Article Text

Abstract
Objective To estimate the risk of tuberculosis (TB) in patients with rheumatoid arthritis (RA) both with and without exposure to biological therapy and to directly compare the risks between therapies.
Methods Data from the Swedish National Population Registers, Tuberculosis Register and the Swedish Biologics Register were used to conduct a prospective population-based national cohort study (2002–2011). We estimated the rate of incident TB in the general population and in a cohort of biological-naïve and biological-exposed patients diagnosed with RA. Cox models were used to estimate HRs with particular attention to risks by calendar and follow-up time and individual biologics.
Results Compared to the general population, RA patients not exposed to biologicals had a fourfold increased risk of TB (HR 4.2; 95% CI 2.7 to 6.7), which did not decline over calendar time. In contrast, the risk of TB in the biological-exposed RA population decreased since 2002 compared with biological-naïve; from HR=7.9 (95% CI 3.3 to 18.9) in 2002–2006 to HR=2.4 (95% CI 0.9 to 6.1) in 2007–2011. The HRs for most recent exposure to adalimumab and infliximab compared with etanercept were 3.1 (95% CI 0.8 to 12.5) and 2.7 (95% CI 0.7 to 10.9), respectively, and the HR for etanercept compared with biological-naïve RA was 1.7 (95% CI 0.6 to 4.6).
Conclusions In the past decade, the risk of TB has decreased among biological-exposed RA patients but remains higher than in biological-naïve RA patients. Most cases of TB in RA occur in biological-naïve RA patients, underscoring the elevated risk also in these patients.
- Rheumatoid Arthritis
- Tuberculosis
- Anti-TNF
- Treatment
Statistics from Altmetric.com
Introduction
Cases of tuberculosis (TB) associated with anti-tumour necrosis factor (anti-TNF) exposure in patients with rheumatoid arthritis (RA) have been reported from randomised controlled trials,1 ,2 spontaneous adverse event reports3–5 and observational studies.6–13 These studies, along with guidelines issued in the last decade in most countries, including Sweden, have led to increased vigilance, screening and treatment for latent TB before biological treatment initiation.14–16
The extent to which increased awareness and targeted pretreatment screening have reduced TB risk with anti-TNFs, as suggested in at least one study from Spain,17 remains less clear. Similarly, few studies have made head-to-head comparisons of individual anti-TNFs. These studies have been limited by small numbers of cases and short follow-up, especially for the more recently introduced anti-TNFs.6 ,7 Although risks with biologicals other than anti-TNFs are believed to be lower than risks with anti-TNFs,18 there is little substantiating evidence.19 It also remains unclear whether TB risks are ‘transient’ or persist years after biological treatment initiation and to what extent general increased clinical vigilance has affected the TB risk in biological-naïve RA. This is important as any risk estimates associated with biologicals must take into account the underlying TB risk in biological-naïve RA in the country and time period under study.10–12 ,20 ,21
Our aim was therefore to examine TB risks in the general population and in patients with RA both exposed and unexposed to biologicals since 2002 (following the first signals of increased TB risk and introduction of pretreatment TB screening in Sweden). We used a population-based and register-based prospective cohort design and linkage to a national TB register (to which reporting is mandatory) to estimate the risk of TB on a national level. Among individuals with RA exposed to biologicals, we directly compared the risk of TB between biological therapies.
Methods
Study population
A national population-based RA cohort was identified using the National Patient Register (NPR) (inpatient care 1969–2011 and outpatient, non-primary care 2001–201122) and the Swedish Rheumatology Quality Register (SRQ; 1997–2011). The inpatient component of the NPR is over 99% complete, and the outpatient specialist non-surgical care component is over 87% complete. Similar to our previous studies,23 ,24 we included individuals ≥18 years old with an RA diagnosis (≥2 visits with an International Classification of Diseases (ICD) code for RA in the NPR, with ≥1 visit to a rheumatology or internal medicine department and ≥1 in outpatient care). Patients with a diagnosis code for juvenile idiopathic arthritis, psoriatic arthritis, spondylarthritis, ankylosing spondylitis or systemic lupus erythematosus were excluded. In an analysis of 100 patients, using American College of Rheumatology (ACR) 1987 or ACR/European League Against Rheumatism (EULAR) 2010 criteria showed that 95% of the patients defined using this RA definition are correct (Kristin Widén, personal communication). Biological-exposed patients with RA were identified from the Swedish biologics register (1999–2011), a national population-based register contained within the SRQ. Data are entered by treating rheumatologists and shown to include approximately 90% of all biological-treated patients with RA in Sweden.25 Individuals with a history of biological treatment before 1 January 2002 were excluded from the study population. We identified a cohort of patients diagnosed with RA and unexposed to biological therapy (n=37 982, ‘biological-naïve’) and a cohort of patients with RA starting their first biological drug (‘biological-exposed’) at any time during the study period 1 January 2002 through 31 December 2011 (n=10 800). For each unique patient with RA, up to five general population comparators matched on sex, year of birth and residential county were identified from the National Population Register (n=175 972).
