Article Text

Abstract
Vitamin D is frequently prescribed by rheumatologists to prevent and treat osteoporosis. Several observations have shown that vitamin D inhibits proinflammatory processes by suppressing the enhanced activity of immune cells that take part in the autoimmune reaction. Moreover, recent evidence strongly suggests that vitamin D supplementation may be therapeutically beneficial, particularly for Th1-mediated autoimmune disorders. Some reports imply that vitamin D may even be preventive in certain disorders such as multiple sclerosis and diabetes type 1. It seems that vitamin D has crossed the boundaries of calcium metabolism and has become a significant factor in a number of physiological functions, specifically as a biological inhibitor of inflammatory hyperactivity.
- 1,25(OH)2D3, 1,25-dihydroxyvitamin D3
- 25(OH)D, 25-hydroxyvitamin D
- GM-CSF, granulocyte-macrophage colony stimulating factor
- IFNγ, interferon γ
- IL, interleukin
- NFκB, nuclear factor κB
- SLE, systemic lupus erythematosus
- VDR, vitamin D receptor
Statistics from Altmetric.com
- 1,25(OH)2D3, 1,25-dihydroxyvitamin D3
- 25(OH)D, 25-hydroxyvitamin D
- GM-CSF, granulocyte-macrophage colony stimulating factor
- IFNγ, interferon γ
- IL, interleukin
- NFκB, nuclear factor κB
- SLE, systemic lupus erythematosus
- VDR, vitamin D receptor
Autoimmune diseases are the third leading cause of morbidity and mortality in the industrialised world, surpassed only by cancer and heart disease.1 Despite this relatively high prevalence rate, the aetiology and pathogenesis of most autoimmune disorders remain obscure and a number of factors have been implicated in their pathogenesis. One of the most recent agents found to be associated with autoimmunity is vitamin D.
Vitamin D has multiple immunosuppressant properties. Supplementation of vitamin D was shown to be therapeutically effective in various animal models such as autoimmune encephalomyelitis,2,3 collagen-induced arthritis,4 type 1 diabetes mellitus,5 inflammatory bowel disease,6 autoimmune thyroiditis7 and systemic lupus erythematosus (SLE),8 and in some models of SLE it prevented disease development. A recent study showed that high circulating levels of vitamin D were associated with a lower risk of future multiple sclerosis.9
PHYSIOLOGY OF VITAMIN D
The classic prominent function of vitamin D is regulation of calcium homeostasis, which is primarily maintained via bone formation and resorption.10–12 Homeostasis is maintained in addition through the interaction of vitamin D with the parathyroid, kidney and intestinal tissues.13
Vitamin D can be ingested orally or can be formed endogenously in cutaneous tissue following exposure to ultraviolent B light.14 Vitamin D3 from both sources is metabolised in the liver to 25-hydroxyvitamin D (25(OH)D) which is the major circulating form of vitamin D. This form of the vitamin is the one measured by clinicians to determine vitamin D levels in patients. However, 25(OH)D is biologically inert and requires additional hydroxylation within the kidney to form the biologically active derivative of vitamin D, 1,25-dihydroxyvitamin D (1,25(OH)2D3). 1,25(OH)2D3 is a lipid-soluble hormone that interacts with its vitamin D receptors (VDRs) in the small intestine. Its action leads to enhanced expression of the epithelial calcium channel, the calcium-binding protein and various other proteins which sustain the transport of calcium from the intestinal lumen into the circulation. 1,25(OH)2D3 also interacts with VDRs on osteoblasts, which stimulate the expression of the receptor activator of nuclear factor κB (NFκB) ligand (RANKL). This results in a cascading effect that facilitates the maturation of osteoclast precursors to osteoclasts which, in turn, mobilise calcium stores from the skeleton to maintain calcium homeostasis.15
The 25(OH)D3-1-α-hydroxylase that converts 25(OH)D to 1,25(OH)2D3 in the kidney is also expressed in activated macrophages and dendritic cells.16,17 However, in contrast to the renal cells, in antigen presenting cells the enzyme is non-responsive to suppression by either parathyroid hormone or 1,25(OH)2D3. Instead, it is inducible in the cells by a number of factors such as interferon γ (IFNγ) and is downregulated as the dendritic cell matures.18
Vitamin D deficiency is typically found in countries where there is no (or hardly any) ultraviolet light during the winter months and people must rely on the diet as their main source of the vitamin.19 The optimal level for 25(OH)D for bone health begins at 75 nmol/l (30 ng/ml), with the best concentrations at 90–100 nmol/l (36–40 ng/ml),20–22 but the vitamin D level required to maintain optimal immune system homeostasis has not yet been established.
