Article Text

Abstract
Background Analysis of myeloid-related protein 8 and 14 complex (MRP8/14) serum concentrations is a potential new tool to support the diagnosis of systemic-onset juvenile idiopathic arthritis (SJIA) in the presence of fever of unknown origin.
Objective To test the ability of MRP8/14 serum concentrations to monitor disease activity in patients with SJIA and stratify patients at risk of relapse.
Methods Serum concentrations of MRP8/14 in 52 patients with SJIA were determined by a sandwich ELISA. The monitoring of therapeutic regimens targeting interleukin 1 and tumour necrosis factor α, and methotrexate treatment was analysed and diagnostic power to predict flares was tested.
Results MRP8/14 levels were clearly raised in active disease and decreased significantly in response to successful treatments. Serum concentrations of MRP8/14 increased significantly (p<0.001) (mean±95% CI 12.030±3.090 ng/ml) during disease flares compared with patients with inactive disease (864±86 ng/ml). During clinical remission MRP8/14 serum levels of >740 ng/ml predicted disease flares accurately (sensitivity 92%, specificity 88%). MRP8/14 levels correlated well with clinical disease activity, as assessed by physician's global assessment of disease activity (r=0.62), Childhood Health Assessment Questionnaire (r=0.56), active joint count (r=0.46) and with C-reactive protein (r=0.71) and erythrocyte sedimentation rate (r=0.72) (for all p<0.001).
Conclusion MRP8/14 serum concentrations correlate closely with response to drug treatment and disease activity and therefore might be an additional measurement for monitoring anti-inflammatory treatment of individual patients with SJIA. MRP8/14 serum concentrations are the first predictive biomarker indicating subclinical disease activity and stratifying patients at risk of relapse during times of clinically inactive disease.
Statistics from Altmetric.com
Introduction
Systemic-onset juvenile idiopathic arthritis (SJIA) is an aggressive autoinflammatory disease presenting with arthritis, high spiking fever, erythematous rash, lymphadenopathy, hepatosplenomegaly and serositis.1 However, characteristic autoimmune features are not present in SJIA and typical clinical signs such as arthritis may be absent at the onset of disease and especially in patients experiencing a disease flare while receiving anti-inflammatory treatment.
It has already been shown that myeloid-related proteins (MRP) 8 (S100A8) and 14 (S100A9) are useful serum markers for the diagnosis of SJIA in the presence of fever of unknown origin.2 The myeloid-related protein 8 and 14 (MRP8/14) complexes are secreted after activation of phagocytes via a so-called alternative secretory pathway3,–,5 and cause strong proinflammatory effects on phagocytes and endothelial cells in vitro.6 7 They act by binding to Toll-like receptor 4 (TLR4) and form a positive feedback loop with interleukin 1β (IL-1β) in SJIA.2 The loss of control over secretory processes involving the IL-1 family and the damage-associated molecular pattern (DAMP) molecules MRP8/14 may contribute to the pathogenesis of SJIA.2 MRP8 and MRP14 are calcium-binding proteins expressed in granulocytes, monocytes and macrophages during early differentiation stages. Since the activation of the innate immune system is a hallmark of the pathogenesis of SJIA,3 8 MRP8/14 serum concentrations seem to be a good candidate marker for monitoring disease activity as has been already shown in other autoinflammatory diseases.9 Furthermore, MRP8/14 serum concentrations can detect subclinical inflammation in non-systemic JIA and indicate a higher risk of relapse after discontinuation of anti-inflammatory treatment.10
The aim of this work was to evaluate MRP8/14 serum concentrations in relation to disease activity and to investigate if it is a useful tool to affirm reactivation of SJIA and response to anti IL-1 and antitumour necrosis factor (TNF) agents. Furthermore, we studied if MRP8/14 serum concentrations can detect subclinical inflammatory activity that predisposes to reactivation of the disease.