Covariates
Statistics Sweden provided data from the Total Population Register (containing census information) and the Education Register—quality of databases is managed through annual audits.26 Highest education level was categorised as ≤9 years, 10–12 years, >12 years of education or missing. Country of birth was categorised as Nordic, non-Nordic Europe and outside Europe. History of any visit with an ICD code for diabetes, cancer, chronic obstructive pulmonary disease (COPD) was collected from the NPR. Using each Swedish resident's unique personal identification number, we linked covariates to the study population.
TB assessment
Data on active TB diagnosis were retrieved from the TB register, and any individuals diagnosed with TB before start of follow-up (1 January 2002) or with latent TB were excluded. In Sweden, TB is managed at chest or infectious disease clinics, and clinicians are obliged to report to the TB register's web-based reporting system any individual they start on treatment for TB, whether verified or only on suspicion. Laboratories report any positive finding of Mycobacterium tuberculosis in the same system, linked to the clinician's report by the patient's unique personal identification number. If a laboratory report is not completed with a clinical report within a few weeks, the treating physician is contacted and asked to send one. Quality of the data retrieved is monitored on a weekly basis. This results in a coverage of 100% for all cases verified by culture. Of all TB cases reported during the last 5 years in Sweden, approximately 60% were pulmonary TB and 80% were verified by culture.
Exposure assessment
Date of start of biological treatment (prescription of abatacept, adalimumab, anakinra, certolizumab, etanercept, golimumab, infliximab, rituximab and tocilizumab as first or subsequent biologic) as entered by the treating rheumatologist was obtained from the Swedish Biologics Register. We defined exposed person-time (‘at-risk windows’) in three ways: (1) ‘current exposure/on drug’—follow-up until discontinuation of biological plus 90 days (any event occurring >90 days after discontinuation was considered unexposed); (2) ‘most recent exposure’—follow-up until start of a subsequent biological treatment ignoring any discontinuation date of the previous biological; and (3) ‘ever exposed’—follow-up continued until end of study regardless of starting a second biological and/or discontinuation. These exposure windows allow us to examine whether biologicals confer a short-term (window 1) or long-term (window 3) risk and whether censoring at time of switching drugs (windows 1 and 2) or ignoring switching (window 3) affected risk estimates. A description of these ‘at-risk windows’ is presented in the paper by Dixon et al.27
Follow-up
Emigration date was retrieved from the Total Population Register, and date of death was retrieved from the Cause of Death Register, which includes all deaths in Sweden. Individuals were followed for incident TB until 31 December 2011, death, emigration or date of TB diagnosis, whichever came first. In analyses comparing TB risk in the biological-naïve RA population with the general population, person-time was censored at first start of a biological therapy. Biological initiators during follow-up contributed person-time (and any events during this time) to the biological-naïve RA cohort up until biological initiation.
