Article Text

Abstract
Objectives To investigate how the first wave of COVID-19 pandemic influenced decisions of rheumatologists and health professionals in rheumatology regarding the management of patients with inflammatory rheumatic and musculoskeletal diseases (RMDs).
Methods An English-language questionnaire was developed by a EULAR working group and distributed via national rheumatology societies of EULAR countries, EMEUNET and individual working group members. Responses were collected using an online survey tool. Descriptive statistics were calculated.
Results We analysed 1286 responses from 35/45 EULAR countries. Due to containment measures, 82% of respondents indicated cancellation/postponement of face-to-face visits of new patients (84% of them offering remote consultation) and 91% of follow-up visits (96% with remote consultation). The majority of respondents (58%) perceived that the interval between symptom onset and first rheumatological consultations was longer during containment restrictions than before. Treatment decisions were frequently postponed (34%), and the majority (74%) of respondents stated that it was less likely to start a biological disease modifying anti-rheumatic drug (DMARD)/targeted synthetic DMARD during the pandemic, mainly because of patients’ fear, limited availability of screening procedures and decreased availability of rheumatological services. Use of (hydroxy)chloroquine (HCQ) and tocilizumab (TCZ) for the COVID-19 indication was reported by 47% and 42% of respondents, respectively, leading to a shortage of these drugs for RMDs indications according to 49% and 14% of respondents, respectively.
Conclusion Measures related to containment of COVID-19 pandemic led to a perceived delay between symptom onset and a first rheumatological visit, postponement of treatment decisions, and shortage of HCQ and TCZ, thereby negatively impacting early treatment and treat-to-target strategies.
- epidemiology
- arthritis
- rheumatoid
- autoimmune diseases
- health services research
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Key messages
What is already known about this subject?
Containment measures have been established in several European countries to prevent exponential growth of the infectious rate with the novel SARS-CoV-2 causing COVID-19.
(Hydroxy)chloroquine (HCQ) or tocilizumab (TCZ) have been used for treatment of some patients with COVID-19.
What does this study add?
This study investigated from a public health perspective to what extent COVID-19 affected decisions of rheumatologists and health professionals in rheumatology concerning the management of patients with inflammatory rheumatic and musculoskeletal diseases (RMDs).
Rheumatology services were partially or completely closed in the majority of EULAR countries leading to cancellation/postponement of face-to-face visits.
The perceived interval between symptom onset and first rheumatological consultations was longer during containment restrictions than before.
Treatment decisions were frequently postponed and it was less likely to start a biological disease modifying anti-rheumatic drug (DMARD)/targeted synthetic DMARD during the pandemic.
Use of HCQ and TCZ for the COVID-19 indication led to a shortage of these drugs for RMDs patients.
Key messages
How might this impact on clinical practice or future developments?
Telemedicine and other care strategies should be researched more intensively in order to maintain high-quality of care even when face-to-face visits are not feasible.
Future off-label use of drugs for COVID-19 indication outside a clinical trial should be discouraged as it might led to shortage of the respective substance for patients with RMDs.
Prioritising strategies for face-to-face visits and investigations should be developed in order not to delay diagnosis and treatment and to guarantee adequate monitoring of disease activity and safety of patients with inflammatory RMDs also during future waves of COVID-19 or other pandemics caused by highly contagious infectious agents.
Introduction
The novel SARS-CoV-2 and COVID-19 is a highly contagious disease that has reached Europe at the beginning of 2020 and has been causing high morbidity and mortality.1–3 Containment measures have been established in most European countries in order to prevent exponential growth of the infection.3 To what extent these measures influenced early diagnosis and treatment of patients with inflammatory rheumatic and musculoskeletal diseases (RMDs) is unknown.
While the majority of patients with COVID-19 has a favourable outcome, some of them develop severe pneumonia eventually leading to respiratory failure along with other organ manifestations and sepsis.1 COVID-19 appears to have at least two distinct disease phases: a phase characterised by the immune response against the virus aiming at eliminating the pathogen, and in some patients, a subsequent phase of severe ‘cytokine release syndrome’ instead of the expected phase of convalescence.4 Some of the most severe complications of COVID-19 seem indeed to be caused by an exaggerated response of the immune system. Immunomodulatory agents commonly prescribed in rheumatology such as (hydroxy)chloroquine (HCQ) or tocilizumab (TCZ) have been used for treatment of patients with COVID-19.5–7 Whether the off-label use of these drugs in COVID-19 induces a shortage of supply and whether this has an impact on treatment decisions in patients with RMDs is elusive so far.
