Article Text

Abstract
Objective: Chronic inflammatory diseases such as systemic lupus erythematosus (SLE) and rheumatoid arthritis are associated with accelerated atherosclerosis. We hypothesised that atherosclerosis may also be increased in Takayasu arteritis.
Methods: The frequency of atherosclerotic plaques and the intima–media thickness (IMT) were investigated in 30 female patients with Takayasu arteritis (mean age (standard deviation), 35.4 (8.0) years), along with 45 sex-matched and age-matched patients with SLE (37.4 (6.8)) and 50 healthy controls (38.2 (5.7)). Plaques were scanned and IMT was measured at both sides of the common carotids, carotid bulb, and internal and external carotid arteries by B-mode ultrasonography. Traditional risk factors for atherosclerosis were also assessed.
Results: Most of the atherosclerotic risk factors were comparable between patients with Takayasu arteritis and SLE. More atherosclerotic plaques were observed among patients with Takayasu arteritis (8/30; 27%) and those with SLE (8/45; 18%) than among the healthy controls (1/50; 2%; p = 0.005). Logistic regression analyses showed that the presence of a plaque was associated only with age in both Takayasu arteritis and SLE (p = 0.04 and 0.02, respectively). The mean overall IMT was significantly higher among patients with Takayasu arteritis (0.95±0.31 mm) than among the patients with SLE (0.58±0.10 mm) and the healthy controls (0.59±0.08 mm; p<0.001).
Conclusion: Patients with Takayasu arteritis have a high rate of atherosclerotic plaques, at least as frequent as that observed among patients with SLE.
- BMI, body mass index
- CCA, common carotid artery
- ESR, erythrocyte sedimentation rate
- HDL, high-density lipoprotein
- hsCRP, high-sensitivity C reactive protein
- ICA, internal carotid artery
- IMT, intima–media thickness
- LDL, low-density lipoprotein
- SLE, systemic lupus erythematosus
- USG, ultrasonography
Statistics from Altmetric.com
- BMI, body mass index
- CCA, common carotid artery
- ESR, erythrocyte sedimentation rate
- HDL, high-density lipoprotein
- hsCRP, high-sensitivity C reactive protein
- ICA, internal carotid artery
- IMT, intima–media thickness
- LDL, low-density lipoprotein
- SLE, systemic lupus erythematosus
- USG, ultrasonography
Takayasu arteritis is a chronic, idiopathic, inflammatory disease that principally affects the aorta and its primary branches. Arteritis can produce stenosis, occlusions and aneurysms of large vessels.1–3 Women are affected more than men.
Strong and growing evidence shows that diseases associated with chronic inflammation lead to premature atherosclerosis.4–6 Both overt and subclinical atherosclerosis have been described in patients with systemic lupus erythematosus (SLE) and rheumatoid arthritis.7,8,9,10,11,12,13,14
There have been sporadic reports, using imaging technology including B-mode ultrasonography (USG),15–19 in which some features of premature atherosclerosis, along with characteristic arterial wall changes of the disease itself, are described in Takayasu arteritis. Furthermore, there are autopsy reports of atherosclerotic changes in young patients with the same disease.20–24
The carotid arteries can easily be visualised by B-mode USG. This method allows the detection of atherosclerotic plaques and measurement of intima–media thickness (IMT), both considered to be markers of generalised atherosclerosis.25–28
We investigated the frequency of atherosclerotic plaques and measured carotid artery IMT by using B-mode USG among patients with Takayasu arteritis, along with patients with SLE and healthy controls of similar age and sex in a formal protocol.
PATIENTS AND METHODS
Consecutive female outpatients with Takayasu arteritis and SLE, aged 18–50 years, who were routinely followed up in the Division of Rheumatology, Cerrahpasa Medical Faculty, Istanbul, between June 2004 and March 2005 were studied. Patients with both Takayasu arteritis and SLE participated in the study regardless of a history of myocardial infarction, stroke or a transient ischaemic attack. However, patients with renal insufficiency (serum concentration of creatinine ⩾1.4 mg/dl) were excluded. In all, 50 women hospital workers aged 18–50 years were used as healthy controls. None of them had hypertension, diabetes mellitus, chronic renal failure, myocardial infarction, stroke or a transient cerebral ischaemic attack.
