Article Text

Abstract
OBJECTIVE To demonstrate the use of high resolution ultrasound measurements and power Doppler mode in the diagnosis and follow up of a patient with psoriatic arthritic with retrocalcaneal bursitis and Achilles tendonitis.
METHODS An outpatient based ATL HDI 3000 ultrasound equipment was used with a CL10–5 MHZ 26 mm probe and musculoskeletal software. Real time B mode and power Doppler mode were used to detect changes in structure and blood flow.
RESULTS Unilateral retrocalcaneal bursitis and Achilles tendonitis were demonstrated by sonography. Power Doppler mode was useful to demonstrate an increased blood flow around an abnormal retrocalcaneal bursa. A follow up examination showed marginal thickening of the Achilles tendon without any bursitis.
CONCLUSIONS Ultrasonography is an objective method in the confirmation of clinical diagnosis after physical examination. During the examination it is possible to gain not only qualitative but also quantitative data. A comparative study with quantitative data is possible in longitudinal studies.
Statistics from Altmetric.com
Over the past five years a number of editorials have been written about the use of ultrasonography in rheumatology practice.1-6 Recently, Grassi and colleagues reported the use of ultrasonography in the evaluation of a patient with psoriatic arthritis.7 We report the use of ultrasonography in following the natural history of Achilles tendonitis in a patient with HLA-B27 negative psoriatic arthritis.
Clinical history
A 35 year old man with a two year history of HLA-B27 negative psoriatic arthritis presented to the rheumatology clinic with increasing right heel pain. He was receiving sulfasalazine 2.5 g and indometacin 75 mg twice daily for his arthritis. Physical examination revealed a swollen and tender right Achilles tendon. In view of his increased disease activity his dose of sulfasalazine was increased from 2.5 to 3.5 g/day.
Methods
ATL HDI 3000 ultrasound equipment with a CL 10–5 MHZ 26 mm probe (linear array, small footprint hockey-stick style transducer) was used to image both Achilles tendons without applying pressure. During the examination the patient was in a prone position with his feet freely hanging over the edge of the examination table in a neutral position. After static examination a dynamic examination was performed with the foot in slight dorsal and plantar flexion. The Achilles tendon thickness was measured on both sides. The power Doppler mode was also used with the following parameters: medium flow optimum, low wall filter, dynamic range 55 dB, pulse repetition frequency 1000 Hz. After one year a follow up examination was performed. Scans were stored in a magnetic optical disk drive.
Results
Real time B mode ultrasonography confirmed a thickening of the Achilles tendon and retrocalcaneal fluid accumulation on the right side. Left Achilles tendon thickness was in the normal range (0.47 cm). The right Achilles tendon thickness was 0.95 cm. The retrocalcaneal bursa diameters were 0.59 cm and 0.42 cm (fig1).

Measurements of the bursa and the Achilles tendon in the sagittal plane on the first occasion. The left Achilles tendon thickness was in the normal range (0.47 cm). The right Achilles tendon thickness was 0.95 cm. The retrocalcaneal bursa diameters were 0.59 cm and 0.42 cm.
Power Doppler sonography showed increased blood flow around the bursa in the longitudinal and transverse section. One year later when symptoms had clinically resolved, repeat ultrasound examination did not detect a power Doppler signal or fluid collection (figs 2 and 3). The right Achilles tendon was, however, still thicker than the left side 0.60 cm and 0.48 cm respectively (fig 4). On the normal left Achilles tendon the difference in thickness between the two examinations was only 0.01 cm, which demonstrates a small intraobserver error.

The middle image shows the sagittal scanning position of the distal part of the Achilles tendon. The left image shows the patient's first sagittal sonogram. The right image shows the control sonogram in the same position. PR = proximal; D = distal; S = skin surface; A = Achilles tendon; C = calcaneus; F = fluid in the retrocalcaneal bursa. The green frame signifies the area of a power Doppler scan and the red colour may indicate increased blood flow.