Looking at the current situation from a public health perspective, there are several questions that arise: (1) have the ‘treat to target’ and ‘early diagnosis’ paradigms for patients with inflammatory RMDs been still feasible during the COVID-19 crisis?; (2) have patients been less likely to initiate TCZ or other biologicals or have they been switched from TCZ to therapies with other modes of action in order to save drugs for patients with COVID-19?; (3) has a shortage of medication led to patients having to stop HCQ or TCZ?
This EULAR project was designed to clarify how and to what extent COVID-19 affected decisions of rheumatologists and health professionals in rheumatology (HPR) concerning the management of patients with RMDs from a public health perspective. The knowledge gained from this study will help to prepare for future waves of COVID-19 and other pandemics caused by highly contagious infectious agents.
Methods
An English-language questionnaire was developed by a EULAR working group composed of rheumatologists, a methodologist, experts in public health, and an HPR. The questionnaire contained 37 questions organised in three broad sections: (1) professional background, (2) influence of containment measures on the organisation of care for patients with inflammatory RMDs and (3) drugs used both in rheumatology and to treat COVID-19. The majority of questions were in the multiple-choice format recognising the possibility that multiple not mutually exclusive strategies might have been applied (eg, which patient groups have been prioritised during closure for a face-to-face or remote visit). The survey also contained a few single choice (eg, for age and sex) or open-ended questions.
The survey was distributed via EULAR secretariat and EULAR scientific member societies (No.: 45), delegates of the EULAR Standing Committee on Epidemiology and Health Services Research, and EMEUNET using emails, newsletters and social media. The working group members also personally contacted physicians and HPR from different countries, requesting them to answer and disseminate the questionnaire (snow-ball principle). The questionnaire was accompanied by an explanatory letter regarding the purpose of the survey. The answers were collected via an online survey tool (SurveyMonkey) from 13 May till 17 June 2020. At least one reminder was sent by EMEUNET and individual working group members. Online supplemental file 1 provides the full questionnaire and additional details on the execution of the survey. Ethical approval was not required because the study did not involve patients; all responses were anonymous.
Supplemental material
The target audience of the survey were rheumatologists and other physicians or HPR from EULAR countries who have been directly involved in care of patients with inflammatory RMDs, however; the survey was open to all physicians/HPR.
Descriptive and summary statistics were applied to the questionnaire responses. Absolute and relative frequencies were calculated and depicted in tabular and graphical form. Data are presented as number (nominator) and percentage of all available responses to each question (denominator) throughout the manuscript. The denominator may change from question to question for the following reasons: (1) questions and individual answers could have been skipped, (2) some questions could have been answered with ‘not applicable’ or ‘do not know’, which were detracted from the denominator as indicated, (3) specific subgroup analyses were conducted. Since the majority of questions were in the multiple-choice format, the sum of nominators from individual questions may exceed the corresponding denominator.
Results
A total of 1428 responses were collected from 58 countries (see online supplemental table 1 for number of responses from all countries): 1286 (90%) were from 35 out of the 45 EULAR countries, 15 (1%) came from Africa, 10 (0.7%) from Asia, 8 from North-America (0.6%), 7 from South-America (0.5%), 2 (0.1%) from Australia/New Zealand, 1 (0.1%) from Andorra whereas 99 (7%) have not specified the country of practice.
Supplemental material
In this paper, only results for EULAR countries are presented (n=1286). Ten (22%) EULAR countries provided no and 19 (56%) more than 10 responses. Demographic data of respondents are summarised in table 1. The number of responses per question ranged from 663 to 1286. To support the interpretation of results in relation to the country-specific impact of COVID-19, we summarised data on infections with SARS-CoV-2, mortality and containment measures in EULAR countries as per April 2020 in online supplemental table 2.
