Article Text

Abstract
Background Tumour necrosis factor (TNF)-inhibiting therapy increases the risk of serious infections in rheumatoid arthritis (RA). However, it is not clear whether this risk differs between TNF inhibitors.
Objective To analyse whether the risk of serious infections in patients with RA treated with an anti-TNF inhibitor is different for adalimumab, infliximab and etanercept.
Methods Data from the Dutch RA monitoring registry were used. Incidence rates were calculated from the observed number of first serious infections and follow-up time up to 5 years. A Cox proportional hazards model with time-to-first-serious infection was used to estimate risk differences among the anti-TNF treatment groups, with correction for confounders.
Results The unadjusted incidence rate of a first serious infection in patients with RA per 100 patient-years was 2.61 (95% CI 2.21 to 3.00) for adalimumab, 3.86 (95% CI 3.33 to 4.40) for infliximab and 1.66 (95% CI 1.09 to 2.23) for etanercept. Age, year of starting anti-TNF therapy, comorbidities at baseline and disease activity score 28 over time were included as confounders. No difference in risk for serious infections was found between adalimumab and infliximab with an adjusted HR (adjHR) of 0.90 (95% CI 0.55 to 1.48). The risk of serious infections was significantly lower in etanercept than in both infliximab (adjHR=0.49 (95% CI 0.29 to 0.83)) and adalimumab (adjHR=0.55 (95% CI 0.44 to 0.67)).
Conclusions The risk of serious infections in patients with RA treated with adalimumab or infliximab was similar, while the risk of serious infections in patients with RA treated with etanercept was lower than with both adalimumab and infliximab.
Statistics from Altmetric.com
Introduction
The inhibition of tumour necrosis factor α (TNF) by adalimumab, infliximab and etanercept is effective in reducing inflammation in patients with rheumatoid arthritis (RA) and results in reduction of signs and symptoms and better outcomes. However, TNF plays an essential part in the host-immune system.1 Inhibition of TNF may lead to an increased risk for infections in patients with RA, who already are at risk because of their underlying disease and use of immunosuppressive drugs.2 Several observational studies showed a modest increase in risk for serious infections during TNF-inhibiting therapy in comparison with disease-modifying antirheumatic drug (DMARD) therapy.1 ,3–8 This increased risk has been confirmed in a number of reviews and meta-analyses.9–12 While the risk appears similar for adalimumab and infliximab a trend towards a lower risk for etanercept has been seen, although not statistically significant.4–6 ,8 ,12–17 A Cochrane review (2011) of randomised controlled trials and open-label extension studies did indicate a lower risk for etanercept for adverse events, but there were no clear differences for serious infections.1 ,18 While anti-TNF agents have not been compared directly in a randomised controlled trial, head-to-head comparisons of these agents make use of observational data. Differences in infection risk could be explained by the different mode of action of infliximab and adalimumab in inhibiting TNF compared with etanercept.1 ,19 ,20 These possible differences among TNF inhibitors emphasise the urgent need for more research into the comparative safety of different biological agents, notably using head-to-head comparisons.18
Therefore, the objective of this study was to analyse whether the risk of serious infections in patients with RA starting TNF-inhibiting therapy is different for adalimumab, infliximab and etanercept, in a head-to-head comparison with a follow-up time of up to 5 years.
Methods
Design
This was a prospective cohort of patients with RA starting their first TNF inhibitor—namely, adalimumab, infliximab or etanercept, with a follow-up time of up to 5 years. None of the patients starting anti-TNF therapy in the Dutch RhEumatoid Arthritis Monitoring (DREAM) registry had previously used another biological agent. Data were extracted from the DREAM biological registry (since 2003) and a preceding biological registry from the Radboud University Nijmegen Medical Centre (RUNMC) (before 2003), both with the same inclusion criteria and work flow. The DREAM registry is a multicentre registry of RA in daily clinical practice.21 All patients with RA who start a biological agent for the first time (biological agent-naïve) in one of 13 participating hospitals in the Netherlands are included in the DREAM biological registry. In the Netherlands, outpatient rheumatological care is always hospital based. Data collection in DREAM is continued when patients have stopped using biological agents. Written informed consent was obtained after the patient had been informed verbally and in writing about the study by their attending rheumatologist. Approval for this study was obtained from the ethical committee.
