Article Text

Abstract
Objective To evaluate active inflammatory lesions (AIL) and structural changes (SC) in patients with active non-radiographic axial spondyloarthritis (nr-axSpA) compared with patients with ankylosing spondylitis (AS) on whole-body MRI (wb-MRI).
Method 75 patients with active disease and a symptom duration of <5 years (39 with AS and 36 with nr-axSpA) were investigated with a comprehensive wb-MRI protocol and scored for AIL and SC in the spine, sacroiliac joints (SIJs) and non-axial manifestations.
Results 92% of patients with AS showed active inflammation in the SIJ, 53% in the spine and 94% and 39%, respectively, in the nr-axSpA group. There was a non-significant trend towards more inflammation in patients with AS compared with patients with nr-axSpA in SIJs and spine. Peripheral enthesitis/osteitis was more common in patients with AS (n=22) than in those with nr-axSpA (n=12) (p=0.05). SC were more common in patients with AS than in those with nr-axSpA, with significantly higher scores for SIJ fatty bone marrow deposition (FMD) in patients with AS (4.8±3.2) compared with those with nr-axSpA (2.4±2.7; p=0.001) and more frequent bone proliferation in the spine and the SIJ (p=0.02 and p=0.005, respectively). SIJ erosions were more common in AS (score 4.2±2.3) than in nr-axSpA (score 3.8±1.8) patients (not significant).
Conclusions Wb-MRI detects active inflammation and SC more frequently in the SIJs than in the spine. Half of the patients showed inflammation in non-axial sites. Active inflammatory and structural lesions were present both in patients with AS and those with nr-axSpA, being only slightly more common in patients with AS.
Statistics from Altmetric.com
Introduction
With the development of the new Assessment of SpondyloArthritis international Society (ASAS) classification criteria for axial spondyloarthritis (SpA),1 the study of early manifestations has become a prime target for rheumatological research. More recently, cohorts of patients with early axial SpA have been studied.2–4
MRI can detect active inflammatory lesions in bone marrow and soft tissue and is now widely accepted as the most sensitive imaging modality for detecting sacroiliitis and early spondylitis.5–9 Growing evidence also exists that MRI can detect the extent of structural changes (SC) in the spine and sacroiliac joint (SIJ).10 ,11 Recently, active inflammation of the SIJ and spine as shown by MRI have been defined in more detail by an international expert panel.12 ,13
SpA, despite its primary manifestation at the axial skeleton, is known to also affect peripheral sites, predominantly the lower extremities.14 ,15 Whole-body MRI (wb-MRI) is a new clinical tool that is currently under scientific investigation.16 ,17 This new imaging modality is especially useful to detect early disease manifestations of SpA at different sites of the skeleton.18 This method has been validated against conventional MRI19 and its diagnostic utility has been defined recently.20 However, there is only limited information on inflammation of peripheral joints and entheses in early disease.
The aim of this study was to describe the extent of active inflammation and SC at the SIJ, spine and non-axial sites by wb-MRI in a cohort of patients with axial SpA with a disease duration of <5 years and to examine potential differences between patients with radiographic sacroiliitis (ankylosing spondylitis (AS) group) patients with non-radiographic axial SpA (nr-axSpA).
Patients and methods
Study design
The study population of 75 patients with proven axial SpA and a symptom duration of <5 years was divided into two groups: one group of 39 patients with AS (AS group) with radiographically proven sacroiliitis (grade 2 on both sides or at least grade 3 on one side) and a second group comprising 36 patients with nr-axSpA. Here we analyse the baseline MRI data from an investigator-sponsored trial with the primary focus on treatment effects of etanercept in comparison with sulfasalazine (results reported in Song et al21 in more detail).
Inclusion and exclusion criteria
Retrospectively, all patients fulfilled the recently published ASAS classification criteria for axial SpA.1 All patients had to have chronic low back pain with a duration of <5 years, a Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) ≥422 and back pain score (BASDAI question 2) of ≥4, despite treatment with non-steroidal anti-inflammatory drugs and had to have active inflammatory lesions (osteitis) on wb-MRI in either the SIJ or the spine. Other inclusion criteria are described elsewhere.21 All patients underwent investigation with the same wb-MRI device.