Patients and methods
Patients with systemic-onset JIA
In total, serum samples from 52 patients (median age (range) 11 (2–21) years) who fulfilled the International League of Associations for Rheumatology criteria for SJIA11 were prospectively obtained during the course of disease. Serum samples and routine laboratory parameters were obtained and clinical disease status was recorded at the time of patient examinations. MRP8/14 serum levels were analysed retrospectively and did not influence clinical decisions in the participating centres. The study was approved by the institutional ethics committees, and informed consent was obtained from patients or parents.
Correlation between disease activity and MRP8/14 levels
In 45 of 52 patients (male/female: 20/25, age at disease onset, median (range): 5.7 (2–15) years; follow-up period, median (range): 52 (12–120) months) serum was collected regularly every 3–6 months at control visits or when disease activity changed, analysed at the end of the study and correlated with disease activity (samples/patient, mean (range) 11.5 (6–55)). In the remaining seven patients only data before and after methotrexate (MTX) treatment were available.
Follow-up and subgroup analysis of patients with inactive disease
From the 45 patients mentioned above, 26 patients in remission on medication or with inactive disease off medication were followed up over 6 months with continuous examinations and sample collection at intervals of about 3 months. Patients were included only if they fulfilled the remission criteria and had a complete set of serum samples. Patients without apparent disease activity for at least 6 subsequent months were characterised as ‘non-relapsers’. Patients who experienced a relapse within 6 months were characterised as ‘relapsers’. MRP8/14, C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), high-sensitivity CRP (hsCRP) and ferritin levels were compared during times of remission in both groups in order to investigate the predictive value of these inflammation markers to indicate imminent disease flares.
MRP8/14 concentrations during response to treatment
In 24 of 52 patients response to treatment was analysed. Twelve patients were treated with MTX (13.0–20.6 mg/m2) either orally (five patients) or subcutaneously (seven patients) once a week and were followed up for 6 months. Six patients were treated with recombinant IL-1 receptor antagonist (IL-1Ra) anakinra (Kineret, Amgen, Cambridge, UK; 2 mg/kg/day administered subcutaneously) and were followed up for 9 months. MRP8/14 levels were further analysed before discontinuation of IL-1Ra in four of these patients after a minimum of 12 months of treatment. In six patients, treatment with the soluble TNFα receptor fusion protein etanercept (Enbrel, Wyeth, Muenster, Germany; 0.8 mg/kg/week or 0.4 mg/kg/twice weekly administered subcutaneously) was monitored for 12 months.
Clinical assessment of disease activity
Clinical disease activity was determined according to the core set criteria for JIA.12 13 Patient data collected included medical history, physical examination, number of joints with active disease, number of joints with limited motion, physician's global assessment of disease activity and parent's/patient's assessment of overall well-being (as measured by the Childhood Health Assessment Questionnaire (C-HAQ)). The Juvenile Arthritis Disease Activity Score (JADAS) score was calculated retrospectively.14 Leucocyte count, ESR and CRP levels were determined as measures of inflammation (table 1). CRP levels <5 mg/l were defined as normal values, according to the manufacturer. Serum samples of patients taken during acute infections were excluded from the analysis. Patients were categorised as having active disease (presence of any joint with active disease or signs of systemic disease) or were considered to have inactive disease or disease in remission based on the proposed preliminary criteria,15 including the absence of any systemic symptoms, no active arthritis, and normal CRP and ESR, regardless of medication.16 Relapse was defined according to the preliminary definition of disease flare in JIA.16
Characteristics of the patients with active SJIA (new onset or flare) or inactive disease
Determination of normal MRP8/14 serum levels
Normal MRP8/14 serum concentrations were determined in 50 healthy control individuals without signs of inflammation who were routinely examined at the University Children's Hospital Muenster or who were volunteering laboratory workers. Controls were age-matched to the study group. As previously described, there were no significant differences in serum MRP8/14 concentrations according to age or sex distribution.3 The upper limit of MRP8/14 concentrations in healthy controls was defined as mean plus two SDs.
