Article Text

Abstract
Background: Enthesitis is a remarkable feature of ankylosing spondylitis (AS) not specifically approached by the available measuring tools for the disease. Ultrasonography (US) has proved to be an excellent technique for the assessment of tendon pathology.
Objective: To test a Sonographic Entheseal Index (SEI) of the lower limbs in a cohort of patients with AS, as a potential measuring tool.
Methods: 44 patients with AS and 10 healthy controls were enrolled. Bath Ankylosing Spondylitis Functional Index and Bath Ankylosing Spondylitis Disease Activity Index, pain at entheseal points, severity of symptoms, acute-phase reactants, Schober’s test and stage of sacroiliitis were recorded. Patients underwent US examination of five entheseal regions from both lower limbs by two experts. Hypoechogenicity, increased tendon thickness, peritendinous oedema and bursitis were considered signs of active inflammation. Insertional bone erosions, intratendinous calcifications, decreased thickness and tears were considered signs of chronic injury. Each alteration independently scored one point. Data were analysed with Spearman’s correlation method.
Results: A significant interobserver correlation in SEI scores (p<0.001) and a fine discriminative power between controls and patients were observed. Acute entheseal lesions predominated (63% vs 37%), the most frequent alteration being tendon hypoechogenicity (43%). 72% of all lesions were located at the foot. The SEI correlated with reduction of Schober’s test (p<0.02), but not with other activity or severity parameters.
Conclusions: A scoring method such as the SEI may be of help in characterising entheseal injury in AS, and for decision making in these patients.
- AS, ankylosing spondylitis
- BASDAI, Bath Ankylosing Spondylitis Disease Activity Index
- BASFI, Bath Ankylosing Spondylitis Functional Index
- CRP, C reactive protein
- ESR, erythrocyte sedimentation rate
- MEI, Mander’s Entheseal Index
- SEI, Sonographic Entheseal Index
- SEI-A, Sonographic Entheseal Index for acute lesion
- SEI-C, Sonographic Entheseal Index for chronic lesion
- US, ultrasonography
Statistics from Altmetric.com
- AS, ankylosing spondylitis
- BASDAI, Bath Ankylosing Spondylitis Disease Activity Index
- BASFI, Bath Ankylosing Spondylitis Functional Index
- CRP, C reactive protein
- ESR, erythrocyte sedimentation rate
- MEI, Mander’s Entheseal Index
- SEI, Sonographic Entheseal Index
- SEI-A, Sonographic Entheseal Index for acute lesion
- SEI-C, Sonographic Entheseal Index for chronic lesion
- US, ultrasonography
Enthesitis, or the inflammation of ligament, tendon and joint capsule insertions, is a prominent feature of ankylosing spondylitis (AS).1 Although no single abnormality can be considered as a unique hallmark of AS, enthesitis has been proposed as the primary lesion of AS,2 and fibrocartilage, a major component of entheses, as a candidate target tissue.3–5 However, it seems that this feature usually remains underestimated in clinical practice. In this sense, definite criteria for the diagnosis of enthesopathy are lacking and, so far, there are no validated tools to accurately measure entheseal injury in AS. Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) and Bath Ankylosing Spondylitis Functional Index (BASFI) are instruments that were developed to overcome the poor sensitivity of biological markers, such as erythrocyte sedimentation rate (ESR) and C reactive protein (CRP).6–8 But these questionnaires fail to specifically address enthesitis, since only one of six items in BASDAI and none in BASFI refers to this feature. With regard to physical examination, the Bath Ankylosing Spondylitis Metrology Index includes five clinical measurements; however, its utility is limited to spinal involvement.9
Two methods have been designed to evaluate enthesopathy in AS: Mander’s Entheseal Index (MEI) and the Maastricht Ankylosing Spondylitis Entheseal Score.10,11 MEI is based on the intensity of pain produced by local pressure on 66 entheseal points, and it scores severity of pain in a 0–3-point scale. Maastricht Ankylosing Spondylitis Entheseal Score has been recently developed with the intention of simplifying MEI. This instrument reduces the number of entheseal points to 13, and omits graduation of pain. Both are manual systems, therefore limited as objective measuring tools.