Whole-body MRI
Wb-MRI was performed on a 1.5 Tesla scanner (Avanto, Siemens, Germany). Coronal T1-weighted fast spin echo sequences and short τ inversion recovery (STIR) sequences were performed according to a previously described protocol,18 including the head, neck, chest, chest wall, abdomen, pelvis and lower extremities, excluding elbow, hand and toe joints.
Scoring of wb-MRI
All MR images were scored independently by two musculoskeletal radiologists for active inflammatory lesions and chronic SC in the SIJs and the spine including the posterior segments. Non-axial (peripheral) inflammatory changes and SC were scored in consensus reading sessions.
To evaluate both types of changes by wb-MRI, a scoring method covering the entire body, was applied as briefly described by our group21 ,23 (table 1).
SIJ and spine
In general, the scoring system for inflammation, mainly osteitis, and SC (fatty bone marrow deposition (FMD), erosions, bone proliferation) has been constructed as proposed by MRI experts from ASAS.12 ,24 For extensive descriptions of the scoring system see table 1.
Briefly, active inflammation is defined as increased STIR signal with corresponding T1 signal loss, denoting active inflammatory lesions, according to a slightly modified previously described scoring method.25–27 Each SIJ was divided into four quadrants (score 0–24) and the spine into 23 vertebral units (VUs) with a score between 0 and 69. Scoring for active inflammatory lesions of the posterior segments included the facet joints and the spinous processes in each VU, and the costovertebral and costotransverse joints of the thoracic spine (taking into account both sagittal and coronal STIR sequences). SC of SIJ and spine are defined as described by Rudwaleit et al12 and Hermann et al.24
The SIJ and the spine MRI scores were calculated from the mean values of both scorers.
Non-axial manifestations
Manifestations not affecting the spine or SIJ are termed as non-axial (peripheral) sites for the purpose of this paper. Both active lesions and structural damage were evaluated at joints and entheses. For active inflammatory lesions, joints and bursae which comprise synovial tissue were scored. Insertion sites without the presence of synovial tissue were scored separately.
The following sites were scored for synovitis/effusion: shoulders, the sternoclavicular joints, hips, knees, ankles and Achilles tendon bursae. In addition, the following entheses were evaluated for osteitis and soft-tissue oedema: tendon insertions at the humerus and acromion, joint capsule insertions at the sternoclavicular joints, sternal synchondrosis, costosternal junctions, tendon insertion at the iliac crest, ischial tuberosity, lower border of the sacrum (the insertion site of the sacrococygeal ligament), pubic symphysis, tendon insertions at the hip joints, greater trochanter of the femur, femoral condyles, tibial plateau, the insertion sites of the Achilles tendon, the plantar fascia at the calcaneus and the ligamentous insertion sites at the intertarsal joints of the mid-foot.
The presence of erosions was investigated at the shoulders, the sternoclavicular joints, hips, knees and ankles.
A high signal on STIR images within the bone marrow or surrounding soft tissue was considered as enthesitis. Synovitis/effusion was categorised by the amount of fluid collection in the joint capsule. Bony erosions were scored as cortical defects in T1-weighted sequences.
Statistical analysis
The non-parameteric Wilcoxon test and χ2 test were used to compare differences between patient groups. To measure the inter-reader reliability the intraclass correlation coefficient was calculated. p Values <0.05 were considered significant.
Results
Baseline characteristics
Seventy-five patients with axial SpA were included into our study. Patients’ characteristics did not show statistically significant differences for the patients with axial SpA with radiographic and those without radiographic sacroiliitis (table 2).
Clinical characteristics of study patients at baseline, by AS/nr-axSpA
All patients had active disease as shown by elevated BASDAI values, high values for patient global and physician global assessment, elevated values for C-reactive protein (52% of patients) and erythrocyte sedimentation rate, and MRI showing active inflammatory lesions in the SIJ and/or the spine.