Laboratory measures
Serum concentrations of MRP8/14 were determined by sandwich ELISA as described previously.3 For comparison with earlier studies, internal control serum samples were used as a reference in all ELISA studies. The readers of the laboratory assay were blinded for diagnosis and inflammatory activity of the patients. A hsCRP test measuring low levels of CRP using laser nephelometry and ferritin analysis by a luminescence immunoassay were applied.
Statistical analysis
Analysis of variance was used to study differences between patient subgroups. Confirmed differences were tested for statistical significance using subsequent selective post hoc testing as described by Dunnett and Tamhane. Rank differences were analysed using the Mann–Whitney U test. Correlations were calculated using Spearman's ρ. Receiver operating characteristic (ROC) curves were plotted to determine the accuracy of inflammation marker measurements as a diagnostic test for a flare. Cox proportional hazards multiple regression analysis was performed to assess the predictive power of laboratory parameters for the risk of relapse. For this analysis, the probability of relapse developing within 6 months (in the presence of abnormal laboratory parameters) in patients with clinically inactive disease was tested. For relapsers, the last blood sample obtained before a relapse was included. For non-relapsers, samples obtained up to 6 months before the end of the individual follow-up periods were included. PASW Statistics 18.0 for Windows (SPSS, Chicago, Illinois, USA) was used for statistical analyses. Unless stated otherwise, data are expressed as the mean±95% CI.
Results
MRP8/14 concentrations reflect disease activity in systemic-onset JIA
Forty-five patients with SJIA were followed up through the course of disease. Samples were obtained at disease onset (20 patients), during disease flares (34 patients) and during inactive disease (all 45 patients). Serum levels of MRP8/14 in patients with new-onset SJIA were significantly raised (mean±95% CI 24.750±11.410 ng/ml) compared with patients with flares (12.030±3.090 ng/ml; p<0.01) and with healthy controls (310±40 ng/ml; p<0.001). MRP8/14 levels among patients with SJIA with inactive disease (864±86 ng/ml) were significantly lower than in patients with active disease but not significantly different from those of healthy controls (figure 1A). Patients with clinical remission on medication (CRM) and inactive disease (ID) on and off medication did not reveal significant differences in MRP8/14 serum levels.

(A) Serum concentrations of myeloid-related protein 8 and 14 protein complex (MRP8/14) in patients with active (new-onset and flare) and inactive systemic-onset juvenile idiopathic arthritis (JIA). Also shown is the serum concentration of MRP8/14 in a group of healthy controls. Box plots show the median (thin horizontal line), the mean (thick horizontal line), and the 25th and 75th centiles. Bars indicate the 10th and 90th centiles. There was a significant difference in MRP8/14 concentrations between patients with active and inactive systemic-onset JIA (***p<0.001) or healthy controls (***p<0.001) (note the break in the y-axis). (B) Receiver operating characteristic curve analysis of MRP8/14, C-reactive protein concentrations (CRP) and erythrocyte sedimentation rate (ESR) displayed as sensitivity against 1–specificity for the differentiation between flare and inactive systemic-onset JIA.
ROC analysis demonstrated a better diagnostic accuracy for MRP8/14 than for ESR and CRP to detect flares. The area under the curve was 0.957±0.019 for MRP8/14, 0.893±0.043 for CRP and 0.889±0.038 for ESR (figure 1B). An MRP8/14 cut-off concentration of 2100 ng/ml had a sensitivity of 92% and specificity of 83% for the diagnosis of a relapse (positive likelihood ratio 11, negative likelihood ratio 0.18). There was a strong correlation between MRP8/14 and the active joint count (r=0.46,), physician's global assessment of disease activity (r=0.62), C-HAQ (r=0.56) and JADAS (r=0.62); MRP8/14 also correlated with concentrations of CRP (r=0.71), ESR (r=0.72) and absolute leucocyte count (r=0.59) (for all p<0.001).
