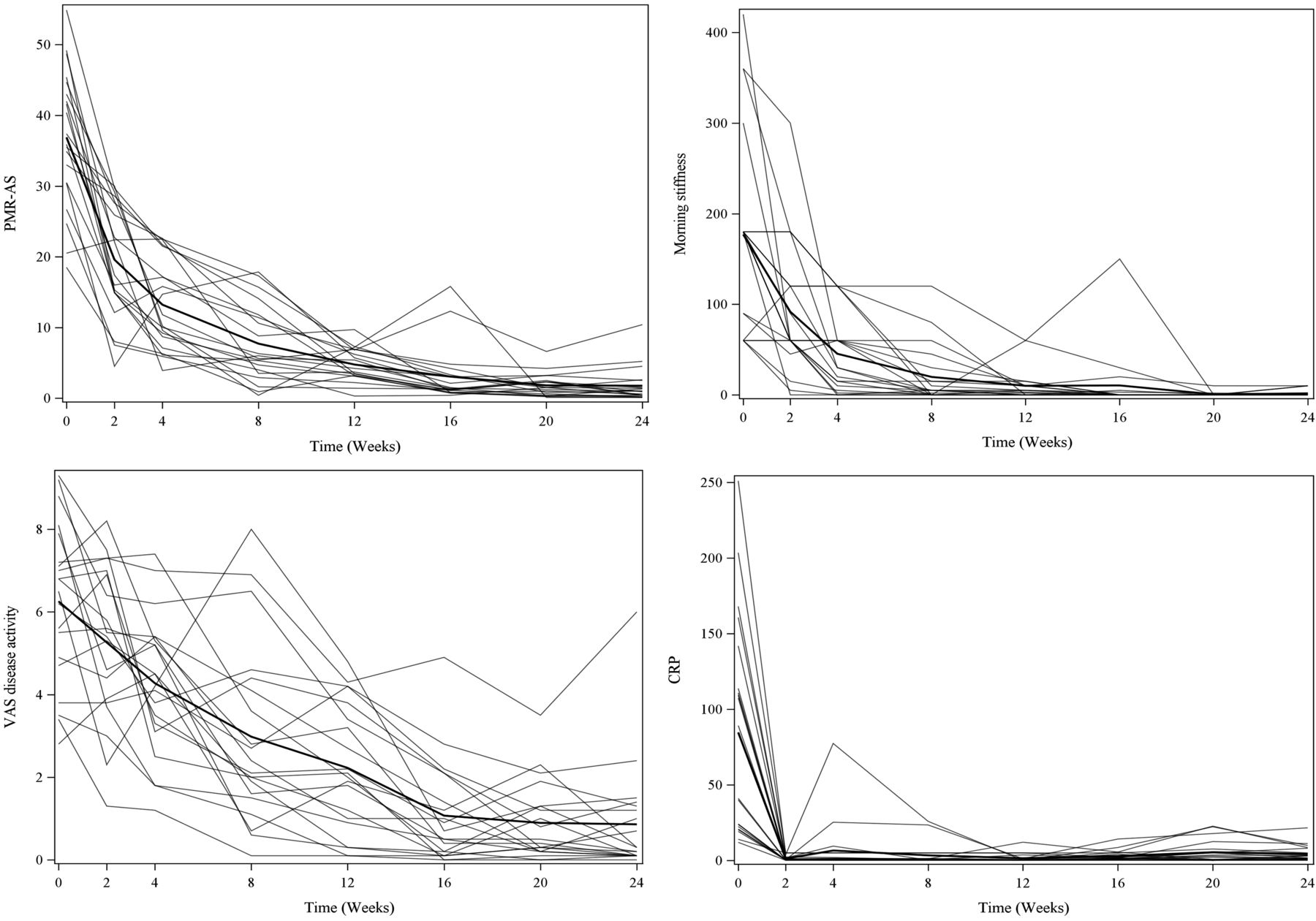
Tocilizumab efficacy was evaluated at weeks 4, 8 and 12. All patients achieved the primary end point of PMR-AS≤10 by week 12 (table 1). Median PMR-AS was 36.6 (30.4–43.8) at baseline and 4.50 (3.2–6.8) at week 12 (p<0.001). By week 2, there was already a significant improvement (median 19.75 (14.9–27.7)) (figure 1); PMR-AS was ≤10 in 3 (15%) patients at week 2, 9 (45%) at week 4 and 13 (65%) at week 8. Very low disease activity (PMR-AS<7)11 was noted in 1 (5%) patient at week 2, 4 (20%) at week 4, 12 (60%) at week 8 and 17 (85%) at week 12. PMR-AS (ESR) values also improved.
Global treatment efficacy during the tocilizumab and prednisone periods

{kind=link}
Efficacy of tocilizumab and prednisone on the polymyalgia rheumatica activity score (PMR-AS) and three of its components. CRP, C reactive protein; VAS, visual analogue scale.