MRI findings
In the total study group, 74 patients showed active inflammatory lesions in the axial skeleton, 39 of these only in the SIJs, four only in the spine (including the posterior elements), and 31of these in the SIJs and the spine.
Ninety-two per cent of patients with AS showed active inflammatory lesions in the SIJ, 49% in the SIJ and the spine, but only 5% in the spine but not in the SIJ compared with 94%, 33% and 6% in the nr-axSpA group. Thus, in patients with nr-axSpA, the spine was less often inflamed than in patients with AS, although this difference was non-significant (table 3).
MRI—active lesions and structural changes (SC) of the axial skeleton
Sacroiliac joints
At the SIJ, 93% of the patients (n=70) had active inflammation. The mean osteitis score in the SIJ was 6.7 (±5.8) out of 24 possible scoring points. The AS group showed more inflammation at the SIJ (osteitis score 7.6±6.3) than the nr-axSpA group (5.7±5.2) (table 3), but the difference was not significant.
Structural changes: FMD was detected in 38.9% of all SIJ quadrants. We found significantly more affected quadrants in the AS group (50.4%) with a significantly higher mean score per patient of 4.8±3.2, compared with 27% of affected quadrants and a mean patient score of 2.4±2.7 in the nr-axSpA group. Erosions were only slightly more common in patients with AS than in patients with nr-axSpA, but without significant differences (73.1% all patients, 74.2% patients with AS and 71.9% non-AS). Sclerosis was found in 76% of all patients (score 1.4±0.9 in AS and 1.1±0.8 in patients with nr-axSpA). Ankylosis was detected in 6.9% of quadrants. As expected, ankylosis was not present in the nr-axSpA group.
Analysis of each separate quadrant showed no significant differences in the amount of active inflammation or chronic changes. In detail, active inflammation was present in quadrant I (sacral bone, upper quadrant) in 50 patients (67%), in quadrant II (sacral bone, lower quadrant) in 45 patients (60%), quadrant III (iliac bone, lower quadrant) in 52 patients (69%) and quadrant IV (iliac bone, upper quadrant) in 40 patients (53%).
Spine
Active inflammatory changes were rather low grade in the spine (spine osteitis score of 1.9±3.3 out of 69 possible scoring points) compared with the SIJ (SIJ osteitis score 6.7±5.8 out of 24). The most common sites of inflammation were the lower thoracic spine and the lumbar spine (figure 1). Mean spine osteitis scores in the AS group were more than double those in the nr-axSpA group; however; owing to the overall low spinal activity no statistically significant differences were found (table 3).

Frequency of active inflammation in the spine (vertebral units). AS, ankylosing spondylitis; nr-axSpA, non-radiographic axial spondyloarthritis.
The posterior segments showed signs of active inflammation significantly more often in the AS group (n=10) than in the nr-axSpA group (n=3). Of note, just one patient showed inflammation only in the posterior elements and not in the vertebral bodies in the group of patients with nr-axSpA.
SC in the vertebral bodies were clearly less common in the spine than in the SIJ, with <1% of the VUs showing erosions and <5% FMD. On the patient level, FMD was the most common structural change (n=23 patients, mean score 1.8±4.6) compared with structural damage-like erosions (n=13 patients, mean score 0.2±0.6) and bone proliferation (n=9, mean score 0.5±1.9). Comparison of AS and the nr-axSpA groups showed that FMD, erosions and bone proliferation were found more often in patients with AS (table 3), but only bone proliferation showed a statistically significant difference (p=0.0193) on the spine.
There was a high agreement between both scorers with an intraclass-correlation coefficient (ICC) of 0.93 for assessing active inflammatory lesions of the spine and ICC of 0.96 for the SIJs. ICCs for detection of FMD were 0.97 for the SIJ and 0.90 for the spine, 0.90 and 0.75 for scoring of ankylosis and 0.86 and 0.82 for scoring of erosions, respectively.
Non-axial manifestations
A total of 58 patients (77%) showed signs of active inflammation, either enthesitis/osteitis or synovitis/effusion, beyond the spine and the SIJ.