Supplemental material
Demographics of respondents from EULAR countries (n=1286)
Influence of containment measures on organisation of care for patients with inflammatory RMDs
General organisation of rheumatology care
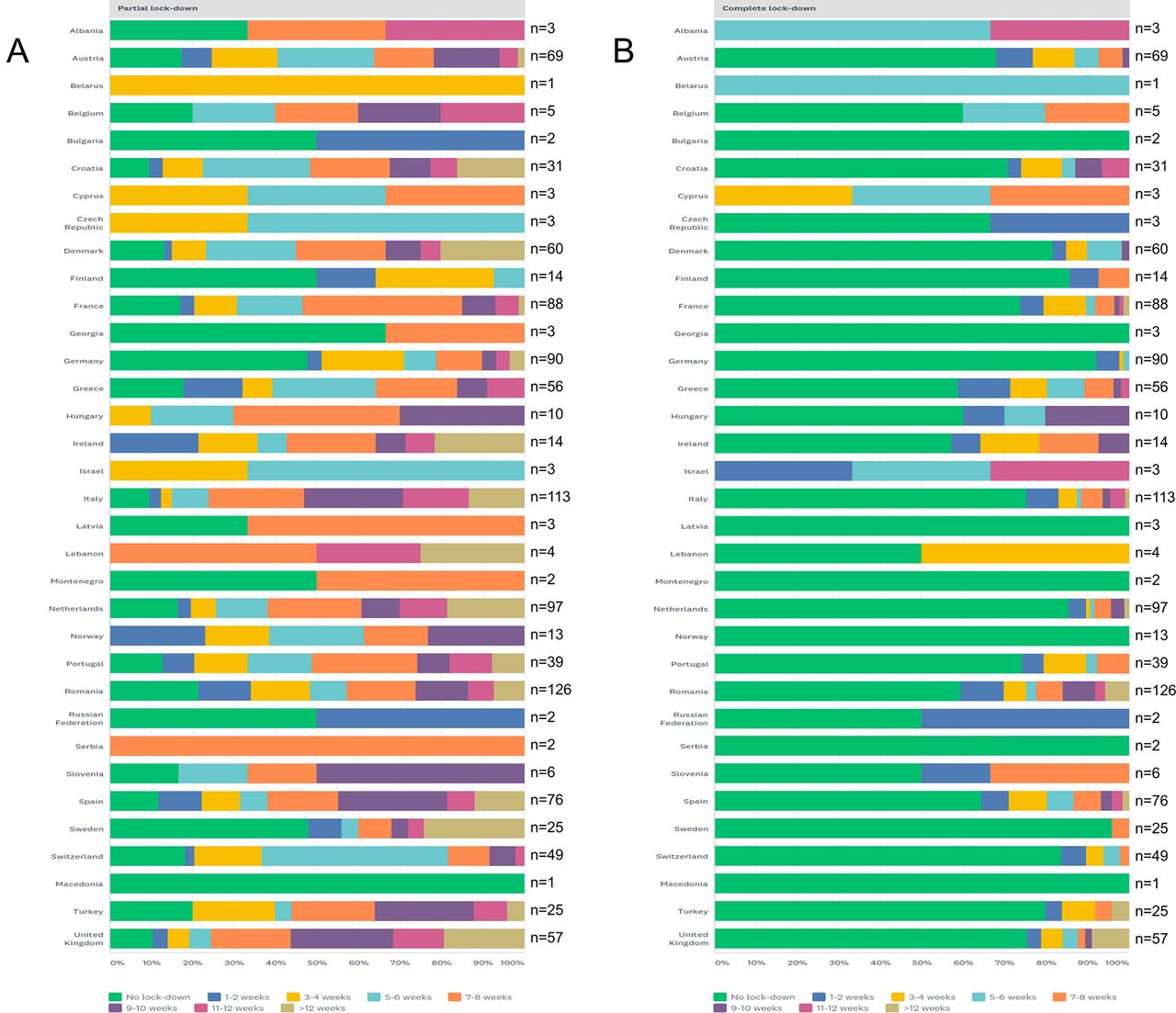
Partial closure of rheumatology services guaranteeing, for example, only emergency visits was reported by 622/1094 (57%, 192 skipped the question) of respondents, 19 (2%) indicated that rheumatology services were suspended completely at least temporarily, 265 (24%) reported both, partial and complete closure and only 188 (17%) indicated no closure. Partial closure typically lasted between 5 and 8 weeks (43% of those who reported partial closure), whereas complete closure was normally not longer than 1–4 weeks (48% of those who reported complete closure). See figure 1 for data on duration of partial and complete closure according to different EULAR countries. A median of 26.4% (±34.1%) of total working time of respondents (ie, workforce) was reallocated to other services such as emergency department, infectious disease clinic, COVID-19 unit or similar.

Partial and complete closure of rheumatology services in EULAR countries. Figures indicate the percentage of respondents indicating the number of weeks with partial (A) or complete (B) closure according to different countries.