Clinical evaluation
The study population was evaluated within a week of the ultrasonographic scans. Patients and controls were given a standard questionnaire on traditional atherosclerotic risk factors. These included smoking history, familial history of premature cardiovascular disease, menstrual status, diabetes mellitus, hypertension and prior history of myocardial infarction. A physical examination was carried out, and height and weight were measured. Blood was drawn for laboratory analyses. Clinical characteristics and information on the use of immunosuppressants and corticosteroids were obtained from the charts.
Assessment of traditional cardiovascular risk factors
Previous or current use was considered to be positive smoking history. Having a first-degree relative with myocardial infarction, stroke or sudden death before the age of 55 years for men or before the age of 65 years for women was considered to be positive family history of cardiovascular disease. Diabetes mellitus was defined as a fasting blood glucose concentration ⩾126 mg/dl or being a current user of oral hypoglycaemic agents or insulin. Hypertension was defined as having a systolic blood pressure ⩾140 mm Hg or a diastolic blood pressure ⩾90 mm Hg, or using antihypertensive drugs. Blood pressure of patients and controls was measured after a 5-min rest during physical examination. Among patients with Takayasu arteritis, arterial blood pressure could be measured on the right arm in eight patients, on the left arm in three and on the lower extremities in two; it could not be measured at all on either extremity in two patients. In the remaining 15 patients with Takayasu arteritis and all other study participants, the measurements were made on both upper arms. Only the highest level measured was taken into consideration. The body mass index (BMI) was calculated as weight divided by the square of height (weight (kg)/(height (m))2).
Blood samples were collected after overnight fasting. Biochemical parameters (serum glucose, creatinine, triglycerides, total and high-density lipoprotein (HDL) cholesterol) were measured with an Olympus AU 800 autoanalyser (Olympus, Tokyo, Japan). The methods used were hexokinase for glucose, Jaffe for creatinine, cholesterol oxidase-p-aminophenazone for total cholesterol and glycerol phosphate oxidase-p-aminophenazone for triglycerides. HDL levels were determined by immunoinhibition. The Friedewald equation was used to estimate low-density lipoprotein (LDL) cholesterol.29 Erythrocyte sedimentation rate (ESR) was measured using an Eriline-Ar 60 automated analyser (Linear Chemicals, Barcelona, Spain). Serum high-sensitivity C reactive protein (hsCRP) concentrations were determined by immunonephelometry, using a BN II Systems Analyser (Dade Behring, Malburg, Germany).
Assessment of carotid artery atherosclerosis
B-mode carotid artery USG was carried out as described.9 A scanner (Ultramark 9 HDI, Advanced Technology Laboratories, Bothell, Washington, DC, USA) equipped with a 10-MHz linear array imaging probe was used. The right and left common carotid arteries (CCA), carotid bulb and the proximal 1.5 cm of the internal carotid (ICA) and external carotid arteries were scanned for atherosclerotic plaques. An atherosclerotic plaque was defined as a distinct area protruding into the vessel lumen. This protrusion had to be at least 50% thicker than the surrounding areas. The plaque severity was graded on the basis of the percentage of stenosis—that is, <30%, 30–50% and >50% of the lumen.
IMT was measured across a 1-cm segment of both the right and left sides of the near and far walls of the distal CCA, the far wall of the carotid bulb and the ICA. When plaques were present, measurements were made from their outside borders. The mean of all measurements from eight locations was taken as an overall measure of IMT. Diffuse and homogeneously increased (⩾1-mm) long IMT segments, which could be differentiated from plaque formation, were identified as possibly associated with Takayasu arteritis.
The radiologist (RC) was blinded to the clinical diagnoses. Intraobserver variability in ultrasound was assessed by a repeated evaluation of 28 randomly selected participants after 1–2 months. Intraobserver agreement was excellent (κ = 1.0) for plaque identification. The mean variability for IMT calculated as described30 by the absolute mean (SD) difference of the two consecutive measurements was 0.14 (0.20) mm.
All participants gave informed consent and the local ethics committee of the Cerrahpasa Medical School approved the study.