Predictive value for the risk of relapse
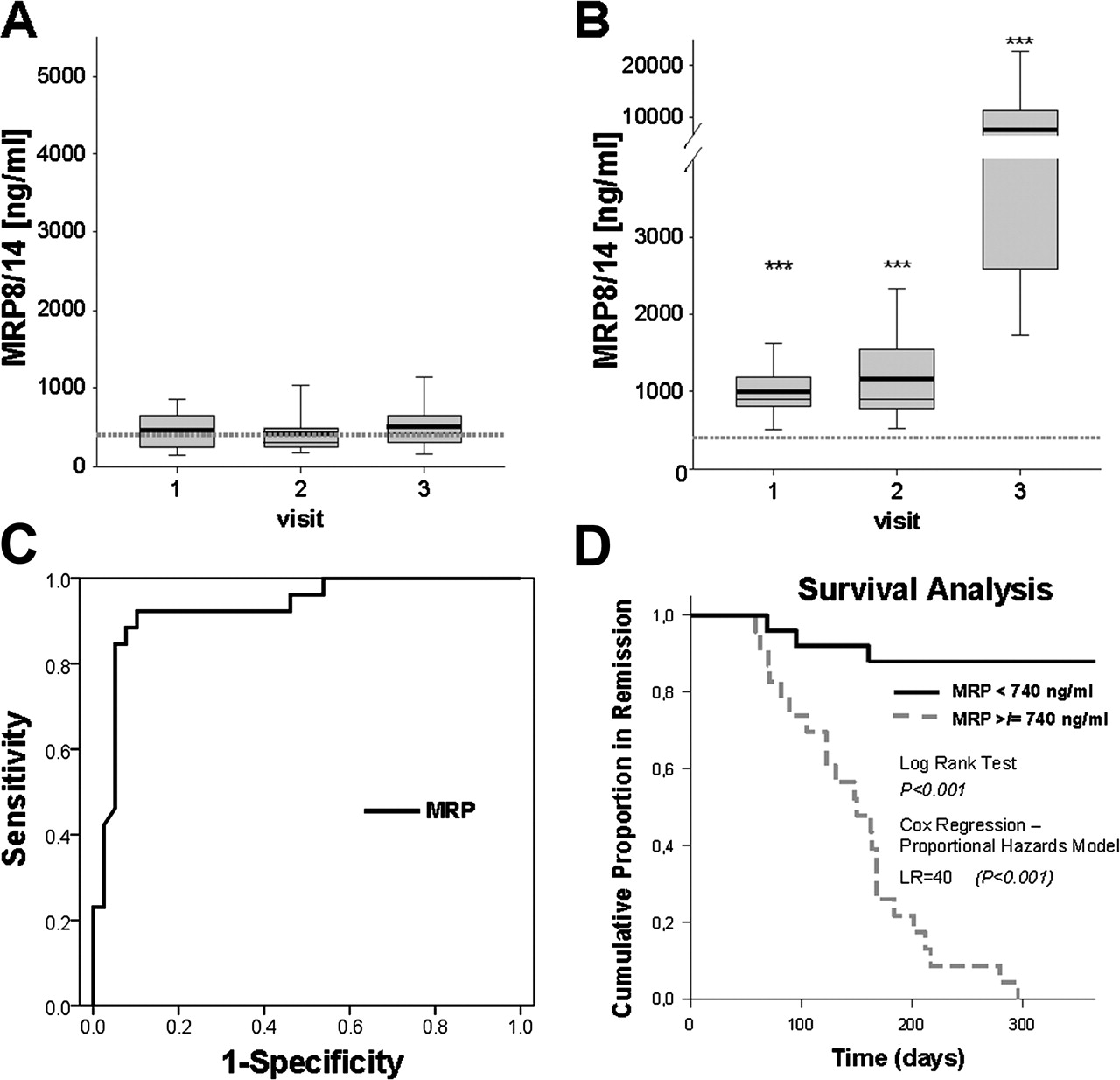
Since a significant number of patients with inactive SJIA whose disease was considered to be in remission still had abnormal MRP8/14 levels, we were interested in the further outcome of these patients. In total, 13 of 26 patients who had been continuously followed up at 3-month intervals after induction of remission on medication or with ID off medication (table 2) had a relapse within the follow-up period (figure 2A,B). The MRP8/14 levels of these relapsers were increased in samples obtained up to 6 months before relapses (1000±206 ng/ml) compared with levels of non-relapsers (458±151 ng/ml) (p<0.001). Significant differences between patient groups with CRM or ID off and on medication could not be found. ROC analyses demonstrated a high diagnostic accuracy for identifying patients at a higher risk of relapse (area under the curve 0.91; p<0.001) (figure 2C). At a cut-off level of >740 ng/ml the test had a sensitivity of 92% and a specificity of 88% to identify patients at risk of relapse, the negative likelihood ratio within the following 3–6 months with MRP8/14 serum concentrations <740 ng/ml was 0.125, which is considered excellent for a diagnostic test.19 By definition, during remission the patients had negative CRP (<5 mg/l) and normal ESR (<20 mm/h) at baseline. Figure 2D shows the cumulative proportional remission in patients with low versus high MRP8/14 levels; exclusion of patients with ID off medication did not change the