Article Text

Abstract
Background A high percentage of patients with systemic sclerosis (SSc) develop interstitial lung disease (ILD) during the course of the disease. Promising data have recently shown that lung ultrasound (LUS) is able to detect ILD by the evaluation of B-lines (previously called ultrasound lung comets), the sonographic marker of pulmonary interstitial syndrome.
Objective To evaluate whether LUS is reliable in the screening of ILD in patients with SSc.
Methods Fifty-eight consecutive patients with SSc (54 women, mean age 51±14 years) who underwent a high resolution CT (HRCT) scan of the chest were also evaluated by LUS for detection of B-lines. Of these, 32 patients (29 women, mean age 51±15 years) fulfilled the criteria for a diagnosis of very early SSc.
Results At HRCT, ILD was detected in 88% of the SSc population and in 41% of the very early SSc population. A significant difference in the number of B-lines was found in patients with and without ILD on HRCT (57±53 vs 9±9; p<0.0001), with a concordance rate of 83%. All discordant cases were false positive at LUS, providing a sensitivity and negative predictive value of 100% in both SSc and very early SSc.
Conclusions ILD may be detected in patients with very early SSc. The presence of B-lines at LUS examination correlates with ILD at HRCT. LUS is very sensitive for detecting ILD even in patients with a diagnosis of very early SSc. The use of LUS as a screening tool for ILD may be feasible to guide further investigation with HRCT.
Statistics from Altmetric.com
Introduction
Pulmonary involvement is the leading cause of disease-related morbidity and mortality in systemic sclerosis (SSc).1 About two-thirds of patients with SSc develop interstitial lung disease (ILD) with a death rate of about 40% within 10 years from disease onset.2,–,4
Among methods of ILD evaluation, high- resolution CT (HRCT) has been shown to be more accurate than chest x-ray in detecting and characterising pulmonary involvement.5 The pulmonary involvement, as observed at HRCT, correlates closely with pulmonary function test abnormalities.6,–,10 Chest HRCT is presently considered as the diagnostic gold standard for ILD assessment. In patients with SSc, ILD affects juxtapleural, posterior and basilar portions of the lungs, with initially subtle alterations of increased ground glass opacities, defined as increased lung attenuation in the absence of architectural distortion, as well as accentuated reticular markings. These alterations may progress to pulmonary fibrosis, defined as architectural distortion with reticular intralobular interstitial thickening, traction bronchiectasis and bronchiolectasis and honeycomb cystic changes.10,–,13 It would be beneficial to be able to detect pulmonary abnormalities at earlier stages in order to establish appropriate treatment. Unfortunately HRCT cannot be repeated very often because of its cost and particularly for radioprotection issues, since the equivalent radiation dose for a chest HRCT scan is 5–7 milliSievert (mSv) which corresponds to the radiological risk of 250–350 chest x-rays.14
Promising data have recently been obtained by lung ultrasound (LUS) which allows the detection of ILD by the evaluation of B-lines (previously called ultrasound lung comets).15 ,16 B-lines are the sonographic sign of pulmonary interstitial involvement,17 including increased thickness of the pulmonary septa. Traditionally, B-lines have been employed in patients with heart failure to detect the location and quantification of extravascular lung water,15,–,19 but many data suggest their use also in evaluating ILD.17 ,20,–,23 Assessment of B-lines by LUS would represent an attractive biomarker for the frequent evaluation of pulmonary involvement in patients with SSc since it is non-ionising, inexpensive and easy to perform and interpret.
The aim of this study was to verify in patients with SSc the correlation between HRCT signs of ILD and B-lines, and also to evaluate their reliability as a screening tool in patients with a diagnosis of very early SSc.
Methods
Fifty-eight consecutive patients with SSc (54 women, mean age 51±14 years) were evaluated in the outpatient Rheumatologic Clinic of the Department of Biomedicine of the University of Florence from December 2009 to March 2012.
The inclusion criteria were (1) a previous diagnosis of SSc according to the American College of Rheumatology classification criteria for SSc,24 independent of the stage of the disease and organ involvement, or according to the preliminary criteria of very early diagnosis of SSc25; and (2) LUS examination for specific assessment of B-lines performed within 2 months of a chest HRCT scan. Chest HRTC was requested as part of the initial or follow-up evaluation of organ involvement.