Patients
Inclusion criteria for the registry are in line with the Dutch regulations for reimbursement of TNF-inhibiting therapy: (1) all patients with a diagnosis of RA according to the 1987 American College of Rheumatology classification criteria, who have a 28-joint Disease Activity Score (DAS28) >3.2; (2) who have had prior treatment with at least two DMARDs including methotrexate (MTX; weekly dose up to 25 mg, if appropriate); (3) who have no contraindication for TNF-inhibiting therapy.
All patients using etanercept, adalimumab or infliximab as initial TNF-inhibiting therapy extracted from these two registers were included in the analyses; patients were excluded if they had previously participated in a trial of TNF inhibitors.
Data collection
Information on patient characteristics, disease activity measures, disease duration, extra-articular manifestations and comorbidities before the start of anti-TNF therapy and treatment information was collected during outpatient visits and prospectively entered into the database. Clinical assessments were performed by trained research nurses at baseline every 3 months for the first 2 years and every 6 months thereafter. During each visit, patients were asked about any adverse event since the previous visit. All clinical information was prospectively entered in a computerised database.
Baseline characteristics
The baseline data included gender, age and weight, disease activity (DAS28), erosiveness, rheumatoid factor status and disease duration, use of corticosteroids and MTX, total number of DMARDs in medical history. Felty's syndrome, rheumatoid noduli, pericarditis, pleuritis, keratoconjunctivitis and rheumatoid vasculitis were regarded as extra-articular manifestations. Presence of cardiovascular disease, diabetes mellitus, chronic obstructive pulmonary disease and leucopenia were regarded as comorbidities, possibly relevant to the occurrence of serious infections.
Time-dependent variables
Dose of MTX, dose of corticosteroids, disease activity (DAS28), visual analogue scale (VAS) pain, Health Assessment Questionnaire, and comorbidities— chronic obstructive pulmonary disease, leucopenia, cardiovascular disease and diabetes, were measures that were allowed to vary over time during the follow-up period of 5 years and were computed as time-dependent covariates with 6-month intervals.
Serious infections
Infections were classified by a doctor according to the Federal Drug Administration definition of a serious adverse event—that is, one needing hospitalisation and/or intravenous antibiotic therapy, is life threatening or leading to persistent or significant disability.22 All serious infections were categorised: septicaemia; skin and soft tissue infections; upper respiratory tract infections; lower respiratory tract infections; ear nose and throat infections; intra-abdominal infections; musculoskeletal infections; cardiovascular infections and miscellaneous serious infections. Opportunistic infections were included if satisfying the definition of ‘serious infection’.
Missing data
Missing values in baseline variables were imputed to increase precision and to avoid bias. Weight, tender and swollen joint count, erythrocyte sedimentation rate, VAS general health, Health Assessment Questionnaire, VAS pain, presence of erosions and rheumatoid factor had missing values (with a maximum of 36%).
Multiple imputation was used for missing values with a linear regression method with a random component, conditionally on being missing at random.
DAS28 was missing in 22.2% and calculated with the imputed values of tender joint count, swollen joint count, Erythrocyte Sedimentation Rate (ESR) and VAS general health.
Statistical analyses
Patients contributed person-years of follow-up for the period in which they were treated with their first TNF-inhibiting agent, plus five times the half-life of the specific TNF-inhibiting agent; which becomes 15 days for etanercept, 45 days for infliximab and 70 days for adalimumab. After five times the half-life less than 5% of the working metabolites are circulating in the blood.
Follow-up ended after up to 5 years, or sooner: when the first TNF inhibitor was stopped, or after occurrence of a first serious infection.
Survival analysis with Kaplan–Meier plots was used to describe time until occurrence of a first serious infection for each of three TNF inhibitors. Only first serious infections were analysed. Incidence rates for serious infections were calculated from the observed number of first serious infections divided by the number of patient-years exposure to TNF-inhibiting therapy.
Baseline differences between the three treatment groups in patient, disease and treatment characteristics were analysed using one-way analysis of variance, χ2 test or Kruskal–Wallis test, as appropriate.