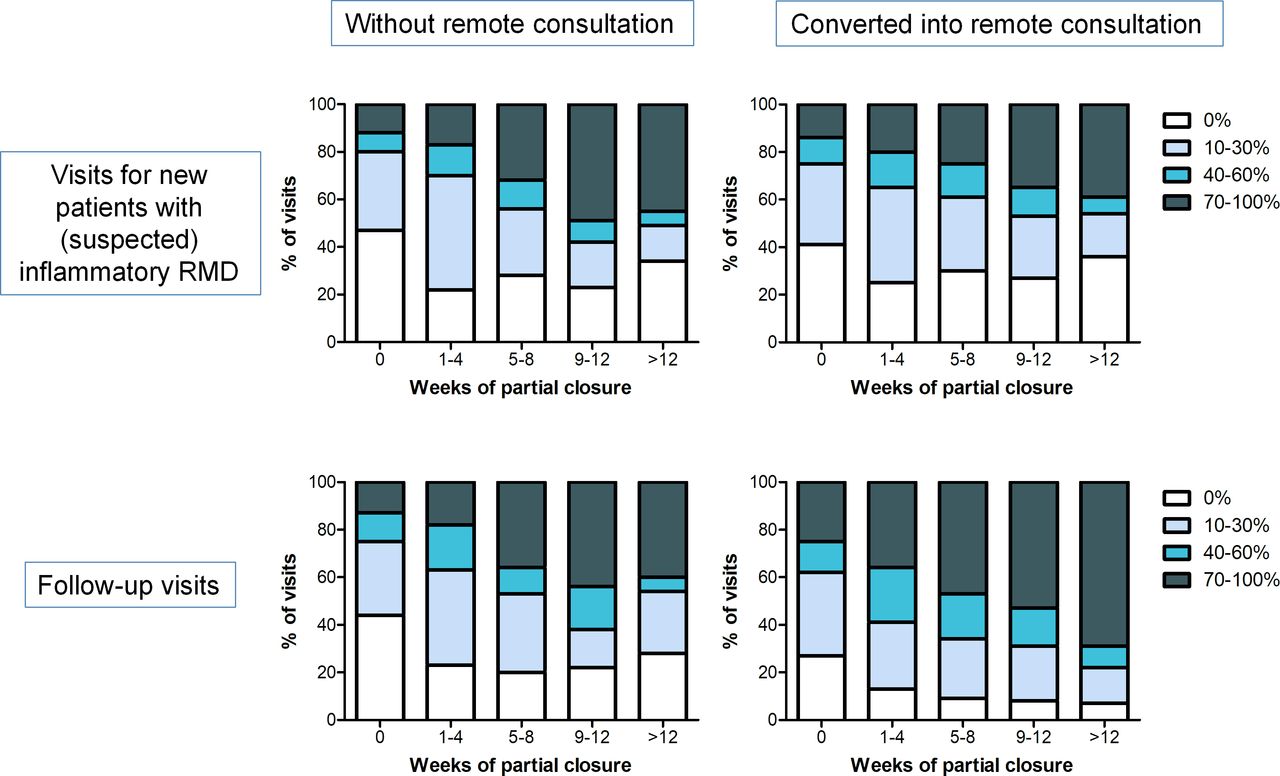
Due to complete and/or partial closure of rheumatology services, 899/1094 (82%) physicians/HPR indicated cancellation or postponement of at least some face-to-face visits of new patients with (suspected) RMDs, 84% of those who had to cancel/postpone visits offered remote consultation at least for some of these visits (see tables 2 and 3 for details). Concerning follow-up visits, 991/1094 (91%) responded to have cancelled/postponed visits with 96% of them offering remote consultation. The frequency of postponement/cancellation of face-to-face visits of new patients and follow-up visits in relation to the duration of partial and complete closure is detailed in figure 2. Accordingly, the percentage of postponed/cancelled visits increased along with the duration of closure.

Postponement/cancellation of face-to-face visits according to the duration of closure of rheumatology services. Figures indicate the cumulative percentage of respondents (Y axis) indicating the proportion of face-to-face visits (4 categories represented by the colours) of new patients and follow-up visits postponed/cancelled with or without remote consultation in relation to the duration of partial and/or complete closure of rheumatology services in weeks.
Cancellation or postponement of face-to-face visits of new patients, according to the extent of closure of the rheumatology services
Cancellation or postponement of follow-up face-to-face visits, according to the extent of closure of the rheumatology services
Remote consultations were conducted by different health workers: 924/1030 (90%) respondents indicated that rheumatologists and/or other specialists performed this activity, 302 (29%) and 223 (23%) stated that specialists in training and HPR, respectively, were (also) involved. Phone (966/1005, 96%) and/or email (n=498, 50%) were among the techniques most commonly used to consult with patients, whereas video (n=241, 24%) or mobile applications (n=44, 4%) were less frequently applied. Respondents stated that patients with suspected inflammatory RMDs (458/1029, 45%), those with previously unstable or active disease (n=563, 55%) or those with ongoing intravenous drug therapy (n=448, 44%) were prioritised for a face-to-face visit. They also indicated that patients receiving biological disease modifying anti-rheumatic drugs (bDMARDs) or targeted synthetic DMARDs (tsDMARDs) (319/1031, 31%) as well as those with unstable disease (n=234, 23%) were prioritised for a remote consultation. No specific prioritisation plan was reported by 277/1029 (27%) for face-to-face visits and by 434/1031 (42%) respondents for remote consultations.