Lung ultrasound (LUS)
LUS was performed for the evaluation of the location and number of B-lines on both right and left hemithoraces using commercially available echographic equipment with a 2.5–3.5 MHz cardiac sector transducer 2.5 cm in length (Mylab50, Esaote, Genoa, Italy). The echographic examinations were performed with patients in the supine position for anterior and lateral scanning and in the sitting position for dorsal scanning. LUS examination was obtained by moving the probe longitudinally along anatomical reference lines, as previously described.15 ,17 ,22 The anterolateral chest was scanned on the right and left hemithorax, from the second to the fourth (on the right side to the fifth) intercostal spaces along the parasternal, mid-clavicular, anterior axillary and mid-axillary lines (figure 1A). The posterior chest was scanned on the right and left hemithorax along the paravertebral, scapular and posterior axillary lines, starting from the apex and proceeding downwards until the diaphragm was visible (figure 1B). A demonstration video showing in detail how to perform a whole LUS examination can be freely accessed at the following link: http://www.youtube.com/watch?v=amsULLws8GI.

Scanning technique for (A) anterolateral chest and (B) posterior chest.
A B-line was defined as an echogenic coherent wedge-shaped signal with a narrow origin in the near field of the image.17 In each intercostal space the number of B-lines was recorded. The sum of B-lines yielded a score denoting the extent of ILD. A scan was considered positive either when ≥3 B-lines were found in at least two adjacent scanning sites or when a total of >5 B-lines were present, as previously employed and validated.15,–,19 ,21 ,22 Zero was defined as a complete absence of B-lines in all scanning sites. The full white screen in a single scanning site was considered as corresponding to 10 B-lines. Two observers (TB and LG) with dedicated training and previous experience in LUS acquired and analysed all the LUS studies. The observers were blinded to chest HRCT results and clinical data. The intra- and inter-observer variability in B-line assessment were 5.1% and 7.4%, respectively, as previously described.19
Chest HRCT
HRCT was performed on a spiral CT/I Highspeed GEMs (General Electric Medical Systems, Milwaukee, Wisconsin, USA) scanner with one row of detectors and a rotation time of 1 s. All patients underwent an A-P and L-L scout. After this, 35–55 scans were acquired at the end of inspiration, in apnoea, from the apex to the lung base, either in supine or in prone decubitus. The acquisition parameters were as follows: sequential mode, 1 mm collimation and 10 mm interval, 180–260 mA average tube current (depending on the build of patient) and 120–140 kV tube voltage. A bone plus reconstruction with lung window was used. No intravenous contrast material was administered. The duration of the CT acquisition was 35–45 s. Matrix was 512–512 and the absorbed dose was in the range of 5–7 mSv. Pulmonary involvement was evaluated by topographically dividing the lung in correspondence to the lung lobes.
Pulmonary function tests and echocardiography
Standard spirometry and lung volume measurements were performed in all patients using a fully equipped computerised spirometric system (CPL Morgan Transflow Test PFT System, Morgan Scientific, Haverhill, Massachusetts, USA). Single-breath diffusing capacity for carbon monoxide (Dlco) was also measured. Actual Dlco values were corrected for haemoglobin and carbon monoxide levels. The results were expressed as a percentage of the predicted values.26 ,27
All patients underwent a comprehensive transthoracic echocardiography examination at rest using conventional methods with commercially available ultrasound machines (IE33, Philips Medical Systems, Andover, Massachusetts, USA; Vivid-I, GE/Vingmed, Milwaukee, Wisconsin, USA) equipped with a 2.5–3.5 MHz phased-array sector scan probe, second harmonic technology and coupled with tissue Doppler imaging. Left and right ventricular systolic and diastolic function and valvular function were evaluated according to the recommendations of the European Association of Echocardiography and American Society of Echocardiography.
Statistical analysis
Continuous variables are expressed as mean±SD and/or median (IQR) as appropriate. Categorical variables are presented as counts and percentages. Univariate comparisons were made with χ2 or two-sample t tests as appropriate. Receiver operating characteristic (ROC) curve was used to evaluate the performance of B-lines in predicting the presence of ILD on chest HRCT. The results are expressed as area under the curve (AUC) and the 95% CI for this area. The best threshold was obtained by selecting the point on the ROC curve that maximised both sensitivity and specificity. A p value of <0.05 was considered statistically significant. All statistical analyses were performed using the SPSS/PC software package Version 13 (SPSS, Chicago, Illinois, USA).