Survival analysis, by a Cox proportional hazards model using the pooled dataset resulting from multiple imputation with time-to-first-serious infection as dependent variable, was used to estimate risk differences between the three treatment groups, with correction for (time variant) confounders. Variables (baseline variables and time varying variables in table 1) were regarded as acting as confounders if the regression coefficient of the main effect (TNF-inhibiting agent) in the Cox proportional model changed by at least 10% when adding the variable to the model using a forward selection approach. The risk difference between adalimumab, infliximab and etanercept were given as adjusted HRs (adjHRs) and 95% CI.
Baseline variables
The proportional hazard assumption was checked by graphical inspection of the linearity of the hazards over time and log−log plots and by plotting Schoenfeld residuals over time.
Sensitivity analyses were performed with different values of the risk window extension: 0 months and 1 month after stopping the first anti-TNF inhibitor, and by only studying patients since 2004 when all three agents were available. In addition, analysis of whether the effect of a TNF-inhibiting agent on infection risk differed with age and gender (effect modification) was studied.
All analyses were performed using SPSS V.18.0, adopting a 5% level of significance (two-sided).
Results
Patient characteristics
By July 2011, 2515 patients were included in the DREAM biological registry and the biological registry from the RUNMC together. A total of 2356 patients were included in the analyses (2000 patients from the DREAM biological registry and 356 patients from the database of RUNMC). There were 621 (26%) patients using infliximab, 776 (33%) patients used adalimumab and 959 (41%) patients used etanercept as first TNF-inhibiting therapy (figure 1). The median (P25–P75) follow-up time in months was 16 (5–40) for etanercept, 19 (7–44) for adalimumab and 16 (5–56) for infliximab.
At the time of starting the TNF-inhibitor, the mean age of the patients was 54 years, most patients were female, and about half of the patients had high disease activity (table 1). There were small baseline differences between the three groups, nearly all of which were statistically significant.
Occurrence of serious infections