Statistical analysis
Comparisons of continuous variables between groups were made by one-way analysis of variance using the Bonferroni correction. The categorical variables were compared by the χ2 test or the Fisher exact test. Comparisons between participants with and without atherosclerotic plaques were made by the Student t test for continuous variables and by the χ2 test or the Fisher exact test for categorical variables. The variables that were associated with plaque presence were later analysed by multiple stepwise logistic regression tests. All tests were carried out using SPSS V.10.0 software for Windows. Continuous data were given as the mean (SD), unless otherwise stated.
RESULTS
A total of 30 female patients fulfilling the American College of Rheumatology 1990 criteria for the diagnosis of Takayasu arteritis31 were studied. The diagnosis was also based on invasive angiography in each case and was carried out at their initial registration into the outpatient clinic. The median time that elapsed between the invasive angiography and the current study was 2.3 years (interquartile range 7 months–10 years). Table 1 gives the disease localisations based on invasive angiography. The major sites associated with Takayasu arteritis were the subclavian artery (n = 24; 80%), common carotid artery (n = 21; 70%) and aorta (n = 18; 60%). Two (7%) patients had myocardial infarction due to coronary ostial stenosis. Of 30 patients with Takayasu arteritis, 18 (60%) were active, according to the National Institute of Health criteria,3 and the remaining 12 (40%) were in remission at the time of the study. All those who had active disease were receiving treatment for Takayasu arteritis, except 4 who had been diagnosed recently. Of 12 who were in remission, 5 were off treatment and 7 were still on treatment. Among 21 (70%) patients who were currently being treated, 11 were using a combination of corticosteroids and azathioprine, 8 were using a combination of corticosteroids and methotrexate, and 2 were on corticosteroids alone.
Angiographic findings in 30 patients with Takayasu arteritis
Among the 45 patients with SLE fulfilling the revised American College of Rheumatology classification criteria,32 renal association was present in 21 (47%) and cerebrovascular disease in 5 (11%). Only one patient, whose coronary angiography had a documented myocardial infarction, was normal. In all, 18 (40%) of the patients reported no symptoms attributable to their disease at the time of the study.
Table 2 gives the demographic, clinical and the cardiovascular characteristics of the patients with Takayasu arteritis, those with SLE and controls. The mean age, disease duration, BMI, diastolic blood pressure, frequency of hypertension, diabetes mellitus and smoking, and the mean levels of ESR and hsCRP, duration of corticosteroid treatment and azathioprine were not different between patients with Takayasu arteritis and those with SLE. The frequency of corticosteroid use along with its duration and cumulative dose were significantly lower among patients with Takayasu arteritis compared with that among the patients with SLE (table 2). The controls, by definition, did not have hypertension or diabetes mellitus. The mean age, BMI, the frequency of being postmenopausal, the levels of serum creatinine, fasting blood glucose, and total HDL and LDL cholesterol did not differ between the study groups. Patients with Takayasu arteritis were more likely to have a positive family history of cardiovascular disease than patients with SLE and were less likely to smoke compared with controls. Also, patients with Takayasu arteritis had higher systolic blood pressure than patients with SLE.