There is general agreement that an image-based procedure is necessary to evaluate entheseal pathology, and x rays and MRI are frequently used for this purpose. However, none of these methods seems adequate for screening, because of radiation exposure or cost. Additionally, x rays only detect indirect evidence of severe or/and longstanding entheseal injury. In turn, MRI has advantages such as a high soft-tissue contrast resolution, a multiple-plane view and a great capability of delineating sites of inflammation.12 The value of this technique to detect bone marrow oedema adjacent to the altered entheses has also been underlined.13 Nonetheless, it has recently been suggested that ultrasonography (US) might be superior to MRI in detecting early signs of enthesopathy.14–16 US is an inexpensive, non-invasive and non-radiating technique, widely available and easy to manage for experienced rheumatologists.17,18 Although this technique can be considered subjective in performance and in evaluation, it certainly eliminates the bias from manual pain-triggering methods, and there is an increasing interest in its use for assessment of entheseal pathology.19–22 In this regard, Balint et al20 elaborated a 36-point US-based scoring, examining five entheseal areas of the lower limbs of patients with AS. They found no correlation between the US punctuation and acute-phase reactants.
These previous works suggest that the development of a standardised scoring system for the evaluation of enthesitis in AS would be of high interest to improve our measuring tools of disease activity and process, and to evaluate response to treatment. With that aim, we present results obtained in this work in a cohort of patients with AS with a US scoring system of enthesopathy at the lower extremities, comparing it with activity and functional indexes.
METHODS
Patients
In all, 44 patients with AS from our unit, Department of Rheumatology, Fundación Jiménez Díaz, UAM Madrid, Spain, were recruited for a transversal study. All of them fulfilled the AS modified New York criteria.23 Patients with other inflammatory rheumatic disease, active known neoplasia, history of recent trauma, exhaustive physical activity, recent surgery or age <18 years were excluded. Ten healthy volunteers of similar age were included as a control group. Relatives of patients with AS or people meeting one or more of the above-mentioned exclusion criteria were not allowed as controls. All patients and controls gave informed consent to participate in the study, and approval was obtained from the institutional ethics committee. Before the evaluations, participants underwent a washout period of their non-steroidal anti-inflammatory treatment intended to allow the disease to flare.
Clinical examination
Disease activity was assessed with BASDAI and BASFI questionnaires, back pain and morning stiffness in 10 cm visual analogue scales, and ESR and CRP as serum markers. Disease severity was measured by Schober’s test, grade of radiological sacroiliitis and BASFI. A clinical evaluation of enthesopathy was carried out using MEI.
Ultrasound examination
US examinations were performed by two experts (JCA, OS-P) who were blinded with regard to the disease status of the subjects. The equipment was a 7.5 MHz linear array transducer (Toshiba Capasee, Tokyo, Japan). All patients underwent two consecutive US examinations performed by each examiner. Table 1 shows the entheseal areas evaluated and the scoring system.
Description of target areas and alterations evaluated in the sonographic scoring of entheses
Patients were laid in a supine position with knees flexed to 60° to explore the quadriceps tendon insertion, the superior patellar tendon insertion, and the inferior patellar tendon insertion at the anterior tibial tuberosity. The insertion of Achilles tendon and the plantar aponeurosis insertions at the calcaneous were evaluated with patients placed in a pronosupination with ankles at neutral flexion. All areas were scanned bilaterally. As table 1 also shows, the examiners established a series of relevant alterations for the development of a Sonographic Enthesitis Index (SEI), based on previous reports.24–28 These were in turn classified into signs of acute inflammation, which included increase of thickness, hypoechogenicity, peritendinous oedema and bursitis, and chronic lesions, which were tears, loss of thickness, intratendinous calcification and bone erosion. Figure 1 shows representative US images of these features obtained in our study. US pathological findings were considered as categorical variables and each scored one point. It was agreed that any unclear image not matching these criteria should be scored as normal, aiming to increase the stringency of the method. The maximal SEI punctuation was 76 points, of which 36 points referred to acute lesions and 40 points to chronic lesions, the difference resulting from the absence of bursa in 2 anatomical areas.

Representative sonographic findings scored in the study; projection, entheseal region and findings are described. (A) Sagittal view; distal infrapatellar tendon insertion; increased thickness of the tendon and bursitis (left side) and the image of the contralateral site, considered normal (right side). (B) Sagittal view; proximal insertion of the infrapatellar tendon; thickening of the tendon (left side) in comparison to the contralateral site, considered normal (right side). (C) Sagittal view, plantar fascia insertion; thickening and hypoechogenicity (left), and the image of the contralateral site, considered normal (right). (D) sagittal view, Achilles tendon insertion, hypoechogenicity of the tendon associated with deep bursitis, peritendinous oedema and erosions at the insertion zone of the calcaneous (CALC). (E) Sagittal view, proximal patellar tendon insertion, entheseal calcification or syndesmophyte formation.