Enthesitis was significantly more common in the AS group (n=22) than in the nr-axSpA group (n=12; p=0.0449). The distribution of enthesitis among non-axial sites is given in table 4. Inflammatory signs at ligament and tendon insertions were found most frequently at the pelvis. Multilocular enthesitis was significantly more common in the AS group than in the nr-axSpA group (p=0.0133).
Non-axial enthesitis/osteitis and synovitis/bursitis on MRI
Forty-five of all patients (60%) showed evidence of peripheral synovitis or bursitis, most of them (n=41) at multiple sites, with similar extent in both groups. The most common locations were the knees (32 patients) and ankle joints (25 patients), followed by the hips (seven patients).
Chronic changes: No erosions were detected in any patient of our cohort at the peripheral joints included in the analysis.
Discussion
In this study we compared MRI findings in patients with radiographic and nr-axSpA by wb-MRI. A total of 75 patients with active inflammatory sites in the axial skeleton were included. Both groups showed very similar clinical characteristics, including short symptom duration and a similar level of disease activity and laboratory characteristics (table 2). There was a trend towards a higher level of inflammation in the SIJs and the spine in the AS group, although this difference was not significant. Only the number of inflammatory sites in the posterior segments of the spine and at the peripheral entheseal sites was significantly higher in the AS group than in the nr-axSpA group. But these differences between the groups were rather small and do not allow the conclusion that patients with AS with more advanced SC in the bone have more active MRI inflammation than patients with non-axial SpA with similar symptom duration.
We give here for the first time a detailed description of the sites of inflammation in SIJs and spine in early axial SpA. Active inflammation was evident in all quadrants of the SIJ without significant differences, though with a trend towards more frequent affection of the lower quadrants. Similar findings were described by Weber et al17 and Muche et al.28
Active inflammation of the spine was present in 53% of patients with AS compared with 39% of those with nr-axSpA (difference not statistically significant). These data, together with recent results from Leeds showing inflammation in the spine in a cohort with early SpA (disease duration of up to 3 years) in only 22% of cases,29 indicate that early in the course of the disease, the spine is less often affected. This is further emphasised by data from the ASSERT study,30 where patients with advanced AS and a mean disease duration of 8.8 years were included and showed active spinal inflammation in 77% of cases.
Inflammatory lesions were most often present in the lower thoracic and lumbar spine both in patients with nr-axSpA and patients with AS in our cohort (figure 1). Involvement of the cervical spine was sparse. These observations are in line with the study by Weber et al.17 Earlier reports in patients with patients with more advanced AS by Baraliakos et al showed the lower thoracic spine as the predominant site of inflammation.31
Involvement of posterior spinal segments occurred infrequently, in 26% in patients with AS and in 8% in patients with nr-axSpA. In established AS with longer disease duration, involvement of posterior elements was described in up to 87% of patients affected.32 Our findings are in contrast to a recent publication by Bochkova et al,33 where much higher frequencies of posterior element involvement, especially in cases of early SpA, was reported (figure 2).