Results
Feasibility for LUS was 100% and the time needed for the scan and analysis was always <10 min. The mean time delay between LUS and HRCT was 42±46 days with a median value of 27 days (minimum 0, maximum 179, IQR 0–70 days). Most patients (40/58, 69%) had an interval between the two examinations of ≤2 months. Between patients with an interval of ≤2 months and those with an interval of >2 months there were no significant statistical differences in age (51±14 vs 53±15 years, p=0.66), duration of disease (5±9 vs 2±2 years, p=0.09) or total number of B-lines (46±53 vs 29±36, p=0.17). ILD was detected at HRCT in 88% of the SSc population and in 41% of the very early SSc population (p<0.01). Differences in clinical, instrumental and LUS characteristics between the very early SSc and SSc populations are shown in table 1.
Differences in clinical, instrumental and lung ultrasound data between patients with very early SSc and those with SSc
The mean±SD number of B-lines in the overall population was 14±18 on anterior chest, 25±33 on posterior chest and 40±47 as total number. A statistically significant difference in the total number of B-lines was found in patients with and without ILD on HRCT (mean 57±53, median 43 (IQR 24–84) vs mean 9±9, median 5 (IQR 1–17), p<0.0001; figure 2). Patients with ground glass at HRCT (n=13, 9 with SSc and 4 with very early SSc) had a higher total number of B-lines than patients without ground glass (63±47 vs 33±40, p<0.05). No significant statistical difference in number of B-lines was found between younger (≤50 years) and older (>50 years) patients (31±38 vs 49±54, p=0.16), nor between patients with a shorter (≤1 year) or longer (>1 year) duration of disease (32±49 vs 52±45, p=0.13).

Difference in number of B-lines in patients with and without interstitial lung disease (ILD) on high resolution CT.
Individual patient analysis between LUS and HRCT showed a concordance between the two examinations of 83% (table 2) in the overall population, with a sensitivity of 100%, negative predictive value of 100%, specificity of 55% and positive predictive value of 78%. All 10 discordant cases were false positive at LUS. Among them, two patients showed discrete pulmonary nodules described as likely inactive tuberculosis sequelae. The remaining eight discordant cases always had a total number of B-lines <20. Between discordant and concordant cases, no significant differences were found in cardiac systolic or diastolic left and right ventricular function.
Concordance table for LUS and HRCT
ROC curve analysis was used to confirm the analytical relationship between the number of B-lines and the presence of ILD at HRCT (AUC=0.94, 95% CI 0.89 to 0.99, p<0.0001; figure 3). The presence of a total number of B-lines >5 had a sensitivity of 100% and a specificity of 59%. The presence of a total number of B-lines ≥20 had a sensitivity of 83% and a specificity of 96%.

Receiver operating characteristic curve showing accuracy of lung ultrasound in identifying the presence of interstitial lung disease on high resolution CT.