Statistical analysis
Descriptive results were expressed as mean (SEM). The interobserver reliability of US scores was analysed by α test and intraclass correlation coefficient with 95% CI. Sonographic scores and disease measures were compared with Spearman’s correlation method. All the calculations were performed with SPSS V.8.0.
RESULTS
Demographic and clinical characteristics of the patients
In all, 35 of the 44 patients with AS were men (ratio 3.8:1). Mean age was 43 (range 24–72) years and average age at diagnosis was 31 (range 11–65) years, with a mean duration of disease of 17 (range 0–47) years.
Back pain was 5.2 (0.3) cm, and morning stiffness 4.5 (0.5) cm; BASFI punctuation was 3.2 (0.4) cm and BASDAI 3.9 (0.4) cm (all measured using visual analogue scales). Clinical evaluation of entheseal areas showed an MEI of 7 points (range 0–42). The value of Schober’s test was 1.9 (0.2) cm, and that of radiological sacroiliitis was 2.7 (0.2). Regarding serological markers of disease activity, ESR was 22 (3) mm and CRP 9 (2) mg/l.
Sonographic findings at the entheses
Following the study protocol described in the Methods section, the two evaluators examined the selected targets of all patients and controls, and the total punctuation for each case was summed to obtain an SEI. All healthy controls had an SEI of 0 points. Only 3 of 44 patients with AS had a normal study, according to the evaluation of both examiners. The interobserver reliability was good, as reflected by an intraclass correlation coefficient of 0.72 (95% CI 0.56 to 0.83; α = 0.84). The SEI from rater 1 (JCA) was used for further studies, this decision being based on individual expertise.
The mean (SEM) global SEI of the AS group was 5.4 (0.6) points. Separately considered, the US scoring of active lesions (SEI-A) was 3.5 (0.4) points and the punctuation for chronic injury (SEI-C) was 1.9 (0.3). There were 109/440 (25%) abnormal entheseal sites on US examination. A total of 150 of 239 (63%) lesions were classified as acute and 89 (37%) were chronic. The most frequent abnormalities were tendon hypoechogenicity and increase in thickness at the attachment region, which accounted for 43% and 38% of the acute lesions, respectively. On the other hand, bone erosion and entheseal calcification were the most common chronic lesions observed (55% and 43% of total, respectively). Achilles tendon and plantar fascia had a higher number of lesions (40% and 32% of total, respectively; fig 2).

Distribution and frequencies of the entheseal alterations detected by ultrasound (US). Total acute lesions and total chronic lesions are represented in black bars, and each of the categories in grey; data are expressed in percentages with regard to all pathological lesions observed.
Comparison between clinical and sonographic evaluation of entheses
Compared with the 25% abnormal entheseal areas found by US, only 8% (n = 35) painful areas were found using MEI. Because of their different design, these measures were only comparable at the entheseal targets of the foot. In these areas, 50% of the 176 entheseal sites evaluated by US had one or more abnormalities, whereas only 12% (n = 14) were painful (fig 3). The lesions at these sites found by US were silent, regardless of being acute or chronic. On the other hand, 90% of the entheses without sonographic lesions were also asymptomatic. In turn, sonographic lesions found in sensitive entheses were acute in 40% of cases, another 40% showing simultaneous acute and chronic lesions, whereas the remaining 20% were chronic.

Comparison between entheseal tender points assessed by Mander’s Entheseal Index (MEI) and signs of entheseal injury by ultrasound (US) at the preselected foot targets. The number of altered (+) or silent (−) cases in Achilles insertion (blue) and plantar fascia (red) is shown. Double positive cases are shown at the right upper panel (squared pattern).