Influence of changed care on principles of early diagnosis and treat to target
The majority of respondents had the impression that the intervals between symptom onset and first rheumatological visits were longer during COVID-19 related closure as compared with the months before (599/1031, 58%, with 26% of those 599 physicians/HPR stating that it was considerably longer).
A minority of respondents (153/1030, 15%) answered that they were contacted more frequently by patients for a suspected flare as compared with before the crisis. Patients with a suspected flare were managed using multiple approaches: most physicians/HPR indicated that a face-to-face visit (723/927, 78% to whom the question was applicable) or a remote consultation (n=553, 60%) were offered. Day-care or in-patient care, referral to the emergency department or consultation with another specialist were rare options (each<10%). The majority of respondents (678/1029, 66%) felt that disease activity of patients with inflammatory RMDs they consulted during closure was not different from that in the preceding period.
Cancellation or postponement of non-urgent tests either by the service provider or by patients themselves were reported by 699/1030 (68%) and 426 (41%) respondents, respectively. Also, 34% of physicians/HPR (299/873 to whom the question was applicable) indicated that treatment decisions were frequently postponed and 62% (n=542) stated that patients’ management was mainly based on history and clinical examination without additional tests.
Drugs used in rheumatology and to treat COVID-19
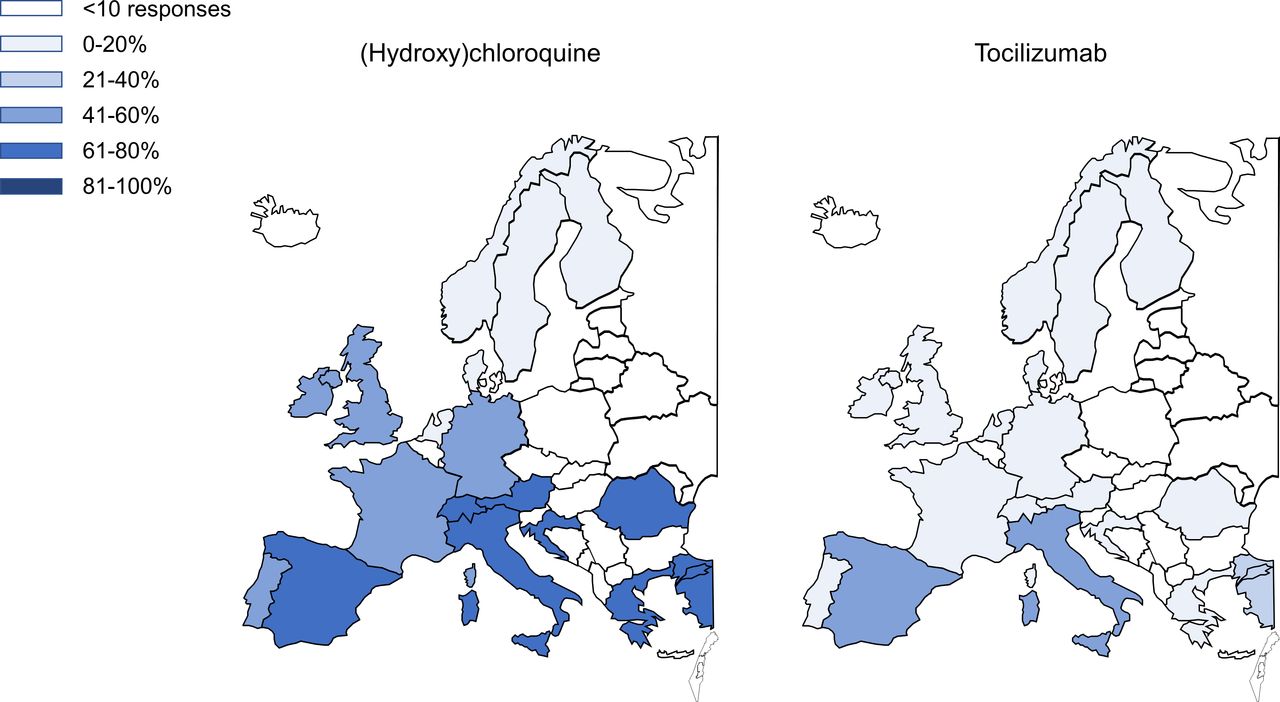
The use of HCQ for COVID-19 indications was reported by 466/1003 (47%) respondents. HCQ was particularly prescribed to patients admitted to the hospital (351 of those 442 who felt knowledgeable to answer this question, 79%) or to the intensive care unit (n=234, 53%), but also to those managed on an outpatient basis (184, 42%). Only a minority of respondents used HCQ for prophylaxis in health workers and/or other individuals (38/1003, 4%) as well as in patients with RMDs (mean 2%±9% of RMDs patients, n=914 responses). A shortage of HCQ was noted by 492/999 (49%) of respondents with large differences between countries (see figure 3). Consequently, this drug had to be stopped in a mean of 10% (±18%) of RMDs patients (n=811 responses). The majority of physicians/HPR (738/996, 74%) stated that they were less likely to start a bDMARD or tsDMARD in RMDs patients during COVID-19 crisis mainly because of patient’s fear to start such a treatment (n=569, 57%), limited availability of screening procedures (n=284, 29%) and/or decreased availability of rheumatological services (n=270, 27%).