{kind=link}
{kind=link}
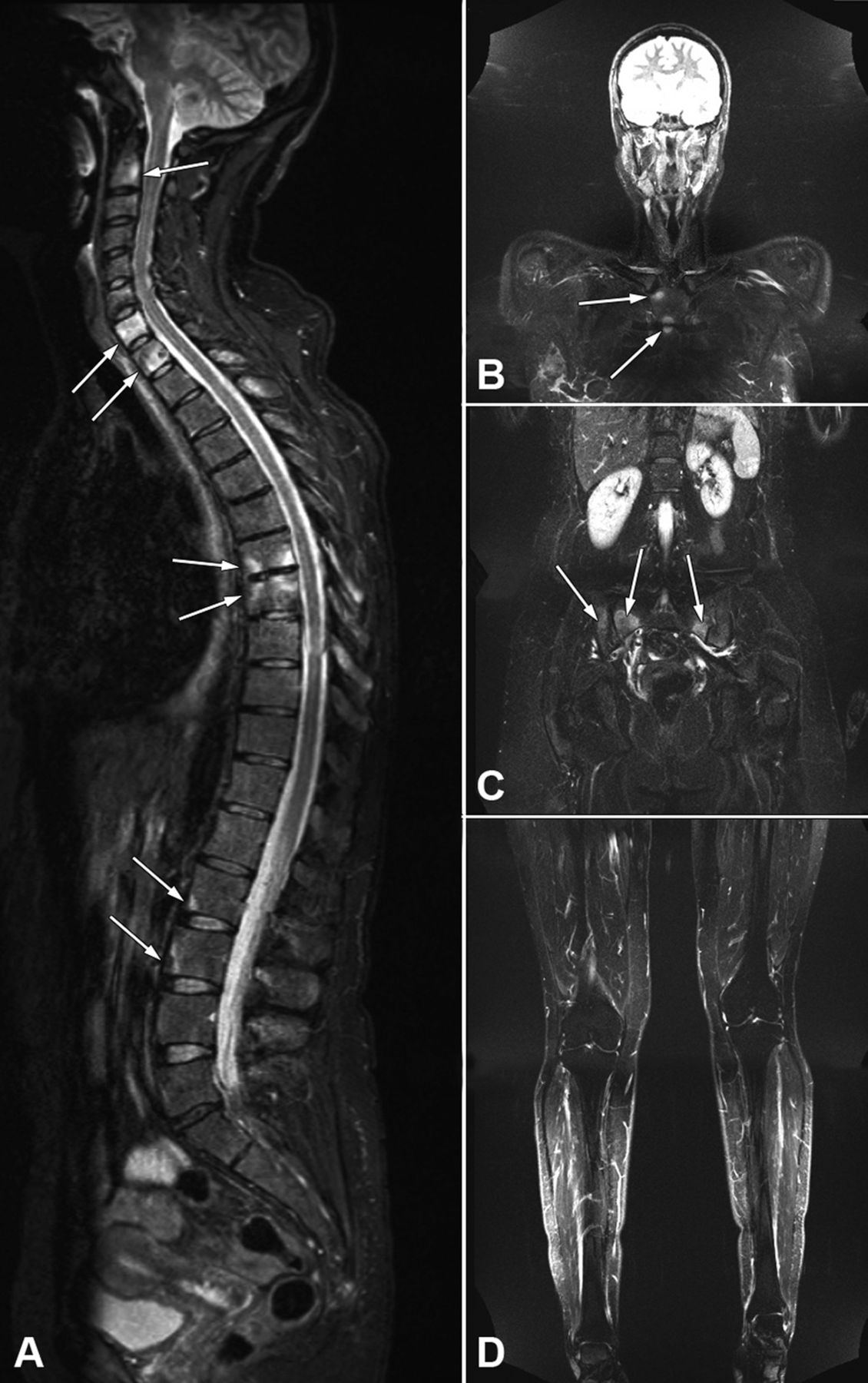
46-Year-old female patient. (A) Sagittal short τ inversion recovery (STIR) sequence of the whole spine showing osteitis lesions in several segments (arrows), most of them with the pattern of anterior or posterior spondylitis. (B–D) Coronal whole-body STIR sequence at different slice levels showing anterior chest wall manifestations (B, arrows) and osteitis due to sacroiliitis (C, arrows). Knees and ankles are also included in the MRI examination but are normal in this case (D).
Few studies so far have investigated the involvement of peripheral sites in SpA by MRI.16 ,17 ,34 Owing to its large coverage of body sites, wb-MRI seems to be the preferred method.16 Initial studies by Weber et al found that the anterior chest wall and hips were affected in early SpA and AS.17 In addition to the involvement of these sites, enthesitis and synovitis of the pelvis and lower extremities are common findings in our cohort. Some clinical scores of enthesitis focus on ligament insertions around the pelvis.35 Careful analysis of these sites by wb-MRI reveals lesions previously not described systematically—for example, sacrococcygeal entheses, iliac crest and ischial tuberosity, which are more frequently affected in patients with AS than in those with nr-axSpA. Inflammatory involvement of entheses of the feet was detected less often than expected.15
As expected, chronic structural lesions were more common in AS than in nr-axSpA, but predominantly in the SIJs, confirming that the disease starts in the SIJs. Erosions were evident in the spine in 25% of patients with AS and in only 8% of patients with nr-axSpA—however, erosions were evident in the SIJs in 85% and 89%, respectively. FMD was significantly more common in patients with AS than in patients with nr-axSpA, which underlines the dynamic process in the development of such lesions, even in the early stage of disease. It has been discussed that such fatty lesions are probably a sequel of inflammation within the bone marrow.12 However, one report in patients with more advanced disease did not show a correlation of FMD with disease duration.6 It seems that the link between inflammation and structural damage is more likely to be found in early SpA.