Correlation of SEI with disease activity and severity measures
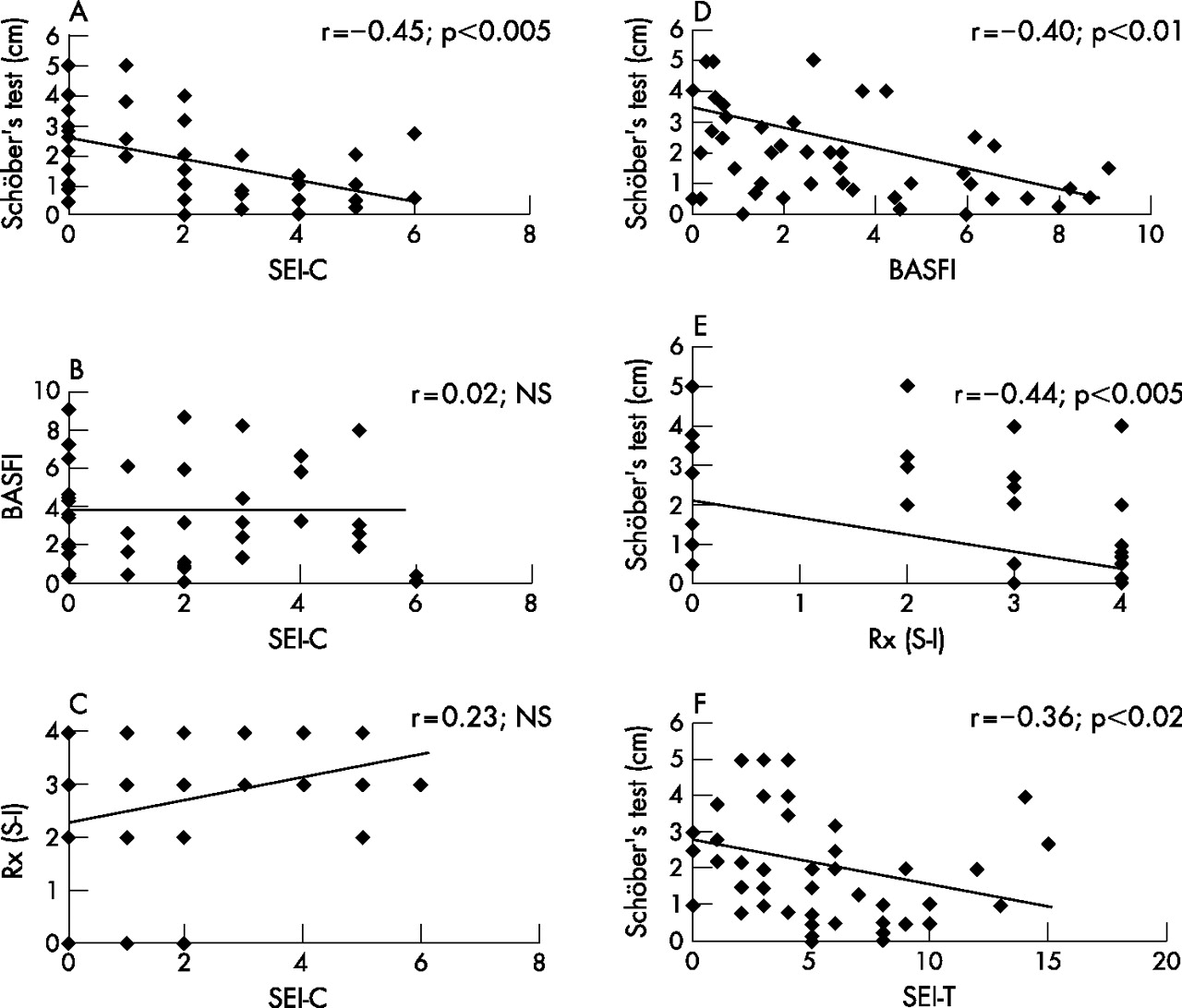
To seek for a correlation between measuring tools for AS and the SEI, we considered the scoring of SEI-A and SEI-C individually, and compared SEI-A with activity measures and SEI-C with severity markers. We did not find a significant correlation between any activity parameters of AS and their SEI-A. By categorising SEI-A into tertiles, we observed a tendency of most parameters to worsen in parallel with increasing categories (data not shown), even though this trend was not found for the serological activity markers PCR and ESR. In turn, the SEI-C showed an inverse correlation with Schober’s test (r = –0.45; p<0.005) but was not correlated with BASFI and radiological sacroiliitis, despite both these measures being inversely correlated with Schober’s test (r = –0.39; p<0.01 and r = –0.44; p<0.005, respectively; fig 4). The global SEI also showed a significant correlation with Schober’s test reduction (r = –0.36; p<0.02; fig 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison between severity of ankylosing spondylitis parameters and the Sonographic Entheseal Index. Correlations were performed with Spearman’s non-parametric method. The tendency and the correlation coefficient are shown, as well as the p value for each comparison. BASFI: Bath Ankylosing Spondylitis Functional Index; Rx (S-I), radiographic sacroiliitis score; SEI-C, Sonographic Enthesitic Index for chronic lesions; SEI-T, Sonographic Enthesitis Index of total (acute plus chronic) lesions.