Clinical characteristics and the cardiovascular risk factors of the patients and controls
Atherosclerotic plaques
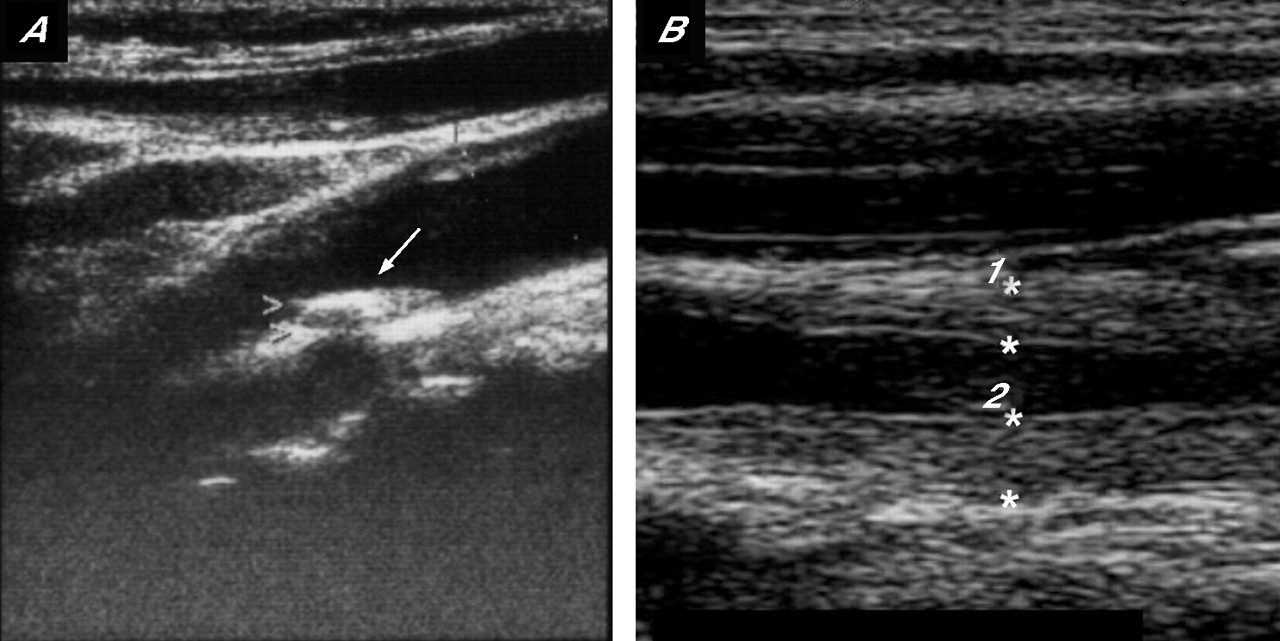
At least one carotid artery plaque was present in 8 of the 30 (27%) patients with Takayasu arteritis, 8 of the 45 (18%) patients with SLE and in 1 of the 50 (2%) controls (p = 0.005). Among the 8 patients with Takayasu arteritis, 10 atherosclerotic plaques were detected in CCA (n = 4), carotid bulb (n = 5) and ICA (n = 1; fig 1A). In all, 9 of 10 plaques caused <30% stenosis of the lumen and the remaining one between 30% and 50%. A total of 11 plaques were seen in 8 patients with SLE, which were localised in CCA (n = 2), carotid bulb (n = 4) and ICA (n = 5). Similarly, 9 of 11 plaques in patients with SLE caused <30% stenosis of the lumen and the remaining 2 between 30% and 50%. Among the controls, one patient had only one atherosclerotic plaque in the carotid bulb, which was of a lower grade.
{kind=link}
(A) Ultrasonographic longitudinal scan of a calcified plaque on the carotid bulb in a 47-year-old patient with Takayasu arteritis. The diffuse arterial wall thickening is visible on the near wall of the scan. (B) Ultrasonographic longitudinal scan of the left common carotid artery in a 32-year-old patient with Takayasu arteritis. The diffuse and homogeneously increased intima–media thickness can be seen in both near and far walls.
Comparisons of patients with and without atherosclerotic plaques
Patients with Takayasu arteritis with atherosclerotic plaques were considerably older and had higher levels of total cholesterol than those who had no plaques (table 3). Although the frequency of postmenopausal patients, the levels of LDL and triglycerides, the systolic and diastolic blood pressures, the disease duration, the duration and the cumulative dose of corticosteroids were higher among patients with Takayasu arteritis with plaques than those without, none of these were significant. Patients with SLE with plaques were also considerably older and more postmenopausal than their counterparts without plaques. Again, although the disease duration and the duration of corticosteroid use were somewhat higher among those patients with SLE with plaques than those without, this was not significant (data not shown). Multiple logistic regression analyses were also used to determine the atherosclerotic risk factors that were associated with plaques. Only age remained significant in this analysis among the patients with Takayasu arteritis (for a 1-year increase in age, odds ratio (OR) = 1.22; 95% confidence interval (CI) 1.01 to 1.46; p = 0.04). The same association with age and having a plaque was also true for SLE (for a 1-year increase in age, OR = 1.20; 95% CI 1.03 to 1.40; p = 0.02).