statistics significantly. These data suggest that MRP8/14 levels are predictive of a relapse up to 6 months before the clinical relapse occurs. Since CRP and ESR have to be normal in remission, we compared the predictive value of the more sensitive inflammation markers hsCRP and ferritin with the predictive value of MRP8/14. None of these additional markers predicted the outcome of patients in remission (table 3).
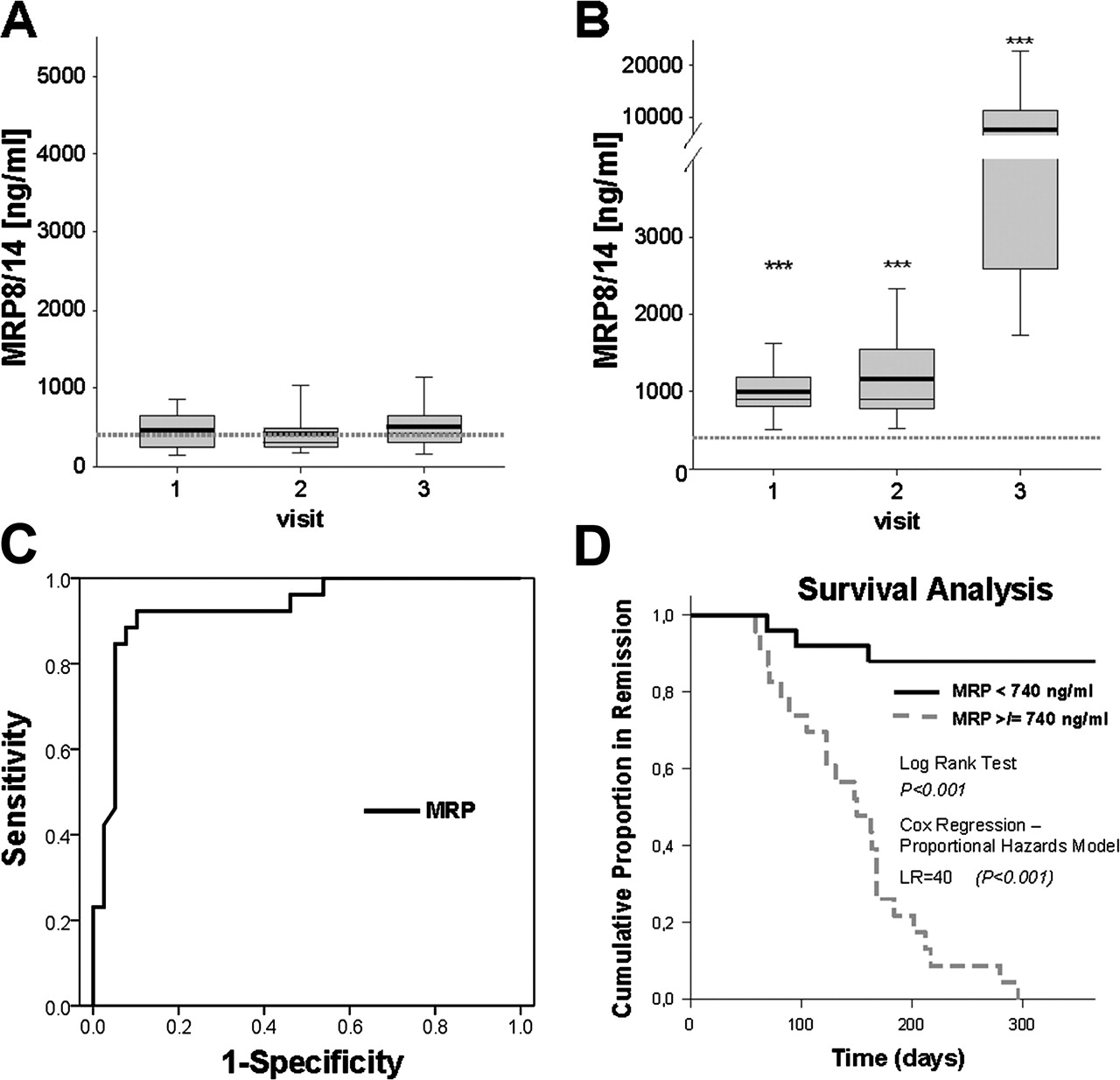
Individual follow-up of patients with systemic-onset juvenile idiopathic arthritis. (A) In 13 patients who were followed up during routine examinations at 3-month intervals, disease remained in stable remission for 6 months after inclusion. The myeloid-related protein 8 and 14 complex (MRP8/14) serum concentrations remained low in these patients over the whole follow-up period. (B) In samples obtained from 13 patients on remission, before a relapse occurred, MRP8/14 concentrations were higher than those in samples obtained from patients with stable remission (***p<0.001 vs A). The grey dotted line represents the normal range. (C) Receiver operating characteristic curve analysis of MRP8/14 concentrations displayed as sensitivity against 1–specificity for the differentiation between patients experiencing a flare and patients in stable remission. (D) Cox proportional hazards multiple regression analysis confirmed the significant association between MRP8/14 serum levels and risk of relapse. The black line represents cumulative remission of patients with MRP8/14 serum