DISCUSSION
It has been suggested that enthesitis could be the primary lesion accounting for the development of all musculoskeletal features of spondyloarthropathies.2,3 For this reason, an increasing number of experts support inclusion of enthesitis in the classification criteria for AS and related syndromes.4 To assess the actual involvement of enthesitis in the pathogenesis of AS, as well as its contribution to disease activity, progression or affect on quality of life in the disease, a systematic examination of entheseal areas with a sensitive tool would be ideal. Furthermore, with new treatments able to control activity and progression of spondyloarthropathies becoming available, the evaluation of entheseal injury could help to select candidates and to measure response to treatment.29 In this regard, several reports have found improvement of enthesitis after treatment with tumour necrosis factor α blockers.30–32
It is thought that microtrauma on fibrocartilage structures is at the origin of enthesitis in spondyloarthropathies.4,29,33 In this regard, the evaluation of target areas at anatomical locations prone to trauma injuries, such as the foot and the knee, could be enough to reflect “total” enthesitis.34 In our study, up to 25% of total entheses examined in this AS cohort showed abnormalities, and only 3 of 44 patients had a normal study. The results confirm both the common involvement of the selected sites, as already reported, and the high prevalence of entheseal alterations in AS.19,20,22
As a whole, our findings were comparable to previous reports, although in contrast with the study from Balint et al,20 we found scant alterations at the inferior patellar tendon insertion. At this entheseal area, several anatomical factors, such as tendon widening and the sharp changing of fibre orientation, account for characteristic anisotropic artefacts that may be misleading. Thus, perhaps this entheseal area should be avoided in a relatively subjective scoring system such as SEI. On the other hand, the plantar fascia and the Achilles tendon were the entheseal sites found more frequently altered in our study and in previous studies.19–22
With regard to manual methods of entheseal evaluation, we did not expect to find a correlation between MEI and the SEI, since the target areas evaluated in each case were not coincidental. However, considering the entheseal targets of the foot, we found a remarkable dissociation between sensitivity to local pressure and US findings. There was a striking number of asymptomatic lesions, even between those classified as acute inflammatory signs. On the other hand, we also found normal US images in symptomatic entheses. In this sense, it has been suggested that structures in proximity, such as bone marrow, rather than the enthesis itself could account for the pain.29 In fact, studies conducted with MRI have shown that bone marrow oedema precedes the appearance of inflammation at soft tissues.13 In turn, enthesitis could be more linked to symptoms such as swelling, discomfort, gelling or stiffness.
Enthesitis in AS consists of local, destructive microscopic inflammatory lesions, which evolve towards fibrous scarring and new bone formation. Perhaps the major novelty introduced by the SEI in this study is that it distinguishes between acute injury and chronic lesions, a differentiation that, at least in the case of rheumatoid arthritis, has therapeutic implications. Nonetheless, our data showed only a vague relationship between the SEI and disease measuring tools. Although this could possibly be overcome by the recruitment of a larger sample, the absence of correlation between measures has also been found by other authors. The poor ability of systemic parameters, such as ESR and CRP, to assess disease activity in AS has also been recognised.35–37 On the whole, this reminds us that several independent markers have to be measured to accurately assess AS, ideally one of them specifically targeting entheseal involvement.
In conclusion, we have developed an SEI that is easy to perform by rheumatologists experienced in US, which may help to characterise entheseal injury better in AS patients. Our results suggest that an SEI could be of interest for decision making in these patients. We highlight the convenience of including an evaluation of the calcaneal insertions, and also a classification of lesions into acute (potentially reversible) and chronic (possibly inactive) lesions. With new US devices of higher resolution becoming available, a more sensitive SEI could be developed.
REFERENCES
Footnotes
-
Published Online First 6 December 2006
-
Competing interests: None declared.