VITAMIN D AND THE IMMUNE SYSTEM
Vitamin D interacts with the immune system. It takes part in the regulation and differentiation of the cells of the immune system directly and indirectly. Early reports linking vitamin D metabolism to the prevalence of autoimmune diseases were largely anecdotal and circumstantial. For instance, associations were detected between the relatively high prevalence of multiple sclerosis and inflammatory bowel disease in northern regions and the lower exposure to sunlight in these geographical locations.23,24 Current data link vitamin D deficiency to many autoimmune diseases including type 1 diabetes mellitus, multiple sclerosis, inflammatory bowel disease, SLE and rheumatoid arthritis.25–27
LYMPHOCYTE CELLS
Vitamin D has direct effects on T and B cells and shapes their responses to activation. Quiescent CD4 T cells express VDRs, but only at low concentrations, which increases fivefold after activation.28
The effect of 1,25(OH)2D3 on the acquired antigen-specific immune response is inhibition of T lymphocyte proliferation,29,30 particularly of the Th1 arm.31 The addition of 1,25(OH)2D3 to CD4 T cells inhibits Th1 cell proliferation and cytokine production.32 The addition of 1,25(OH)2D3 leads to decreased secretion of interleukin (IL)-2 and IFNγ by CD4 T cells and promotes IL-5 and IL-10 production, which further tilts the T cell response towards Th2 dominance.33
The role of 1,25(OH)2D3 in the regulation of IL-4 is controversial. IL-4 is a Th2-associated cytokine whose production has been shown to be upregulated in vivo by 1,25(OH)2D3 treatment. However, other observations have shown inhibition of both Th1 and Th2 cell cytokine production, including inhibition of IL-4.34,35 Addition of 1α,25(OH)2D3 was also shown to inhibit the expression of the IL-6 protein, an important factor that stimulates Th17 cells. Th17 cells are a critical component of the autoimmune reaction.36,37
In B cells, vitamin D has been shown to inhibit antibody secretion and autoantibody production.38
ANTIGEN PRESENTING CELLS
Dendritic cells
Dendritic cells play a central role in regulating immune activation and responses to self. Dendritic cell maturation is central to the outcome of antigen presentation to T cells. In contrast to the antiproliferative effects of 1,25(OH)2D3 on some cell types,39 generation of dendritic cells from bone marrow is not impaired by 1,25(OH)2D3, although an attenuated progression of maturation occurs.40
In vitro, 1,25(OH)2D3 inhibits the differentiation of monocytes into dendritic cells and impedes the stimulatory activity that T cells exert on them.40–42 It has been shown that 1,25(OH)2D3 is one of the most powerful blockers of dendritic cell differentiation and of IL-12 secretion. In vitro, 1,25(OH)2D3 stimulates phagocytosis and killing of bacteria by macrophages but suppresses the antigen-presenting capacity of these cells and of dendritic cells.43 Inhibition of IL-12 is achieved through the direct interaction of 1,25(OH)2D3 bound to the VDR (and NFκB), which interferes with the NFκB-induced transcription of IL-12.44