concentrations of up to 740 ng/ml, while the light grey broken line represents cumulative remission of patients with higher MRP8/14 levels. The latter group had significantly more relapses within a follow-up period of 6 months. LR, likelihood ratio.
Characteristics of systemic-onset juvenile idiopathic arthritis patients with a relapse (‘relapsers’) or stable remission (‘non-relapsers’) within 6 months follow-up. Course of treatment indicates whether the patients were on a stable treatment, tapered the dose or discontinued treatment after inclusion
Inflammation markers in patients experiencing a relapse (visit 3) (n=13) or being in stable remission over the follow-up period of at least 6 months (n=13)
MRP8/14 concentrations before discontinuation of IL-1Ra treatment
Four patients (three boys aged 15, 18 and 21 years and one girl aged 14 years) with stable remission and receiving IL-1Ra treatment without concomitant steroid-treatment or other anti-inflammatory drugs were included. MRP8/14 levels were prospectively analysed every 3 months during continuing treatment with IL-1Ra. Treatment was discontinued before the last visit and two patients with raised MRP8/14 levels before discontinuation of treatment had a flare of disease while the other two patients with MRP8/14 levels within the range of healthy controls remained in remission without medication for at least a further 3 months, underlining the predictive value of MRP8/14 levels for the identification of stable remission (see online supplementary figure S1).