{kind=link}
{kind=link}
{kind=link}
Shortage of (hydroxy) chloroquine (HCQ) and tocilizumab (TCZ) in EULAR countries. Figures indicate the percentage of respondents indicating a shortage of HCQ and/or TCZ according to countries. Only data for EULAR countries with >10 responses are shown.
Treatment of patients with COVID-19 with TCZ was reported by 423/1005 (42%) respondents, either in the setting of a clinical trial (178 of those 423 who indicated the use of TCZ in their hospital or practice, 42%) or off-label outside a study (n=245, 58%). TCZ was mainly administered to patients admitted to the intensive care unit (64% of those reporting use of TCZ for COVID-19). A shortage of TCZ was noted by 134/980 (14%) respondents, mainly in Italy and Spain as outlined in figure 3. Overall, shortage or expected shortage of TCZ only rarely influenced the decision to start this drug in rheumatoid arthritis (RA) or giant cell arteritis, or to change treatment in patients with stable disease as depicted in table 4. In Italy and Spain however, preference of another bDMARD/tsDMARD, postponement of treatment with TCZ, as well as change of therapy in stable patients was commonly considered (online supplemental table 3).
Supplemental material
Influence of shortage/expected shortage of tocilizumab on treatment decisions in rheumatoid arthritis and giant cell arteritis
Other bDMARDs/tsDMARDs used to treat patients with COVID-19 were sarilumab (58 of those 728 who felt knowledgeable to answer this question, 8%), baricitinib (n=55, 8%), canakinumab (n=20, 3%) and/or anakinra (n=103, 14%).
A recommendation for patients with RMDs to decrease or stop nonsteroidal anti-inflammatory drugs (NSAIDs) even when they did not have symptoms of COVID-19 in order to decrease the possible risk for a worse outcome of this disease was made by 151/998 (15%) and 15 (2%) of respondents, respectively. Similarly, 226/1000 (23%) and 1 (0.1%) recommended to decrease or stop glucocorticoids, respectively.
Discussion
The magnitude of the impact of COVID-19 on both management decisions and quality of care of patients with RMDs has been unknown. The most worrisome findings, although not unexpected, are the fact that the lag between symptom onset to first rheumatological visits was increased during COVID-19 related closure, and that treatment decisions, particularly those to start a new b/tsDMARD were postponed mainly because of patients’ concerns to start a new treatment during the pandemic, but also due to limited availability of rheumatological services and/or screening tests. COVID-19 thus impacts heavily on two fundamental principles of rheumatology management, namely those of early diagnosis and treat to target.8 9 While we know from previous studies that long-term non-adherence to these strategies results in worse clinical and structural outcomes, the question to what extent a short-term interruption due to an infectious crisis impacts patients’ disease course is still unclear.8 10 See box 1 for the lessons learnt from this wave of the COVID-19 pandemic.
Lessons learnt from this wave of COVID-19 pandemic
Patient communication needs to be improved in order to address patients’ concerns about the risk of infection and course of new viral epidemics such as COVID-19, particularly if a new disease modifying anti-rheumatic drug therapy is planned.
Telemedicine and other models of care should be regularly assessed and researched more intensively in order to maintain high-quality of care even when face-to-face visits are not feasible.
Off-label use of drugs for COVID-19 indication outside a clinical trial might lead to shortage of the respective substance for patients with rheumatic and musculoskeletal diseases (RMDs) and should be discouraged.
Prioritising strategies for face-to-face visits and investigations such as laboratory testing, imaging and others should be developed in order not to delay diagnosis and treatment, and to guarantee adequate monitoring of disease activity and safety of patients with RMDs.