The total incidence of first serious infections was 125 with 4834.25 patient-years of exposure to TNF-inhibiting therapy, resulting in an incidence rate of 2.59 serious infections per 100 patient-years. The survival curves of time till occurrence of a first serious infection for each of the three TNF inhibitors are shown in figure 2. The proportion of patients who discontinued treatment for other reasons was low (6–9%) and similar for the three agents (figure 1). Most serious infections occurred within the first 2–3 years, therefore a follow-up time of 5 years was deemed appropriate. From figure 2, it can be seen that the occurrence of serious infections was lowest in patients using etanercept and highest in patients using infliximab. The curves diverged only after 6 months.
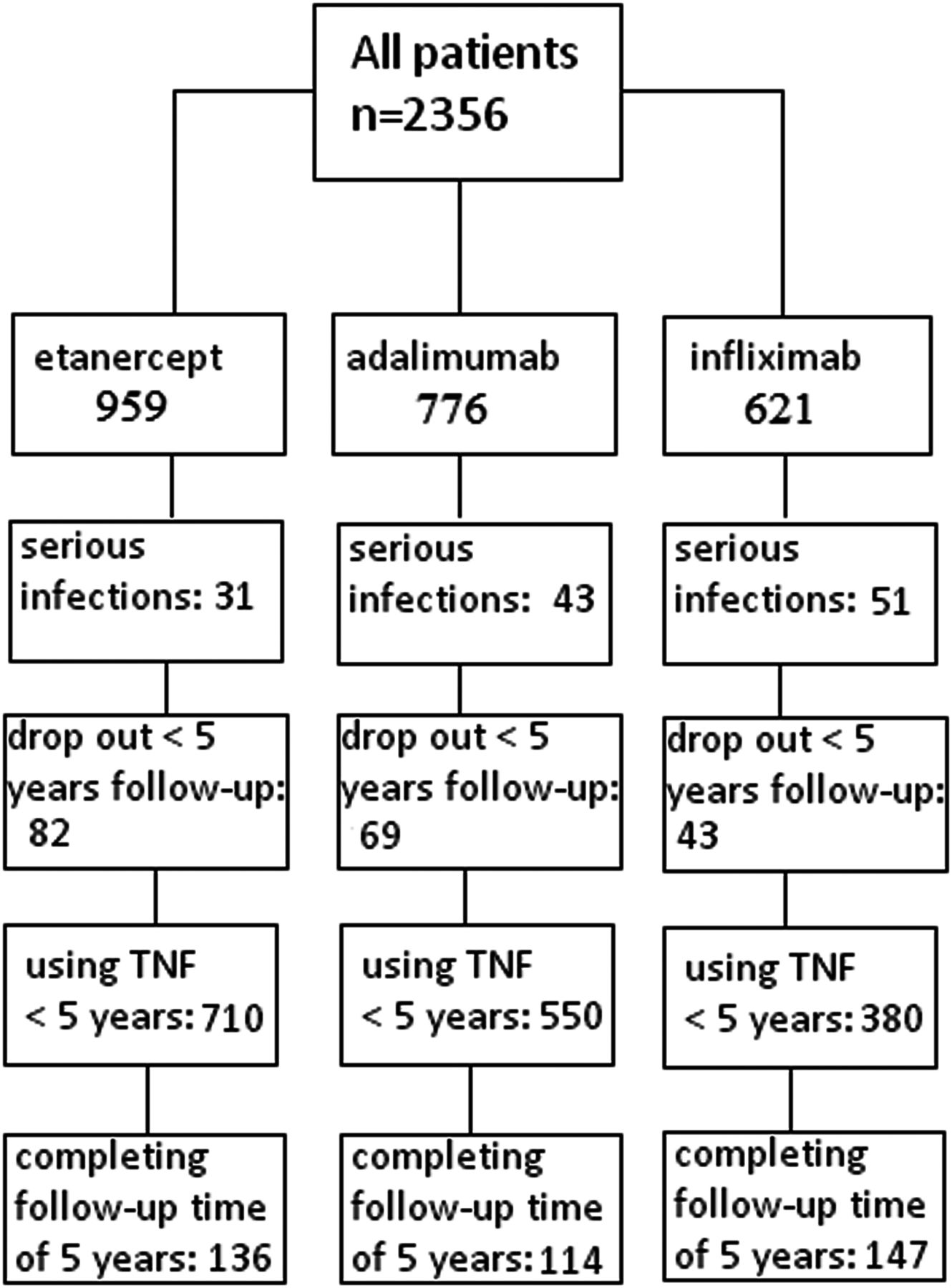
Flowchart of the inclusion of patients separately for each tumour necrosis factor (TNF) inhibitor. Serious infections: total of serious infections for each TNF inhibitor during a follow-up time of up to 5 years. Drop-out <5 years follow-up: total of patients who dropped-out from the study within 5 years follow-up owing to death, moving to another area, not wanting to participate any more, or a serious comorbidity. Using a TNF inhibitor for <5 years: the total of patients who had not dropped out with an observation time of <5 years. The last block represents the total of patients who completed a follow-up time of 5 years.

{kind=link}
{kind=link}
Survival curve of each tumour necrosis factor (TNF) inhibitor.
The unadjusted incidence rate of a first serious infection in patients with RA per 100 patient-years was 2.61 (95% CI 2.21 to 3.00) for adalimumab (patient-years of exposure: 1648.4 years), 3.86 (95% CI 3.33 to 4.40) for infliximab (patient-years of exposure: 1319 years) and 1.66 (95% CI 1.09 to 2.23) for etanercept (patient-years of exposure: 1866.83 years).
Difference between the three TNF inhibitors
In table 2 results of unadjusted and adjusted analyses of the differences in risk for adalimumab, infliximab and etanercept are shown as HRs of adalimumab versus etanercept and infliximab versus etanercept. The following variables acted as confounders: age, year of starting TNF therapy and the presence of comorbidities all at baseline; DAS28 varies over time and acted as a time-dependent confounder.
Results of the Cox proportional hazard model
Both the unadjusted and adjusted model showed a higher risk for adalimumab and infliximab than for etanercept (table 2), while the risks of infliximab and adalimumab were similar. Accordingly, no difference in risk of serious infections was found when comparing adalimumab and infliximab directly, with an adjHR of 0.90 (95% CI 0.55 to 1.48). The relative protective effect of etanercept can also be shown by reversal of the adjHRs. The risk of serious infections was significantly lower in etanercept than in both infliximab (adjHR=0.49 (95% CI 0.29 to 0.83)) and adalimumab (adjHR=0.55 (95% CI 0.44 to 0.67)).