Statistical analysis
Crude incidence rates (IRs) of TB per 100 000 person-years (py) were calculated in the biological-naïve, biological-exposed and general population cohorts. Cox models adjusting for age as a continuous variable, sex, country of birth, education, history of diabetes, COPD and cancer as indicator variables were used to calculate HRs and 95% CIs (HR; 95% CI). If estimates became unstable due to small numbers of events, we either collapsed the variable into fewer categories or dropped it from analysis. We estimated the HR for TB comparing biological-naïve RA the general population overall and stratified by calendar time (2002–2006 and 2007–2011). We estimated the HR for TB comparing biological-exposed RA with biological-naïve, defining exposure as first ever biological initiation. To investigate change in risk over time, we stratified HRs by calendar year and follow-up time and calculated a p for heterogeneity (p-het) using a Wald test. Lastly, we calculated the rate of TB for each biological and calculated drug-specific HRs using etanercept (the largest group) as reference. In analyses comparing biologicals, multivariable HR estimates using three different exposure window definitions were calculated and switchers could contribute to more than one drug. In a sensitivity analysis, we restricted the head-to-head comparison to biological initiators only. Analyses were performed using SAS V.9.2.
Results
TB risk in biological-naïve RA versus the general population
Characteristics of the study populations at baseline are presented in table 1. We identified 32 biological-naïve RA patients with TB over 223 661 py of follow-up (IR 14.3 per 100 000 py; 95% CI 9.8 to 20.2) and 43 general population comparators with TB over 1 227 981 py (IR 3.5 per 100 000 py; 95% CI 2.5 to 4.7). Overall, 63% of the biological-naïve TB cases and 91% of the general population were culture-verified (table 2). For the 12 biological-naïve cases not verified by culture, diagnosis was made on clinical suspicion in all and supported by histopathological findings in four of the cases. Compared to the general population, RA patients unexposed to biologicals had a fourfold increased risk of TB (HR 4.2; 95% CI 2.7 to 6.7) with no change over calendar time (HR 2002–2006 4.4; 95% CI 2.3 to 8.2, HR 2007–2011 3.9; 95% CI 2.0 to 7.8, p-het 0.8). Age, education and country of birth were statistically significantly associated with TB, but adjustment did not greatly change HR estimates.
Baseline characteristics of the biological-naïve and biological-exposed cohorts of patients with RA and matched individuals from the general population 2002–2011
Characteristics of incident TB cases identified in the general population, biological-naïve RA and biological-exposed RA populations, 2002–2011
TB risk in biological-exposed versus biological-naïve RA