Other observations suggest that 1,25(OH)2D3 has additional immunosuppressive effects on dendritic cells. In vitro, dendritic cells treated with VDR agonists retain the monocyte marker CD14, fail to upregulate CD1a, retain the ability to carry out macropinocytosis and never express their full complement of MHC and costimulatory molecules (such as CD40, CD80, CD86). The outcome is a decrease in IL-12 and IFNγ while IL-10 and transforming growth factor β production is enhanced, resulting in inhibition of T cell activation.45–48
Macrophages
Vitamin D has been found to promote the induction of monocytic differentiation to macrophages and to modulate macrophage responses, preventing them from releasing inflammatory cytokines and chemokines.49 Vitamin D deficiency impairs macrophage ability to mature, to produce macrophage-specific surface antigens, to produce the lysosomal enzyme acid phosphatase, and to secrete hydrogen peroxide which is essential to their antimicrobial function.50 The addition of 1,25(OH)2D3 increased the expression of macrophage-specific surface antigens and the lysosomal enzyme acid phosphatase while stimulating their “oxidative burst” function.51–53
Prostaglandin E2, a suppressive cytokine, is stimulated by 1,25(OH)2D3 while granulocyte-macrophage colony stimulating factor (GM-CSF) is suppressed. Suppression of GM-CSF is achieved via binding of ligand-bound monomers of the VDR to a DNA element in the promotor region of the gene encoding GM-CSF.54 Moreover, 1,25(OH)2D3 can decrease the antigen-presenting activity of macrophages to lymphocytes by reducing the expression of MHC II molecules on the cell surface.23,30,55
Some immune cells, in particular activated macrophages and dendritic cells, contain the enzyme 1α-hydroxylase which is necessary for the final activating step of the conversion of vitamin D3 to the metabolically active molecule. These cells therefore hold the capacity to synthesise and secrete 1,25(OH)2D3. The 1α-hydroxylase present in immune cells is identical to the renal enzyme, but regulation of its expression and activity is different. Whereas the renal enzyme is principally under the control of calcaemic and bone signals, the macrophage enzyme is primarily regulated by immune signals such as IFNγ.56
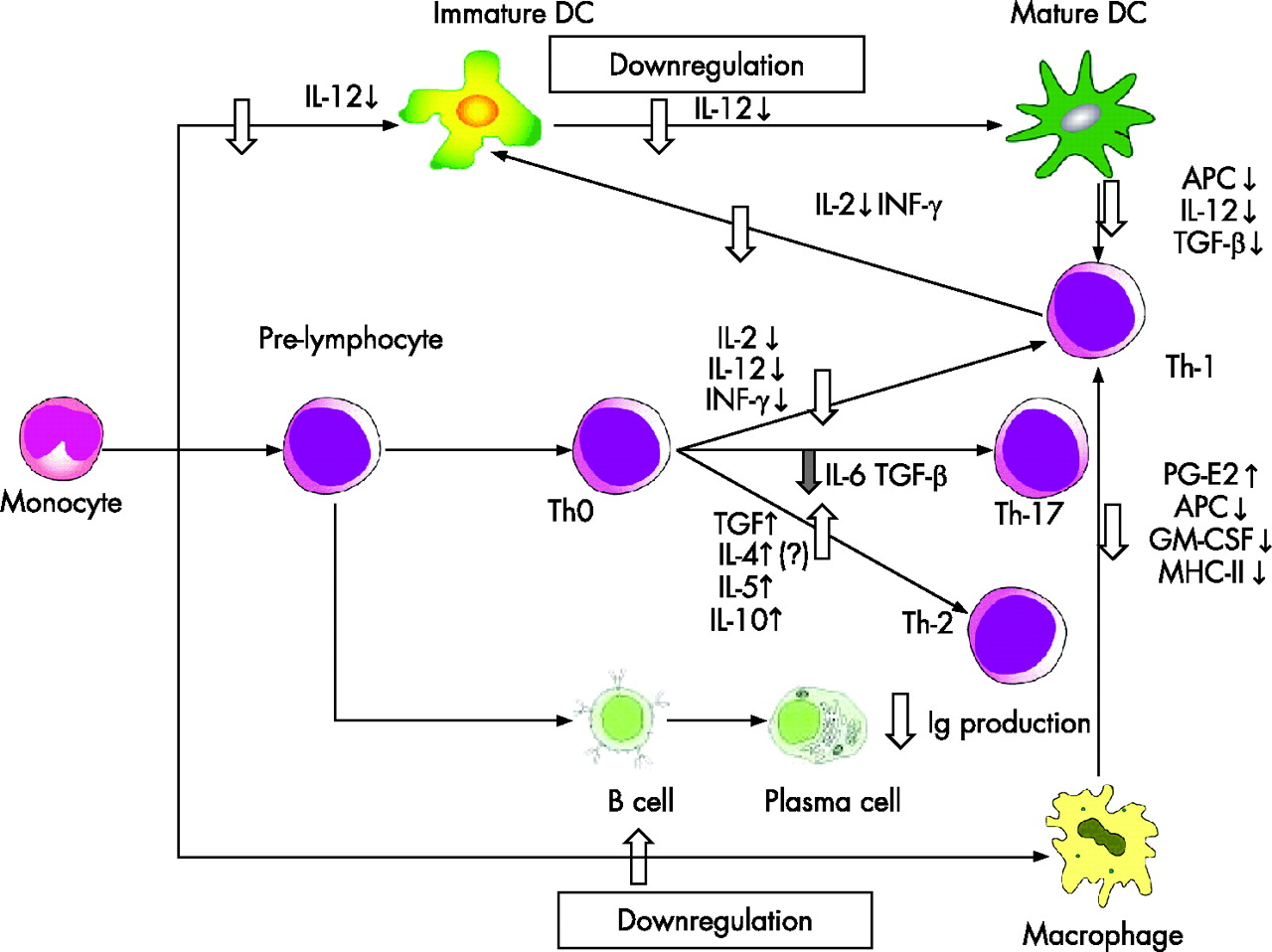
The immunomodulatory effects of vitamin D derivatives in the various arms of the immune system are shown in fig 1.

{kind=link}