No patient required rescue treatment during the first 12 study weeks. All patients were started on low-dose prednisone (0.15 mg/kg/day) at week 12; median starting dosage was 12 mg (9.0–12.5). At weeks 16, 20 and 24, the prednisone dosage was decreased according to the study protocol. Median PMR-AS improved significantly from weeks 12 to 24 (from 4.50 (3.2–6.8) to 0.95 (0.4–2.0)). No patient required rescue therapy or had a flare during the prednisone phase.
The median cumulative dose predicted by BSR recommendations,1 with an initial dosage of 0.3 mg/kg/day, was 2705.3 mg (2158.8–2848.4), which was significantly higher than the median cumulative dose in our patients (808.5 mg (673.3–866.3)) (p<0.001) at week 24 (see online supplementary table S1). The glucocorticoid-sparing effect of tocilizumab was 70.2%.
Supplementary table S1
Glucocorticoid-sparing effect of tocilizumab compared to standard glucocorticoid treatment in a starting dosage of 0.3 mg/kg/day or 15 mg/day
Follow-up was provided 1 year after the end of prednisone therapy, for a median of 12 (12–17) months after week 24 in 18 patients; two patients were lost to follow-up. Six months after week 24, only four patients were still on prednisone therapy and median daily prednisone dosage was 0. At the end of the follow-up, median cumulative prednisone dose was 560 mg (405–755.25). No patient had flares or giant-cell arteritis. One patient experienced a moderate relapse 2 months after prednisone discontinuation; she had received only two tocilizumab infusions, due to an adverse event, and she achieved a second remission after 4 weeks of prednisone therapy, 5 mg/day.
Table 1 reports the other secondary efficacy outcomes. CRP returned to normal within 2 weeks of tocilizumab initiation. All VAS scores decreased, and the decreases were largest for pain and disease activity. Both the physical and the mental components of the SF36 improved. No patient developed symptoms of giant-cell arteritis during follow-up.
Major improvements were noted in clinical and laboratory variables and in the PMR-AS, contrasting with only moderate improvements by PET-CT or MRI and no improvements by ultrasonography (table 2).
Findings from imaging studies at baseline and 2 and 12 weeks after tocilizumab initiation
Safety
Online supplementary table S2 reports the adverse events, serious adverse events and discontinuations due to adverse events. No cases of opportunistic infection, tuberculosis or death were recorded. Cancer unrelated to PMR was diagnosed in two patients. Of the 37 adverse events recorded in 14 patients during tocilizumab therapy, 22 were ascribed to tocilizumab. The most common tocilizumab-related adverse events were leucopenia (five instances in three patients) and neutropenia (seven instances in five patients). Leucopenia prompted a tocilizumab dosage decrease to 4 mg/kg at weeks 4 and 8 in three patients and withholding of the week 4 dose in another patient (see online supplementary figure S2). Three infections were classified as tocilizumab-related but were of moderate severity. Dyslipidaemia occurred on four occasions in three patients but resolved spontaneously. During the prednisone phase, 17 adverse events were reported in 10 patients, including 6 classified as prednisone related. Loss of control of pre-existing diabetes mellitus occurred in one patient. Severe insomnia was reported by two patients, including one in whom this symptom required acceleration of the prednisone taper. Dyslipidaemia occurred in one patient.
Supplementary table S2
Adverse events and serious adverse events per patient during the tocilizumab phase [weeks 0 to 12] and prednisone phase [weeks 12 to 24], reported using System Organ Class [SOC] terminology
Discussion
In our study, tocilizumab was effective in controlling recent-onset PMR when used alone, without glucocorticoid therapy. All patients achieved the primary end point by week 12 and required only low-dose prednisone after tocilizumab therapy; 85% of patients achieved very low disease activity (PMR-AS<7) by week 12. All secondary end points improved.
The response to tocilizumab seems slow. However, in a recent prospective ACR/EULAR study of 125 patients with PMR,18 ,19 only 71% of patients had a complete response to glucocorticoid therapy by week 4.
Four (20%) patients required tocilizumab dosage reductions due to leucopenia, but no serious adverse events were recorded. We recommend close monitoring of peripheral leucocyte counts during tocilizumab therapy for PMR. PET-CT showed moderate albeit significant improvements. However, limited data are available on tissue-level effects of tocilizumab in PMR, which probably differ from those seen in rheumatoid arthritis.
Limitations of our study include the non-randomised design, which was, however, appropriate for this proof-of-concept study. The PMR-AS was the only available AS but includes the CRP level, which tocilizumab affects directly. The use of other ASs or primary end points deserves consideration.20 Whether tocilizumab is a glucocorticoid-sparing agent in PMR requires confirmation.
Acknowledgments
The authors thank the French rheumatologists and general practitioners who referred their patients to the TENOR study. They are grateful to Marie Jezequel and Nathalie Bihannic (CIC) for centralising the material and to Audrey Le Goff-Coquet and Valentine Guiton (DRCI). They also thank the staff for their time and commitment to this work.
References
Footnotes
Handling editor Tore K Kvien
Funding Roche-Chugai provided an unconditional grant for the study and donated the tocilizumab
Competing interests None declared.
Patient consent Obtained.
Ethics approval This study was approved by the appropriate ethics committee (CPP Ouest VI).
Provenance and peer review Not commissioned; externally peer reviewed.