We identified 18 TB cases over 48 228 biological-exposed py (IR 39.4 per 100 000 py; 95% CI 23.7 to 61.5) (table 2). TB diagnosis was verified by culture in 72% of cases. All of the cases with negative cultures had a clinical course compatible with TB and three also had histopathological findings of granulomas. The distribution of biological exposures in this study reflects the national treatment guidelines as well as the calendar time of approval, with the majority (95%) of person-time on first biological consisting of exposure to anti-TNFs. Fourteen of the biological-exposed TB cases occurred during/after first biological treatment. Three cases had been exposed to two biologicals and one had been exposed to four. All exposed cases were exposed to either etanercept, infliximab, adalimumab or rituximab. Time between biological initiation and TB diagnosis ranged from 4 months to 5 years with a mean of 1.6 years (SD 1.4) and median of 1.2 years (IQR 1.1).
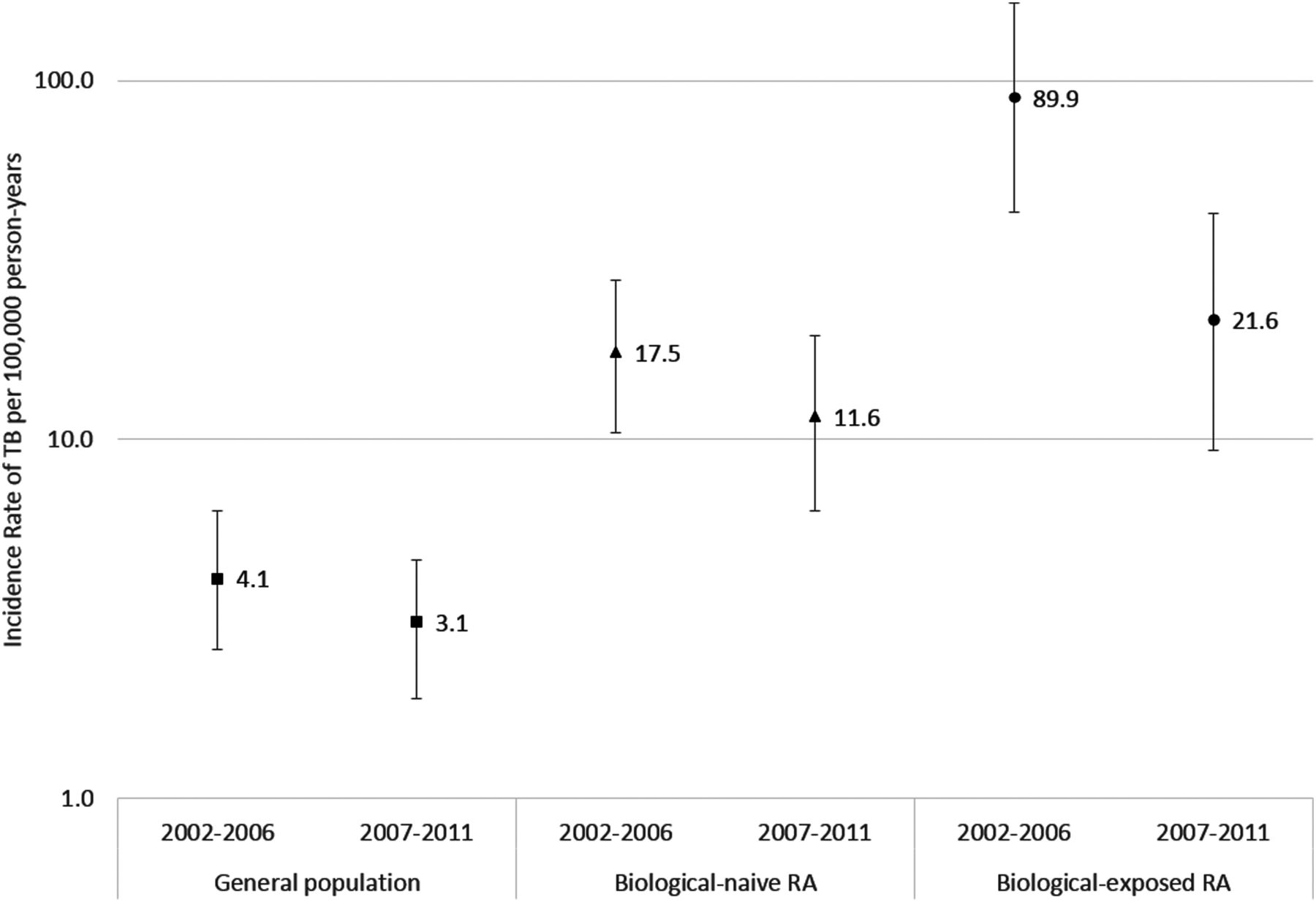
The biological-exposed RA population from 2002 to 2006 had a TB IR of 89.9 per 100 000 py compared with 24.2 in 2007–2011 (figure 1, table 3). Overall, RA patients who were ever biological-exposed had a multivariable-adjusted HR of 4.4 (95% CI 2.3 to 8.5) compared with biological-naïve (table 3). The relative risk of TB comparing biological-exposed to biological-naïve RA declined over calendar time (2002–2006 HR 8.0 vs 2007–2011 HR 2.4). Biological-exposed RA patients in 2002–2006 had an increased risk of TB compared with those exposed in 2007–2011 (HR 3.7; 95% CI 1.4 to 9.4). The relative risk of TB also decreased with increasing follow-up time (<5 years HR 7.8 vs ≥5 years HR 1.2) (table 3).
HRs of incident TB according to biological exposure in the biological-naïve and biological-exposed RA populations 2002–2011 overall, stratified by calendar period and follow-up time
{kind=link}
Incidence rates of tuberculosis per 100 000 person-years and 95% CIs in patients with rheumatoid arthritis (biological-naïve and biological-exposed) and matched individuals from the general population in Sweden, 2002–2006 and 2007–2011.
TB risk comparing biologicals
Cases, person-time, IRs and adjusted HRs of TB for each biological are presented in table 4. Allowing for patients to contribute person-years to multiple biologicals, 89% of the person-time was exposed to anti-TNFs, the majority of which was etanercept (39% of exposed person-time), followed by infliximab (25%), adalimumab (24%), golimumab (0.5%) and certolizumab pegol (0.4%). The HR comparing etanercept-exposed patients with biological-naïve was 1.7 (95% CI 0.6 to 4.6). Restricting to those whose first biological was etanercept, the HR was 2.1 (95% CI 0.8 to 5.6). Among the three most commonly used anti-TNFs, the crude rate of TB was highest for adalimumab and infliximab, and lowest for etanercept. Among the non-anti-TNFs, there was one TB case exposed to rituximab (with no previous exposure to an anti-TNF).