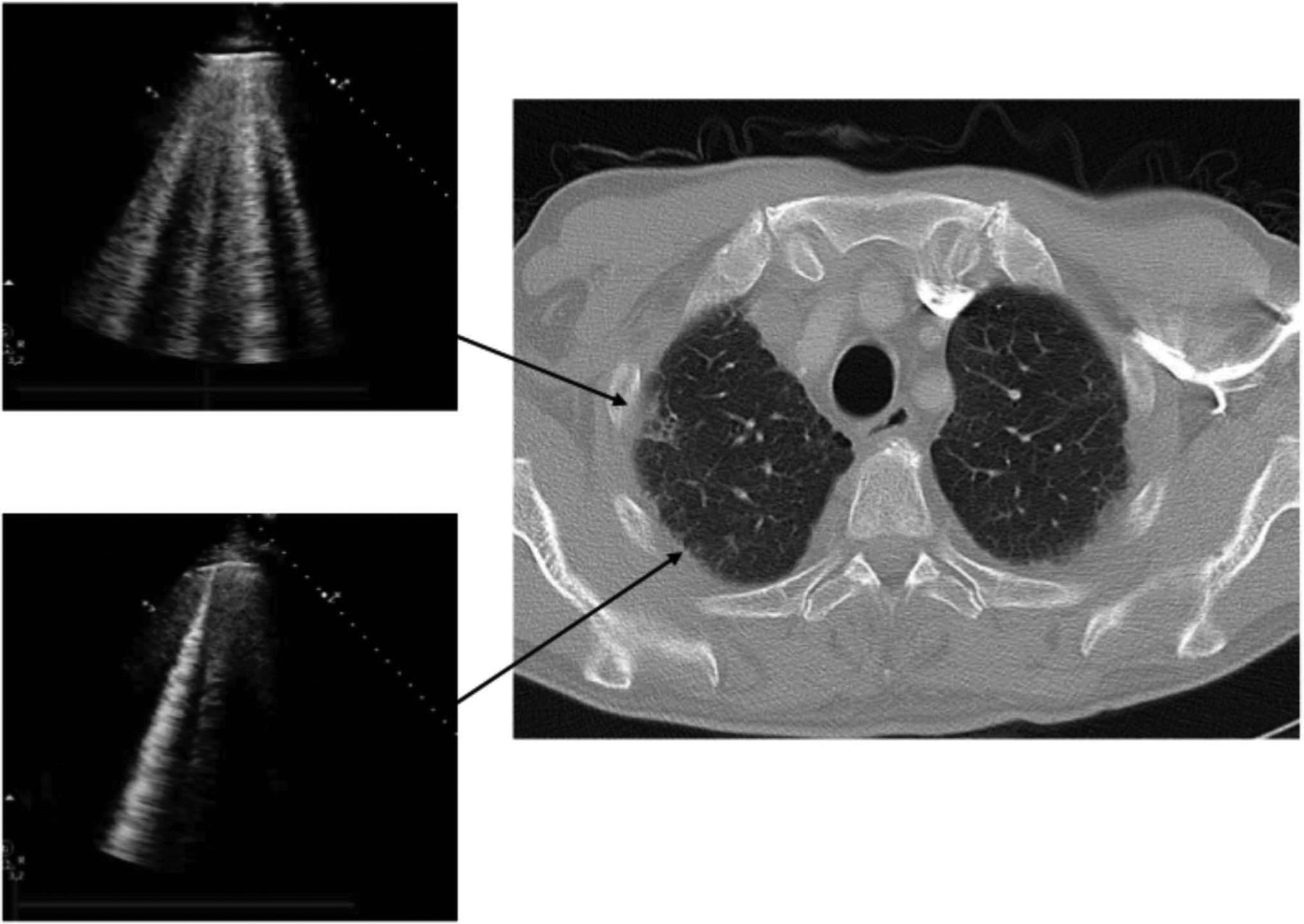
A typical chest HRCT scan showing ILD and the corresponding LUS patterns is shown in figure 4.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
High resolution CT positive for interstitial lung disease and corresponding lung ultrasound patterns.
Discussion
This study shows that LUS is very sensitive for detecting ILD even in patients with very early SSc, and seems reliable as a screening tool to guide further investigation with HRCT. Moreover, it confirms that the presence of B-lines at LUS examination correlates with ILD at HRCT.
Previous studies have demonstrated that LUS may identify ILD in patients with SSc by assessing the number of B-lines.20,–,23 In a previous study on 33 patients with SSc who independently underwent LUS and chest HRCT within 1 week, a LUS score was obtained by totalling the number of B-lines on the anterior and posterior chest and then compared with ILD quantified by HRCT with the previously described 30-point Warrick score.22 A statistically significant positive linear correlation was found between the number of B-lines and the Warrick score. In 1997 Lichtenstein and colleagues first described the presence of B-lines in patients with CT-documented diffuse interstitial pulmonary fibrosis.18 Other studies evaluated this echographic sign in different forms of ILD including pulmonary fibrosis and sarcoidosis, underlining that diffuse parenchymal lung disease should be considered in the presence of multiple B-lines distributed over the whole surface of the lung.20 ,21 Sperandeo et al described the LUS pattern of a more heterogeneous population with pulmonary fibrosis of various degrees23 and found more pronounced LUS abnormalities in patients with more severe degrees of pulmonary fibrosis, as documented at chest x-ray and HRCT.