Earlier work on wb-MRI in AS has been presented by Weber et al17 and our own group.16 ,36 The pilot study by Weber et al included the SIJs, spine, shoulders, anterior chest wall, hips and pubic symphysis.17 The approach applied by our institution goes beyond these locations and includes additional sites of the lower extremities which are commonly involved in SpA: knees, ankles, mid-foot joints, Achilles and plantar fascia entheses, applying both STIR and T1-weighted sequences. More than half of all patients showed inflammatory lesions on the lower extremities. Thus, the most comprehensive coverage of body sites and lesion types is achieved by our wb-MRI protocol. Active inflammatory lesions may also be imaged by giving intravenous contrast agents.34 However, this makes the procedure more invasive and increases the risk of adverse skin and renal reactions37 and does not provide significantly more information than STIR sequences38 ,39 on the SIJ and spine. But this has not yet been investigated for the imaging of the peripheral joints and entheses.
Some of the scores applied in our study were specifically developed for the analysis of wb-MRI. Active inflammation in the SIJs and the spine was scored as previously described.21 Structural damage of the spine was recorded in three independent domains (erosions, FMD and bone proliferation). Another method of scoring structural damage in the spine is the ASspiMRI-c score,40 which combines active inflammatory and chronic SC. However, using a scoring system evaluating all different domains of structural damage independently from active inflammation allows for more detailed quantification in cross-sectional and longitudinal studies.
Here we investigated only patients who were clinically active with an elevated BASDAI and active inflammation on MRI. Thus, at the moment we cannot generalise our results to all patients with AS and patients with nr-axSpA. A higher MRI inflammation score in AS compared with nr-axSpA has recently been reported in unselected patients.41
In summary, in this cohort of patients with early active axial SpA wb-MRI frequently shows structural damage at SIJs and to a lesser degree also at the spine. Active inflammatory and chronic lesions were only slightly more prevalent in AS than in non-radiographic axial SpA with similar symptom duration and similar clinical characteristics. Peripheral sites show active inflammation in about half of the patients. Wb-MRI contributes to the quantification of active inflammation and structural damage in patients with SpA.
Registration at the homepage clinicaltrials.gov (https://register.clinicaltrials.gov/) was done in November 2005 (registration number NCT00844142).
Acknowledgments
The authors thank Joachim Listing and Johanna Callhoff for statistical analysis and data preparation.
References
Footnotes
-
Contributors CA and KGH: MRI performance, study interpretation, designed the application to the study dataset, drafted and revised manuscript. JS: initiated the collaborative project, reviewed and revised the final manuscript. I-HS: organised the collaborative project and reviewed the final manuscript. TD, BF, MR, BH, HH: assisted with the collaborative project and reviewed the final manuscript. AW: wrote the statistical plan, analysed and assembled data in tables and reviewed the final manuscript.
-
Funding This study was supported by Wyeth/Pfi zer.
-
Competing interests CEA, AAW, TD and KGH: none; JS, I-HS, HH and MR: consulting fees or other remuneration from Wyeth/Pfizer, Merck Sharp Dohme/Schering Plough, Abbott Immunology Pharmaceuticals, UCB; BF: former employee of Pfizer/Wyeth.
-
Patient consent Obtained.
-
Ethics approval Ethics approval was granted by Landesamt für Gesundheit und Soziales, Geschäftsstelle der Ethik-Kommission des Landes, Berlin, Germany.
-
Provenance and peer review Not commissioned; externally peer reviewed.