IRs and HRs of TB by biological exposure with etanercept as reference group according to three exposure definitions (ever-exposed, most recent exposure and current exposure/on drug) 2002–2011
Table 4 lists the HRs for each biological and each exposure window. Using the ‘most recent’ exposure window and etanercept-exposed as the reference group, the adjusted HRs for adalimumab, infliximab and rituximab were 3.1, 2.7 and 0.6, respectively. Using the ‘current/on drug’ exposure window, the adjusted HRs for adalimumab, infliximab and rituximab were 4.7, 2.4 and 1.4, respectively (table 4). Results restricting to first biological exposures only are presented in online supplementary table S1.
TB-screening procedures in biological-exposed patients who developed active TB
Two cases had been screened with normal chest X-ray results and negative purified protein derivitive (PPD) yet they developed active TB. One case developed active TB after being newly infected by M tuberculosis when already biological-exposed. One case was diagnosed with disseminated TB at autopsy and TB was deemed as the cause of death. One case with a positive PPD was on prophylactic treatment with isoniazid (INH) for 4 months but developed active TB caused by an INH-resistant M tuberculosis strain. In the majority of cases, TB screening was either not performed, not fully documented or incomplete, yet in retrospect most patients had risk factors for earlier TB exposure (table 5). There is, however, no reporting standard for the documentation of any screening measures taken; lack of information on screening therefore does not mean it was not performed. The important predictors of TB in the RA population were age and country of birth.
Screening information for biological-exposed patients with rheumatoid arthritis diagnosed with tuberculosis in Sweden 2002 through 2011 (n=18)
Discussion
Patients with RA exposed to biologicals are at an increased risk of TB, but this risk has decreased over the past decade likely due to increased general vigilance and the introduction of pretreatment screening. In recent years (2007–2011), biological-exposed RA patients had a 2.5-fold higher risk of TB compared with biological-naïve RA patients. The risk of TB was significantly elevated only within the first 5 years of biological initiation. Between-drug comparisons of the three most common TNF inhibitors showed the lowest risk among those exposed to etanercept, though these estimates were based on small numbers.
Previous studies from the USA, Canada and Europe have estimated the risk of TB in biological-naïve patients with RA to be approximately 2–4 times that of the general population.10 ,13 ,20 ,21 These findings are similar to the fourfold increased risk of TB in the RA population observed in our study. One study from Korea reported a ninefold increased risk, with CIs that overlap ours.12
An increased TB risk associated with anti-TNF exposure was first identified by spontaneous adverse event reports, randomised controlled trials and open-label extension studies.19 The lack of a comparison group and/or small number of cases in these studies make it hard to assess the magnitude of increased TB risk that anti-TNFs confer. In a previous observational study using the Swedish inpatient register (1999–2004), we identified 15 anti-TNF-exposed TB cases (defined as hospitalisations and spontaneous reports of TB).10 In comparison, our current study includes patients diagnosed with RA in the outpatient setting, which may better represent the average RA patient, and TB diagnoses obtained from a mandatory reporting system. Follow-up from 2002 through 2011 allowed us to make a more current estimate of TB risk in a setting in which clinicians are aware of TB risk and patients are screened before biological initiation. The focus of this paper was risks in a more global sense rather than investigations of specific screening measures or adherence to screening programmes. Our results indicate, however, that a structured medical history regarding risk of earlier TB exposure is an important part of screening due to the possibility of false-negative tests.16 ,28 ,29
Few studies have directly compared the risk of TB among biologicals. The French RATIO case–control study reported that the ORs for adalimumab and infliximab were higher than etanercept (OR 21; 95% CI 4.8 to 92.8), which is similar to our findings, although our point estimates are lower.6 The British Society for Rheumatology Biologics Register (BSRBR) study, which was more similar in design to our study, compared the risk of TB among anti-TNFs, but no direct comparison with the biological-naïve RA population could be made because no biological-naïve TB cases were identified.7 The British study included less biological-exposed person-time, especially for more newly introduced therapy such as adalimumab (28 447 py total, 7634 py on adalimumab). In comparison, we included a total of 41 700 py exposed to biologicals and 9635 py on adalimumab (‘on drug’ at-risk window). The BSRBR observed a threefold to fourfold increased risk of TB associated with infliximab and adalimumab compared with etanercept, which is similar to our findings. In contrast to previous studies, we included exposure to non-TNF biologicals and newer anti-TNFs. Follow-up time was limited for those drugs that have been on the market for a shorter time (eg, tocilizumab, golimumab and certolizumab pegol), causing estimates of risk for these drugs to have wide CIs.