The clinical impact of LUS for the assessment of ILD could be very significant since it is a highly versatile technique. It is inexpensive, can be performed at the patient's bedside with a hand-held device, the learning and interpretation curves are very short28 and the performance time is very short (<10 min for a total chest assessment). Moreover, the technique is non-ionising and could limit the number of chest HRCT scans, thus reducing the cost and the risk of x-ray exposure.29 Indeed, LUS can easily be combined with standard echocardiography which evaluates other major prognostic determinants in patients with SSc (eg, pulmonary hypertension and cardiac involvement).
However, to date, no other imaging modality is able to provide all the information yielded by chest HRCT which still remains the gold standard technique for assessing ILD.30 ,31 Nevertheless, although LUS will probably never replace the meaningful information obtained with chest HRCT, it could become a useful tool for guiding the use of HRCT. The early screening of ILD seems one of the most appealing settings in which LUS can provide important information. The ability to identify the first signs of ILD with a very high sensitivity could make the use of LUS crucial in the management of patients with SSc (often young women of reproductive age) who require frequent serial testing to assess the natural history of the disease. From the radiobiological viewpoint, we now know that women are more sensitive than men to the carcinogenic effects of radiation (the risk is approximately 37% higher in women than in men) and that the female breast is a highly radiosensitive organ.14 The need to minimise radiation exposure seems especially important in SSc because of the observed puzzling relation between SSc and breast cancer which usually appears on average 20 years after SSc onset.29 ,32
LUS could also provide close follow-up to assess ILD changes during pharmacological treatment, although published data in this setting are still lacking. Indeed, the feasibility, short time required for scanning and the safety profile allow the frequent use of this technique. If these data will be confirmed in a larger cohort of patients, LUS may become a real screening technique in SSc, useful for the early detection of ILD and able to guide the timing of HRCT.
The limitations of B-lines assessment are essentially patient-dependent. Obese patients are frequently difficult to examine because of the thickness of their rib cage and soft tissues. The main limitation of B-lines is the lack of specificity. B-lines are the sonographic sign of pulmonary interstitial syndrome so they are a very sensitive but not specific sign of pulmonary interstitial involvement that may also be present in cardiogenic pulmonary oedema. However, the differential diagnosis is usually obvious from the patient's history and/or from dynamic serial evaluation since only cardiogenic B-lines are cleared by diuretic therapy.15 In this study, however, the presence of B-lines in patients without signs of ILD on HRCT was not related to cardiogenic pulmonary interstitial oedema, since these patients did not show any sign of decompensation and systolic and diastolic left ventricular function was not different between concordant and discordant cases. A limitation of this study is the long time frame between LUS and HRCT, which could also explain some of the discordant cases. Moreover, this pilot study included a relatively small number of patients, so additional studies with a larger SSc population and with all LUS and HRCT performed in a shorter time frame are needed to provide more accurate information on sensitivity and specificity. A comparison with a control group with other diseases involving the pulmonary interstitium would have added important information. However, this was addressed in previous papers21 ,23 which showed data similar to our findings. To date there are no studies correlating LUS with different radiological patterns, especially ground glass or honeycombing areas. Further studies with larger populations and a more detailed comparison between LUS and HRCT are needed to better define whether LUS is able to recognise different radiological features.
In conclusion, given its very high negative predictive value, LUS evaluation of B-lines may help in the screening of ILD in patients with a diagnosis of very early SSc, suggesting the timing for the first HRCT. Our data also confirm previous observations that B-lines are significantly correlated with HRCT. In the future LUS might become a screening technique useful for a precocious and sustainable detection of ILD in patients with very early SSc.
Acknowledgments
The authors would like to thank Dr Simone Angeli for his help in the practical organisation and scheduling of HRCT.
References
Footnotes
TB and LG contributed equally to this work
-
Funding This study was funded by a grant provided by the Regione Toscana, Italy (Regional Health Research Programme).
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Ethics approval was obtained from the Bioethical Committee of the Azienda Ospedaliero-Universitaria of Pisa, Italy.
-
Provenance and peer review Not commissioned; externally peer reviewed.