Immunomodulatory effects of vitamin D derivatives in the various immune arms: inflammatory dendritic cells (DC), T cells, B cells, plasma cells, macrophages, antigen presenting cells (APC). IL, interleukin; PG, prostaglandin; Ig, immunoglobulin; GM-CSF, granulocyte-macrophage colony stimulating factor; MHC, major histo-compatibility complex; IFNγ, interferon γ; TGFβ, transforming growth factor β.
EVIDENCE FOR ROLE OF VITAMIN D RECEPTORS IN AUTOIMMUNITY
After activation by the active vitamin D metabolite, the VDR, a member of the steroid/thyroid/retinoid receptor gene superfamily of transcription factors, regulates the expression of genes in a variety of vitamin D responsive tissues. This receptor plays a role in the regulation of calcium homeostasis and also exerts immunomodulatory effects.
VDRs are present in a number of cells of the immune system. They can be detected in over 30 different tissues including circulating monocytes, dendritic cells and activated T cells,39 and are found in significant levels in the T lymphocyte and macrophage populations. However, the highest concentration is in immature immune cells within the thymus and in mature CD8 T lymphocytes, regardless of activation status.57 Experiments with VDR knockout mice have concluded that VDRs are needed to enable 1,25(OH)2D3 to induce the differentiation of bone marrow progenitors into monocytes/macrophages, but monocyte/macrophage differentiation can occur in the absence of VDR. Expression of VDR was shown to be important for the generation of a Th1-type immune response by spleen cells.58
Allelic variations within the VDR gene have been implicated in mediating susceptibility to endocrine autoimmune dis-ease.59–61 The genetic differences in the VDR might be one of the many genes that predispose individuals to autoimmunity. Unfortunately, no functional phenotype is associated with specific VDR polymorphisms.62
Several studies have reported an association between type 1 diabetes mellitus and one of four single nucleotide polymorphisms. However, a large meta-analysis combining data from 19 reports found little evidence for a possible genetic association.63,64
Vitamin D is not the only factor affected by exposure to sunlight that has the capacity to modify immune function. Recent studies have shown that melatonin can also act on non-specific, humoral and cellular immune responses.65,66
VITAMIN D DEFICIENCY AND AUTOIMMUNE DISEASES
Inflammatory bowel disease
Inflammatory bowel disease has been found to be more prevalent in areas with decreased sunlight exposure. The disease is more frequent in northern climates such as North America and Northern Europe.67–69 Serum levels of 25(OH)D have been found to be low in patients with inflammatory bowel disease.70
It is unclear why vitamin D deficiency occurs more frequently in inflammatory bowel disease, but it may be due to the combined effects of, for example, low vitamin D intake, malabsorption of many nutrients including vitamin D and decreased outdoor activities with decreased sunlight exposure.