MRP8/14 concentrations during response to treatment
Treatment with MTX
Samples from 12 patients were analysed before and 6 months after MTX treatment was started. All patients were concomitantly treated with oral prednisolone (0.05–2 mg/kg); two of the responders and one non-responder were also treated with intravenous methylprednisolone (30 mg/kg). Initial MTX dosages were between 13 and 15 mg/m2/week and were escalated in certain patients. Six patients (14.6–17.4 mg/m2 MTX, applied orally in three patients and subcutaneously in three patients) responded to treatment (American College of Rheumatology (ACR) 70 or complete response) and showed a strong reduction of MRP8/14 levels after 6 months of treatment (figure 3A). Six patients (13.1–22.0 mg/m2 MTX applied orally in two patients and subcutaneously in four patients) who did not respond or had a weak response (ACR 30) showed constantly raised or only slightly decreasing MRP8/14 levels (figure 3B).

{kind=link}
{kind=link}
{kind=link}
Decrease of myeloid related protein 8 and 14 complex (MRP8/14) in response to treatment. (A, B) Twelve patients with systemic-onset juvenile idiopathic arthritis (SJIA) were treated with 13.0–20.6 mg/m2 methotrexate once weekly. Samples were obtained before the start of treatment and after receiving medication for 6 months. A significant decrease in MRP8/14 serum levels was seen in those patients responding to treatment (A), while patients without response or response grade ACR30 showed constantly raised MRP8/14 serum levels (B). (C) Remission was induced in six patients with SJIA treated with 2 mg/kg interleukin 1 receptor antagonist daily. Samples were obtained before the start of treatment and after receiving medication for 1, 3 and 6–9 months. (D) Remission was induced in six patients with SJIA treated with etanercept 8 mg/kg weekly or 4 mg/kg twice weekly. Samples were obtained before the start of treatment, and after 3 and 12 months from patients with clinically inactive disease. A significant decrease in MRP8/14 levels was seen in all patients responding to treatment.
Treatment with biological agents (IL-1Ra and anti-TNFα treatment)
Samples obtained from six patients who were treated with IL-1Ra owing to failure of other anti-inflammatory treatments were analysed before anakinra was started and after 1, 3 and 6–9 months. We found an impressive decrease in MRP8/14 concentrations after initiation of IL-1Ra treatment, which was stable for at least 6 months (figure 3C).
Samples obtained from six patients were analysed before etanercept treatment was started and after 3 and 12 months (figure 3D). MRP8/14 concentrations decreased markedly after initiation of treatment and response was stable for at least 12 months. The response in both groups was paralleled by a significant decrease in disease activity (number of active joints, CRP, ESR) (see online supplementary table S1 for patients' characteristics).
Discussion
The diagnosis of SJIA and its further management is still a major challenge for paediatric rheumatologists. In a recent study we showed that serum concentrations of MRP8/14 measured in samples from patients with SJIA are in a range not found in other inflammatory conditions.2 This is of significance because MRP8/14 belongs to the DAMP family of molecules and acts as an endogenous activator of TLR4, which is involved in inflammatory processes of arthritis and autoimmunity.17,–,19 Both proteins are released after inflammatory activation of phagocytes and their serum concentrations correlate well with phagocyte activity in different inflammatory diseases.3 9 It is well known that high concentrations of IL-1 are not found in SJIA.20 However, the biological relevance of IL-1 is confirmed by the efficiency of anti-IL-1 treatment in SJIA. We have shown that MRP8/14 is the serum factor responsible for IL-1β release in systemic-onset JIA.2 While IL-1 measurements are of little help in the clinical routine setting, MRP8/14 are stable proteins that can easily be analysed, thus providing insight into the activation of immune mechanisms involving the IL-1 axis that is crucial during SJIA.2
When the diagnosis of SJIA has been established, therapeutic approaches aim to suppress inflammation, resulting in disease remission. However, the assessment of innate immune activity is not easy, although it is probably the key to successful disease management in SJIA. In addition, SJIA is a heterogeneous entity. It has been shown that a variable number of patients with SJIA do not respond to IL-1 blockade.21,–,23 Therefore there has been discussion as to whether SJIA encompasses different subtypes or stages defined by their response to anti-IL-1 treatment. Regardless of the chosen drug—that is, methotrexate or biological agent—our results suggest that MRP8/14 serum concentrations closely reflect disease activity, response to treatment and also, failure of response to treatment. The additional ability to detect disease flares with a higher sensitivity than CRP or ESR makes the assessment of these biomarkers a valuable tool in the clinical follow-up of patients with SJIA. Acute infections have to be ruled out in patients to avoid false-positive results.