At 6 months, there was no significant difference in occurrence of serious infections between the three anti-TNF agents. Proportional hazard assumptions were met.
Sensitivity analyses
For analysis of the primary outcome a risk window of observation time plus five times the half-life was used. There was no difference in results using risk windows extensions of 0 and 1 months.
When patients since 2004 only were analysed—that is, a time when all three agents were available, there was no difference in results. There was no difference in age and gender for the effects of an anti-TNF agent on serious infections.
Occurrence of serious infections by infection site
Table 3 shows the overall rates of serious infections for each TNF inhibitor categorised by infection site. Infections of the lower respiratory tract occurred the most frequently (36%).
Number of first serious infections by infection site
Discussion
TNF-inhibiting therapy increases the risk of serious infections in patients with RA compared with background DMARD therapy. The objective of this study was to analyse whether the risk of serious infections in patients with RA starting TNF-inhibiting therapy differs for adalimumab, infliximab and etanercept, in a head-to-head comparison.
According to the results of this study, there was a significantly lower risk of serious infections in patients with RA treated with etanercept compared with both infliximab or adalimumab, while there was no difference between adalimumab and infliximab. The adjusted hazard rates of etanercept compared with infliximab and adalimumab were 0.49 (95% CI 0.29 to 0.83) and 0.55 (95% CI 0.44 to 0.67). The adjusted hazard rate of infliximab compared with adalimumab was 0.90 (95% CI 0.55 to 1.48). The most common site of serious infections was the lower respiratory tract, which was also the case in some previous studies.3–5 ,8 This finding is in line with the major theoretical role of TNFα in adequate host defence mechanisms in the lung, supported by the high bronchoalveolar fluid TNFα level in the infected pulmonary lobes of patients with pneumonia.23
Previous short-term studies showed less serious infections in etanercept-treated patients, but without a significant difference between the three TNF inhibitors.12 Long-term observational studies showed a mixed picture for the risk of serious infection among adalimumab, infliximab and etanercept, with a trend towards a higher risk in adalimumab and infliximab-treated patients but without a significant difference.4–6 ,8 ,13 ,16 ,20 ,24 ,25 Head-to-head comparisons between the three TNF agents of the risk for serious infections were made in non-randomised observational studies.
The adjHR of serious infections found by Favalli et al5 was higher in adalimumab- (adjHR=1.73) and infliximab-treated patients (adjHR=1.48) than in etanercept. However, in another study the risk for serious infections of anti-TNF therapy compared with DMARD therapy, was similar for infliximab (adjHR=1.3), adalimumab and etanercept (adjHR=1.2 for both).6 A similar non-significant higher HR of 1.2 for anti-TNF therapy versus DMARD therapy was found in a large study in the British Biologics Register; however, the risk was 4.6 (95% CI 1.8 to 11.2) higher for anti-TNF in the first 90 days after treatment start, with a trend for infliximab to have the highest risk.14 Similarly, compared with infliximab, users of abatacept (HR=0.68, 95% CI 0.48 to 0.96), adalimumab (HR=0.52, 0.39 to 0.71), etanercept (HR=0.64, 0.49 to 0.84) and rituximab (HR=0.81, 0.55 to 1.20) had lower rates of hospitalised infection, but patient risk factors contributed more to the risk of infection than did the risk associated with specific biological therapies.13 In the most recent observational cohort study that investigated the difference between the three TNF inhibitors versus DMARDS, a higher adjHR for serious infections in infliximab was seen than with adalimumab (adjHR=1.23) and etanercept (adjHR=1.26).26 HRs did not differ significantly between adalimumab and etanercept. Two other recent studies comparing the risk of serious infections of etanercept and infliximab found no significant difference between these two TNF inhibitors (see supplementary table online).27 ,28
Recently a meta-analysis and a Cochrane review were carried out to compare the safety of biological agents.18 In this study which compared the individual biological agents with background treatment neither adalimumab, infliximab nor etanercept showed a statistically significant increase in serious infections; direct comparisons between the TNF inhibitors were not made. Interestingly, in this meta-analysis adalimumab and infliximab were associated with significantly higher numbers of total adverse events compared with controls, while etanercept was not.