Newly diagnosed patients have lower 25(OH)D levels than controls.71 Experimental inflammatory bowel disease has also been shown to be accelerated by vitamin D deficiency and suppressed by 1,25(OH)2D3 treatment.27,72
In animal studies, IL-10 knockout mice develop a spontaneous inflammatory bowel disease-like condition. IL-10 knockout mice developed diarrhoea and cachexia rapidly and had high mortality rates when they were made deficient in vitamin D. Feeding vitamin D to IL-10 knockout mice prevented these findings and significantly improved their symptoms.73 Experimental treatment with a low calcaemic vitamin D analogue has been shown to display a prophylactic as well as therapeutic profile in Th1-like experimental colitis in mice.74
Multiple sclerosis
The prevalence of multiple sclerosis shows a striking geographical variance. It rises in parallel with increasing latitude in both hemispheres, from a low of 1–2 cases per 105 people near the equator to a high of >200 cases per 105 people at latitudes higher than 50°.75,76 A study set up to investigate bone metabolism in patients with multiple sclerosis revealed a prevalence of low serum levels of 25(OH)D (<50 nmol/l) in 77% of patients.77
Several recent studies have underlined the important role of vitamin D not only in decreasing the rate of relapses in patients with multiple sclerosis but also in preventing the occurrence of the disease. Munger et al9 studied circulating vitamin D levels of more than 7 million active-duty US military personnel taken from 1985 and compared the incidence of multiple sclerosis. The results showed that, among white subjects, the risk of multiple sclerosis significantly decreased with increasing levels of 25(OH)D. In contrast, among black and Hispanic populations, who had lower 25(OH)D levels, no significant associations were found between vitamin D levels and the risk of multiple sclerosis. The authors conclude that supplementation of vitamin D in a high-risk population is safe and beneficial. Although levels of >25 nmol/l have been considered normal and almost everyone in the study had measurements above that level, the optimal serum 25(OH)D concentration should be 90–100 nmol/l.
Another study checked the vitamin D intake in more than 187 000 women from two separate cohorts: the Nurses’ Health Study (92 253 women followed from 1980 to 2000) and the Nurses’ Health Study II (95 310 women followed from 1991 to 2001) and found a 40% reduction in the risk of multiple sclerosis among women who used supplemental vitamin D, primarily in the form of multivitamins, compared with women who did not use these supplements.78 Another intervention study in patients with multiple sclerosis showed that daily supplementation with calcium 16 mg/kg, magnesium 10 mg/kg and vitamin D 125 mg/day for 1–2 years decreased the relapse rate compared with the expected exacerbations.79
In animal experiments, evidence that vitamin D may be a natural inhibitor of multiple sclerosis comes from research done on the experimental autoimmune encephalitis mouse model which serves as a model for multiple sclerosis. Immunisation of mice with spinal cord homogenates containing myelin basic protein or with pure myelin basic protein induces a progressive paralytic autoimmune disease that resembles multiple sclerosis. When vitamin D was given shortly before induction of experimental autoimmune encephalitis, the disease was prevented. Vitamin D also had a therapeutic effect in mice with experimental autoimmune encephalitis and reversed their disease signs.80
Systemic lupus erythematosus (SLE)
In the USA, African-Americans have a threefold increased incidence of SLE which develops at an earlier age with increased morbidity and mortality than in Caucasians.81 This significantly higher prevalence of SLE in the black population cannot be attributed merely to genetics, since the disease is not common among black people who live in West Africa. The difference can therefore probably be attributed to the reduced exposure to sunlight and to the deceased penetration of ultraviolet through pigmented skin resulting in low serum concentrations of vitamin D in the black population living in Western countries. This hypothesis has been reinforced in other studies; Kamen et al27 observed significantly lower serum 25(OH)D levels in patients recently diagnosed with SLE than in controls and a high overall prevalence of vitamin D deficiency. Similar results were also obtained in patients with SLE who had a longer disease course.82–84 However, Huisman et al83 failed to repeat these results. In a cross-sectional study of 25(OH)D, 1,25(OH)2D3 and parathyroid levels in 25 Caucasian patients with SLE and 25 women with fibromyalgia, no significant differences were noted between the two groups. Half of the patients were found to be deficient in vitamin D.