Biological exposure in this study may have been misclassified if the discontinuation date does not reflect the true end of the time at risk. To address this, we used different exposure window definitions and found that estimates were similar across different ‘at-risk’ windows. We minimised misclassification by using data on biologicals collected from the Swedish Biologics Register, which has been shown to have excellent coverage.25 Channelling bias may have affected our results if people at a higher risk for TB were more likely to be prescribed drugs believed to carry a lower risk such as etanercept or a non-biological disease-modifying antirheumatic drug. This would bias the rates of TB in the etanercept, non-TNF biologicals and/or biological-naïve patients upward.
Our results may be affected by differential outcome ascertainment if the exposed population was monitored more carefully for TB than the unexposed. To minimise this bias, we used a nationwide TB register with excellent coverage of all patients diagnosed with culture-verified TB. There was a lower proportion of culture-verified TB in the RA population compared with the general population in our study. The level of suspicion of TB is higher in this group, so they were more likely to get full treatment with negative cultures. After careful review of the TB cases, we are confident that these were true TB cases. Notification of non-culture-verified TB cases might not be as complete, resulting in missing some patients with negative cultures. Since all patients who start TB treatment are normally reported to the register, the number of cases not captured by the register is likely small. The rates in the general population in our study are similar to that of the Swedish population with the same age and sex distribution, showing that estimates in our study using the register represents the true rate of TB in Sweden.
Sweden has an overall TB incidence of 6.8/100 000 py, which is lower than the UK (14/100 000 py) and Spain (15/100 000 py) but higher than the USA (3.9/100 000 py) and France (4.3/100 000 py).30 Generalisability of our results to countries with different rates may be limited, but TB rates would affect both the exposed and unexposed equally, making the ratio of rates similar across countries.
Conclusion
Although the risk of TB with TNF inhibitors has declined over calendar time, increased awareness and screening has not removed this risk. Most cases of TB in RA occur in biological-naïve patients, underscoring the elevated risk also in RA patients unexposed to biologicals.
Acknowledgments
To all patients and rheumatologist for entering information into the Swedish Rheumatology quality of care register. We wish to thank Maud Rütting, ARTIS register, for her assistance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Handling editor Tore K Kvien
Collaborators The ARTIS Study Group: JA, EB, NF, Lars Cöster, Helena Forsblad, Peirre Geborek, Lennart Jacobsson, Lars Klarskog, Lars-Erik Kristensen, Staffan Lindblad, Solbritt Rantapää-Dahlqvist, Ronald van Vollenhoven.
Contributors Conception and design: EVA, JA, EB, NF, JB, the ARTIS Study Group. Data collection: JJ, EVA. Analysis and drafting of manuscript: EVA. Critical revision of manuscript and final approval: all authors.
Funding The ARTIS Study Group conducts scientific analyses using data from the Swedish biologics register (ARTIS) run by the Swedish Society for Rheumatology. For this register, the Swedish Society for Rheumatology has received funding, independent of the conduct of these scientific analyses, from Merck, BMS, Pfizer, Abbott Laboratories, SOBI, UCB and Roche. These entities were allowed to comment on the findings before submission, although all final decisions resided with the investigators. This specific study further received funding from the Swedish Foundation for Strategic Research and from the Swedish public–private COMBINE research consortium. These entities had no influence on the data collection, statistical analyses, manuscript preparation or decision to submit.
Competing interests None.
Ethics approval Karolinska Institutet.
Provenance and peer review Not commissioned; externally peer reviewed.