EULAR provisional recommendations for the management of RMDs in the context of SARS-CoV-2 suggest to consider withholding face-to-face visits temporarily or transforming them into a remote visit in phase of closure when the rheumatic disease is stable.11 According to the results of our survey, rheumatology service providers compensated for cancelled/postponed face-to-face visits using telemedicine, and many of them developed standard operating procedures to prioritise patients for face-to-face visits. Recent publications also indicate rapid development of telemedicine during the first wave of the pandemic,12–14 however, it seems that patients’ acceptance of telemedicine is only moderate yet.15 16 Besides, we have insufficient data on the effectiveness of telemedicine in rheumatology and need to know more about how and when telemedicine might efficaciously replace live visits.17 Given the expected increase in the prevalence of inflammatory and non-inflammatory RMDs in future due to an ageing population and other reasons, and the expected insufficient growth of workforce in rheumatology,18 19 telemedicine and strategies to better prioritise visits are essential to maintain high quality of care in RMDs, irrespective of additional waves of the COVID-19 pandemic.
Another lesson we learnt from this crisis is that we need to better address patients’ concerns and fears about possible risks of immunosuppression in order not to delay treatment of new or active patients. Till today, there is no convincing evidence suggesting that patients with RMDs (regardless of whether or not they are taking DMARDs) are at an increased risk for COVID-19 infection and course as compared with the general population.20 21 Many advisories, including official government bodies nevertheless considered these patients at risk with corresponding communications to patients’ societies, which might have further increased patients’ concerns to adhere to hospital visits and immunosuppressive therapy.22–26
Another observation is that management of RMD patients during closure was mainly based on patient’s history and clinical examination, given that non-urgent tests were either not available or not desired by patients. Some of these tests such as imaging are important to inform rheumatologists who establish a diagnosis and to aid monitoring of disease status and disease activity.27–29 Similarly, laboratory tests are essential to guarantee patients’ safety in case a new DMARD is considered but also for those who are on stable drug treatment.30 Investigations performed in the office as part of the clinical visit (eg, ultrasound conducted by the rheumatologist) or on a domestic basis (eg, blood tests) might be preferable over those requested from another department or hospital service, in order to reduce (patients’ concerns about) the contact to other patients and hospital-based structures.
HCQ was used for the COVID-19 indication according to almost half of respondents for inpatients and outpatients and occasionally for prophylaxis. The common use of this drug in this off-label indication led to a shortage in several countries and consequently, about 10% of patients with RMDs had to stop it at least temporarily. A shortage of TCZ occurred mainly in Italy and Spain, two countries who were heavily affected by the COVID-19. Clinicians might have been pressured to try every drug with possible efficacy in critically ill patients, however, the use of HCQ and TCZ for COVID-19 was not based on solid data rather than on theories about the mode of action, case series and small observational studies.31–33 Recent studies indicate that HCQ is not beneficial for COVID-19,34 35 and some evidence suggests that it might perhaps increase mortality when combined with azithromycine.36 Patients with inflammatory RMDs, particularly those with connective tissue disease, might be at a considerable risk of flare when they run out of HCQ.37 A comparable problem arises for TCZ: while a change to another bDMARD/tsDMARD (at least in RA) might be considered in case of drug shortage, this is definitely not desirable due to the risks of intolerance and lack of efficacy. Our survey indicates that in fact, this has been performed only occasionally in clinical practice. While there is some evidence from observational studies and non-randomised trials that TCZ helps to reduce the mortality of patients with COVID-19 who develop severe (autoinflammatory) pneumonia,38 the randomised phase III (COVACTA) trial comparing TCZ with placebo in patients with severe COVID-19 associated pneumonia failed its primary endpoint of improved clinical status, as well as the key secondary endpoint of reduced mortality.39 Almost 60% of those 423 physicians/HPR who stated that TCZ had been used in their hospital/practice for patients with COVID-19 indicated off-label use of this drug outside a clinical trial, an ethically questionable approach that is discouraged by EULAR.11
NSAIDs, which have been concerned to upregulate ACE 2 receptors and to increase the susceptibility to the virus,40 and glucocorticoids, which might negatively affect virus clearance,41 should not automatically be stopped in patients with RMDs according to the EULAR task force.11 Even patients with symptoms of COVID-19 who are chronically treated with glucocorticoids should continue this treatment.11 Interestingly, 23% of respondents advised their patients to reduce the glucocorticoid dose and 15% that of NSAIDs, presumably not to expose patients to unnecessary risk during the pandemic. Discontinuation of these drugs, however, was the exception.