VDR gene BsmI polymorphisms have been used as genetic markers to determine their association with SLE. A Japanese study of 58 patients with SLE found that the BB genotype might trigger the development of SLE and that the bb genotype was associated with lupus nephritis.65 A Taiwanese study of 47 patients with SLE also found an increased distribution of the VDR BB genotype in SLE, but indicated no association between the frequency of VDR allelic variations and clinical manifestations or laboratory profiles.85,86
There are no published studies of the use of vitamin D for treating SLE. Abe et al87 reported that supplementation with vitamin D3 to the MRL/lpr spontaneous developing lupus mouse model significantly improved longevity and reduced proteinuria.
Diabetes mellitus type I
Several epidemiological studies have reported that dietary vitamin D supplementation during infancy and childhood may reduce the risk of developing type 1 diabetes. An important paper in this regard examines the risk ratio for developing type 1 diabetes mellitus with respect to vitamin D supplements in infancy in Finland. A 30 year follow-up study found a marked reduction in the prevalence of type 1 diabetes (relative risk 0.12) in infants who received daily vitamin D supplementation (50 mg/day) in the 1960s. On the other hand, children suspected of having rickets during the first year of life had a threefold increased prevalence of type 1 diabetes compared with normal infants.88,89 Fronczak et al90 reported that the presence of islet autoantibodies in offspring was inversely correlated with maternal dietary vitamin D intake during pregnancy.
Similar to other autoimmune models, 1,25(OH)2D3 successfully prevented autoimmune insulinitis and diabetes in the non-obese diabetic mouse model.5,91
Rheumatoid arthritis
Low 1,25(OH)2D3 levels have been shown to be associated with higher rheumatoid arthritis disease activity in cross-sectional studies. Epidemiological data indicate that >60% of patients with rheumatoid arthritis have 25(OH)D levels <50 nmol/l,92 and 16% have levels in the range of vitamin D deficiency (<12.5 nmol/l). However, the finding of a positive correlation between 1,25(OH)2D3 and alkaline phosphatase indicates that this may partly reflect the fact that people with higher disease activity have increased bone resorption.93
Intervention trials with a dosage of 1 μg 1α-vitamin D were not associated with an improved outcome.94 However, administration of higher amounts of 1α-vitamin D or other forms of vitamin D was associated with decreased pain sensation and a significant reduction in C-reactive protein levels.95
VITAMIN D AND HYPERSENSITIVITY
Owing to the immunomodulatory effect of vitamin D, which suppresses Th1 cell activity, several studies have examined whether vitamin D supplementation in newborn infants is associated with increased rates of atopic reactions commonly encountered in western countries.96 In a cohort of 8285 children aged 3 years, Milner et al97 found a 1.6-fold increased risk for food allergy by multivitamin drops while, in 12 058 live births, Hyppönen et al98 showed a similar 1.7-fold risk of atopy in babies given daily supplements of vitamin D. In animal experiments, asthma-induced VDR knockout mice failed to develop airway inflammation, eosinophilia or airway hyper-responsiveness despite high IgE concentrations and raised Th2 cytokine levels.99
CONCLUSIONS
The common denominator that rises from these studies is that vitamin D affects the immune system at many levels and by a number of mechanisms. It takes part in the genetic regulation of cytokine production, VDR expression and affects important biological processes by which these cells interact. On the whole, vitamin D confers an immunosuppressive effect. Vitamin D has been shown to provide clinically beneficial effects in animal models, and initial observations indicate that vitamin D supplementation may be preventive in multiple sclerosis and diabetes mellitus. These preliminary results are encouraging and further clinical trials are needed to evaluate the potential role of vitamin D in clinical practice.
REFERENCES
Footnotes
-
Published Online First 8 June 2007
-
Competing interests: None.