Variables associated with atherosclerotic plaque formation among patients with Takayasu arteritis*
Intima–media thickness
In one patient with Takayasu arteritis, the right CCA, carotid bulb and ICA could not be visualised, because of the complete occlusion of these vessels. The measurements in this patient were made from non-occluded segments. The mean IMT of carotid arteries among the patients with Takayasu arteritis (0.95 (0.31) mm) was significantly increased compared with that of the patients with SLE (0.58 (0.10) mm) and the controls (0.59 (0.08) mm; p<0.001). It did not markedly differ between SLE and controls.
Among 30 patients with Takayasu arteritis, by B-mode USG, 23 had diffuse and homogeneous intima–media thickening >1 mm, which we had defined as suggestive for involvement with Takayasu arteritis (fig 1B), whereas none of the patients with SLE or controls had such involvement. Among these 23 patients, 19 (83%) were already known to have carotid artery involvement by angiography, whereas 4 had no such involvement. The mean carotid IMT (SD) was significantly thinner among patients without carotid involvement (0.59 (0.05) mm; n = 7) compared with that among patients with carotid disease (1.06 (0.27) mm; n = 23; p = 0.003), but similar to that among those patients with SLE and controls. It was also noteworthy that among 8 patients with carotid plaques, there were 10 plaques, 9 of which had diffuse and homogenous intima–media thickening. On the other hand, no plaques were seen among those seven patients who had no carotid disease.
DISCUSSION
In this case–control, cross-sectional study, we chose to restrict our observations to women, as the number of male patients with Takayasu arteritis and SLE was very small, because of the inherent sex allocation in these diseases. This, coupled with the potential confounder effect of men being usually more prone to atherosclerosis, made us study only female patients. To reduce the frequency of “naturally occurring” atherosclerosis in our study population, we restricted our upper age limit to 50 years (47 for Takayasu arteritis).
We observed that 27% of our patients with Takayasu arteritis and 18% of patients with SLE had atherosclerotic plaques in carotid arteries, whereas this was 2% among the age-matched and sex-matched controls. On the other hand, IMT was increased only among the patients with Takayasu arteritis. Recent case–control studies on SLE likewise found no increase in thickness of carotid arteries despite a high frequency of plaques.11,14 The mean carotid artery IMT (range) of patients with Takayasu arteritis (0.95 (0.4–2.7 mm) was markedly greater than that of SLE and controls and was also, as expected, higher among those with carotid artery involvement than among those without. Our finding of an increased IMT only among patients with Takayasu arteritis is therefore more suggestive that it is the nature of disease, the unique association of the vessel wall in Takayasu arteritis, that has primarily been behind the increase in IMT. The range of IMT measurements and qualitative observations among the patients with Takayasu arteritis conform with other reports15–19,33 and the intraobserver variability we worked with in our study (0.14 (0.20) mm) was well within the range of what has been described in two previous reports (0.02–0.66 mm).30,34
The inflammatory changes in Takayasu arteritis affect the adventitia and the media, whereas in atherosclerosis, intimal changes are more pronounced.20,21 As it is not possible to distinguish between intima and media with ultrasound,25,26 our contention that the increased IMT is due to the vasculitis itself is mainly based on indirect evidence. Further studies on Takayasu arteritis, also looking at vessels less commonly associated with atherosclerosis, have the potential for a more direct approach. It will also be helpful to use electron beam computed tomography to search for atherosclerosis.35
Although the utility of B-mode carotid USG is not good enough to differentiate between an increased IMT due to Takayasu arteritis itself or the associated atherosclerosis, it is better when we look for plaques.36 A heterogeneous increase in density covering shorter areas with an irregular appearance is rather specific for atherosclerotic plaques (fig 1A).15,19,33,36 The perfect intraobserver variability in detecting these plaques is also a reflection of the high specificity of the B-mode USG for plaque detection. Finally, studies report that the atherosclerotic plaques are more reliable than an increased IMT for the presence of atherosclerosis.27,28,37,38