Our study is limited by the descriptive nature and by a potential responder bias. There were more responses from Romania and the Netherlands, countries with a relatively small population, than from the UK, Spain, France or Germany. We followed the same dissemination strategy of the survey in every country, so any imbalance in the number of responses compared with the expected target population may be due to factors beyond our control (eg, different communication strategies of national societies). Furthermore, owing to its anonymous nature, the survey could have been completed by different healthcare providers within the same centre, and we were unable to contact respondents to solve any data inconsistency. Two respondents, for example, indicated no cancellation of first or follow-up visits despite complete closure of their rheumatology service. While there might be a plausible explanation for this answer (eg, patients were sent to another rheumatologist), we were unable to clarify it. We did not ask to stratify the responses on prioritisation strategies according to diagnosis, acknowledging that the diagnosis (eg, inflammatory arthritis vs systemic RMDs) might have had an impact on these strategies.
Our study reflects experiences and opinions of physicians and HPR from EULAR countries and despite its limitations, this survey provides important insights into management decisions concerning patients with inflammatory RMDs during the COVID-19 outbreak. Retrieval of empiric data to respond to the questions raised was certainly not feasible during this wave of the pandemic.
In conclusion, measures related to containment of the COVID-19 pandemic led to a perceived delay between symptom onset and a first rheumatological visit, a postponement of treatment decisions, and a shortage of drugs used to treat RMDs patients and those with COVID-19 such as HCQ and TCZ. Important lessons we have learnt are the need to better address patients’ concerns about the risk of infection and course of COVID-19, particularly in case a new DMARD is planned. Telemedicine and prioritising strategies should be researched more extensively in order to maintain high quality of care even when face-to-face visits and other investigations, such as laboratory testing or imaging, are not feasible, for example, during a future wave of the COVID-19 pandemic.
Acknowledgments
The authors are grateful to all physicians/HPRs that completed the survey, the national societies of EULAR countries, the EMerging EULAR NETwork (EMEUNET) and the EMEUNET Country Liaisons for their help with distributing the survey. The authors would also like to acknowledge Dr Nelly Ziade, Dr Milan Bogojevic, Professor Ori Elkayam, Mrs Elena Kazakova, Professor Nemanja Damjanov, Professor Mahmoud Abu-Shakra, Mrs Stefania Volpinari, Haner Direskeneli, Mrs Mimoza Maar, Igor Medojevic, Professor Elena Kartvelishvili, Dr Rima Akhvlediani, Dr Nana Kalandadze, Dr Artur Kollcaku, Dr Hilde Berner Hammer, Dr Sebastian Rodriguez Garcia, Professor Natalia Martusevich, Dr Su-Ann Yeoh and Ms Polina Pchelnikova for the support in collecting information regarding containment measures across European Countries. PMM is supported by the National Institute for Health Research (NIHR) University College London Hospitals (UCLH) Biomedical Research Centre (BRC). The views expressed are those of the authors and not necessarily those of the National Institutes of Health (NIH), (UK) National Health Service (NHS), the NIHR or the (UK) Department of Health.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Désirée van der Heijde
Twitter @pedrommcmachado, @FranciscaSivera
Contributors All authors designed the study and contributed to data collection. CD analysed the data and drafted the first version of the manuscript. All coauthors critically interpreted the results, discussed the findings together, critically reviewed the manuscript and approved its final version.
Funding This study was funded by the European League against Rheumatism (EULAR), project number EPI025.
Competing interests CD received consulting/speaker’s fees from Abbvie, Eli Lilly, Janssen, Novartis, Pfizer, Roche and Sanofi, all unrelated to this manuscript. AA has nothing to disclose. JWJB received honoraria from Lilly, Roche, Abbvie, Galapagos, SUN all unrelated to this manuscript. AB received research granst form Abbvie and Celgene, and consultation/speakers fees from Eli Lilly, Novartis, UCB and Galapagos all to here department and all unrelated to this manuscript. BC received honoraria from AbbVie; BMS; Gilead; Janssen; Lilly; Merck; Novartis; Pfizer; Roche-Chugai; Sanofi; and research grants from Novartis, Pfizer and Roche; all unrelated to this manuscript. AF has nothing to disclose. PMM received consulting/speaker’s fees from Abbvie, BMS, Celgene, Eli Lilly, Janssen, MSD, Novartis, Pfizer, Roche and UCB, all unrelated to this manuscript. IP received honoraria from Novartis, Sanofi, Abbvie, Sandoz and Roche, all unrelated to this manuscript. FS has nothing to disclose. TAS has nothing to disclose. FB received consulting/speaker’s fees from Abbvie, Lilly, Horizontherapeutics, Pfizer and Roche/Chugai, all unrelated to this manuscript.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. The data will be shared if there is a reasonable request for it.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.