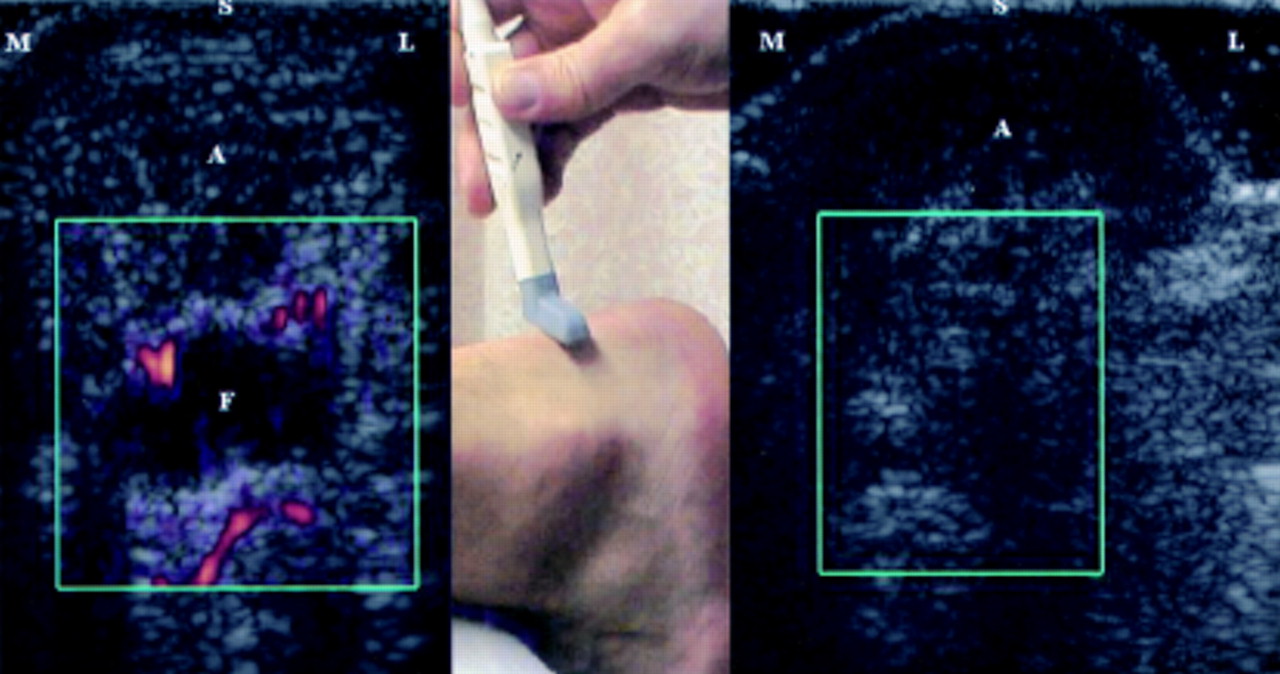
The middle image shows the transverse scanning position of the distal part of the Achilles tendon. The left image shows the patient's first transverse sonogram. The right image shows the control sonogram in the same position. M = medial; L = lateral; S = skin surface; A = Achilles tendon; F = fluid in the retrocalcaneal bursa. The green frame signifies the area of a power Doppler scan and the red colour may indicate increased blood flow.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Measurements of the Achilles tendon in the sagittal plane on the second occasion. The left Achilles tendon thickness was again in the normal range (0.48 cm). The right Achilles tendon thickness (shown on the left hand side of the figure) was 0.60 cm. No fluid could be detected on this occasion.
Discussion
Clinical examination will easily detect a swollen Achilles tendon in most cases. However, to distinguish between Achilles tendonitis, paratenonitis, and retrocalcaneal bursitis, ultrasonography is required. The Achilles tendon is a relatively large superficial structure, which is easily imaged by ultrasound. Previously, this technique was described without8 and with a stand-off pad9 and pitfalls have been recognised.10Normal and abnormal retrocalcaneal bursae have also been studied previously.11-13 Ultrasound guided aspiration and corticosteroid injection have been used with excellent results.14 ,15 Cunnane and colleagues treated six of 13 patients with retrocalcaneal bursitis with guided corticosteroid injection and all responded well.15 This group included two patients who had had a number of unsuccessful non-guided injections. Interestingly, in all 13 cases retrocalcaneal bursitis was associated with postero-superior calcaneal erosions. In our case we could not demonstrate any bony changes, probably owing to the short duration of symptoms.
This case illustrates that ultrasonography can detect pathological changes in Achilles tendonitis and can monitor changes over a long period of time. The use of the power Doppler mode may be helpful in detecting increased blood flow due to inflammation, but standardisation of the technique to ensure reproducibility is difficult.