An intriguing possibility also exists that it is mainly in areas where primary vessel wall disease is more prominent in Takayasu arteritis that secondary atherosclerosis is more common. When we classified the patients with Takayasu arteritis into those with and without carotid involvement on the basis of USG findings, we observed that plaques were present only among patients with Takayasu arteritis with carotid involvement (n = 23). Furthermore, 9 of 10 plaques were present on the side of the carotid involvement that we attributed to primary vessel wall disease. Recent studies back up this contention.39,40 The arterial stiffness in Takayasu arteritis was found to be more prominent in carotid arteries and aorta, areas predominantly affected by the disease, rather than the peripheral femoral arteries, which are not typically affected by the disease. Thus, local and systemic persistent inflammation from the disease itself, arterial injury due to the functional abnormalities or turbulent blood flow and shear stress in stenotic segments, all may play a part in the pathogenesis of the atherosclerosis observed in Takayasu arteritis. This is presumably different from the atherosclerosis seen in SLE, where chronic systemic inflammation is thought to play the primary part. The rate of coronary heart disease among patients with SLE is extremely high and is a major cause of mortality,7,8 whereas coronary artery involvement in Takayasu arteritis, which is usually proximal and osteal (hence due to vasculitis), has been reported to be relatively low.41
Patients with Takayasu arteritis were more likely to have a positive family history of cardiovascular disease, were less likely to smoke, and had higher levels of systolic blood pressure than those with SLE and controls. Patients with obstructive vessel disease diagnosed at an early age can be more aware of the presence of vascular disease in their relatives and for the same reason they could smoke less. As expected, patients with SLE had used corticosteroids more than patients with Takayasu arteritis. Apart from these, patients with Takayasu arteritis were comparable to patients with SLE with respect to traditional atherosclerotic risk factors, disease duration, and levels of ESR and hsCRP. Healthy people, by definition, were those lacking the major atherosclerotic risk factors.
In univariate analyses, older age and high cholesterol level were markedly associated with plaques in case of Takayasu arteritis, whereas the same was true for older age and being postmenopausal in case of SLE. However, only age remained significant for the presence of plaques, in multivariate logistic regression analyses in both diseases. Furthermore, in the univariate analyses (table 3), disease duration, duration and dose of corticosteroids, and some classic atherosclerotic risk factors (being postmenopausal, having high blood pressure, high LDL and triglyceride levels) had a tendency to be higher in patients with Takayasu arteritis with plaques than in those without. Several reports on SLE and rheumatoid arthritis show likewise that older age, being postmenopausal and high cholesterol are associated with atherosclerosis.7,9–14 Moreover, in some of these studies, disease duration and corticosteroid use were also found to be associated with atherosclerosis. The lack of a marked association between the presence of plaques and disease duration, traditional risk factors and corticosteroid use in our study may be due to the small number of patients in each subgroup.
The arterial blood pressure measurements among patients with Takayasu arteritis would expectedly be low when measured distal to the areas of diseased vessels. About 80% of our patients have subclavian artery involvement and the remaining 20% have abdominal aorta involvement. Central aortic pressure could not be analysed in our study. Still, arterial blood pressure measurements among patients with Takayasu arteritis were found to be higher than those of others.
Owing to a case–control, cross-sectional design, our study had the obvious limitation of perhaps not including those patients at either end of the clinical severity spectrum, those who had died and those who chose not to attend our clinic because of mild disease. On the other hand, it is not unreasonable to think that this recruitment bias would affect the SLE group in a similar manner. Also, the robustness of the comparisons made between patients with Takayasu arteritis with and without plaques needs to be reconfirmed, because we could compare only a limited number of patients.
Increased atherosclerosis in patients with Takayasu arteritis may be multifactorial. It may be associated with local and systemic disease activity, as well as with traditional atherosclerotic risk factors such as hypertension and hyperlipidaemia, as observed in this study. These risk factors may well develop secondary to Takayasu arteritis or may develop as the side effects of the treatment itself. We think that the effective control of traditional atherosclerotic risk factors is needed, in addition to the effective suppression of disease activity, for the management of Takayasu arteritis.
CONCLUSIONS
The frequency of atherosclerotic plaques was similar among the patients with Takayasu arteritis when compared with that observed in SLE, a disease widely appreciated to be associated with systemic premature atherosclerosis. Whether this increase goes with (a) an augmented and sustained acute-phase response in Takayasu arteritis; (b) with the unique vessel wall involvement in this condition; (c) with the traditional atherosclerotic risk factors; or (d) with all or any combination of the above needs to be clarified.
REFERENCES
Footnotes
-
Published Online First 26 January 2006
-
Competing interests: None.