An explanation for the difference between adalimumab and infliximab versus etanercept in the risk of serious infections and/or adverse events might be the different mode of action in inhibiting TNF between the monoclonal antibodies and the TNF receptor fusion protein.1 ,19 ,20 Etanercept is a soluble TNF receptor fusion protein and scavenges TNF from the circulation, whereas adalimumab and infliximab bind to circulating and membrane-bound TNF.29 TNFα-carrying cells are attacked by adalimumab and infliximab, causing impairment of their function, resulting in reduction of host immune responses. It has been suggested that the effect of an anti-TNF agent on infection risk might vary according to patient characteristics.28 However, such effects were not found in previous studies and our recent study.
The strength of our study is the large number of patients and the quality of the clinical data. The DREAM biological registry represents a large sample of patients with RA from the outpatient clinics of 13 hospitals in the Netherlands. As treatment of RA in the Netherlands is hospital based, this will not lead to selection bias and 90% of patients starting anti-TNF treatment in these hospitals are indeed in the registry, with no difference between the three agents. In the DREAM registry, all data are prospectively collected, with adverse events, treatment information and RA severity data recorded at each visit. Analysis could be performed with the inclusion of major possible confounders. We consider that inclusion of patients before 2003 from the database of the RUNMC did not influence the results. The database of the RUNMC was comparable with the DREAM biological registry and patients who had previously participated in a trial were not included. When analysing the DREAM register only, effects did not differ.
A limitation of our study is that patients were not randomly assigned between treatment options and therefore may differ in their prognosis for serious infections at baseline. However, this is a study into adverse events and confounding by contraindication is hardly operational, in contrast to confounding by indication in the unrandomised comparison of desired effects. In the Netherlands, there is no pressure from insurance companies or government to prefer one anti-TNF agent over another. Baseline differences were statistically significant but small, but nevertheless, correction was made for important confounders. Another limitation is the occurrence of missing values, which is inevitable in observational studies. However, omitting patients with missing values from the analyses would be inefficient and might lead to bias.30 Therefore, missing values were imputed by multiple imputation.
In conclusion, the risk of serious infections in patients with RA treated with adalimumab or infliximab was similar, while the risk for treatment with etanercept was significantly lower than with both adalimumab and infliximab. Further research is necessary to investigate why treatment with etanercept may have a lower risk of serious infections than both adalimumab and infliximab, and for which infections this is the case. A head-to-head comparison using meta-analysis of individual patient data from observational studies and including correction for confounders could be performed to acquire a robust estimate of differences in risk.
Acknowledgments
We thank all research nurses and rheumatologists of the 13 departments of rheumatology from the Netherlands for their participation in the data collection. We acknowledge Thea van Gaalen, Lia Schalkwijk, Carien Versteegden and Marjon de Lange-Brandt for data processing.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table
Footnotes
-
Contributors SAAvD made substantial contributions to the conception and design, analysis and interpretation of data and drafting of the manuscript. JF made substantial contributions to the conception and design, analysis and interpretation of data, and drafting and critical revision of the manuscript and gave final approval of the version to be published. WK was involved in drafting and critical revision of the manuscript for important intellectual content. PLCMvR and MAFJvdL were involved in designing and management of the DREAM registry; in the conception and design of the study and in drafting and critical revision of the manuscript for important intellectual content. MF, AAdB, AH and HV were involved in local project coordination, acquisition of data and drafting of the manuscript.
-
Funding Funding for the data collection for the DREAM cohort was obtained from the Dutch affiliations of Pfizer Pharmaceuticals, Abbott Pharmaceuticals, Schering-Plough Corporation, Roche Pharmaceuticals, UCB Pharma and Bristol-Myers Squibb. No one except the authors were involved in the design, analyses, interpretation of results and writing the manuscript.
-
Competing interests None.
-
Ethics approval Medical ethical committee Arnhem Nijmegen.
-
Provenance and peer review Not commissioned; externally peer reviewed.