While most patients benefit from the treatments temporarily, many of them have recurrent disease activity after tapering or withdrawing treatment. Only 53% of patients with JIA treated with etanercept retain remission over a median of 0.8 years after discontinuation of treatment.24 Therefore a thorough immune surveillance and evaluation of disease activity is important in monitoring the success of treatments and in detecting subclinical immune activation that may predispose the patient to relapse. With the tools available to date, it is not possible to predict the outcome after stopping treatments. With our present results we show the sensitivity of MRP8/14 serum levels (95%) to differentiate patients in remission on medication as prone to a relapse or not. Remission in patients with SJIA should not only be defined by clinical symptoms or raised CRP or ESR levels. We suggest that the status of ‘immunological remission’ should include additionally determination of MRP8/14 serum levels.3 25 Our analysis of IL-1Ra-treated patients with SJIA in remission on medication confirmed these results. In a recent controlled trial the ability of these biomarkers to predict a relapse after withdrawal of MTX in non-systemic JIA has already been shown.10 In SJIA, suboptimal disease control in patients with ongoing inflammatory activity may predispose the patient to both disease flares and to long-term systemic complications.
Although this is the largest biomarker study in SJIA, our study has some limitations owing to the number of cases. Since SJIA is a rather rare disease, it is not easy to collect patient cohorts systematically. Therefore, serum was collected from patients with SJIA regardless of the severity of the disease. No patients were excluded from the analysis, if clinical diagnosis of SJIA was once established. Study of larger cohorts will be important to further prove the accuracy of MRP8/14 analysis in this context.
Interleukins as biomarkers in SJIA are discussed as well. Peripheral blood mononuclear cells from patients with SJIA were shown to release higher amounts of IL-1 in the study by Pascual et al, while Gattorno et al could not find raised IL-1 levels in patients with SJIA.23 IL-6 seems to have an important role in the pathogenesis of SJIA and as a biomarker in active disease.26 Its importance has been shown by the good response of patients with SJIA to the anti-IL-6 antibody tocilizumab.27 However, another study showed that IL-6 and other proinflammatory cytokines such as IL-12 and TNFα are upregulated in all active categories of JIA. In contrast, IL-18 can identify active patients with SJIA among other JIA categories; no prospective data during the course of SJIA are available.20 Although tools for analysis of interleukin are available, their usefulness for monitoring disease activity has not been demonstrated. A major problem in daily practice is the degradation of these cytokines,28 whereas MRP8/14 complexes are stable, which enables sending samples at room temperature and long-term storage.
Together, our study shows that analysis of MRP8/14 serum concentrations is a useful tool for monitoring disease activity in SJIA. It confirms the diagnosis of relapses and reflects response to treatment with different treatment regimens. Furthermore, MRP8/14 levels reflect continuing subclinical inflammatory activity in patients with clinical remission and can identify patients at risk of relapse. Therefore they are a potentially new tool for therapeutic management and, in particular, might support the decision to discontinue a drug. Nevertheless, larger controlled trials are needed to confirm the usefulness of this marker in daily clinical practice.
Acknowledgments
The authors thank Melanie Saers, Susanne Schleifenbaum and Jerzy-Roch Nofer for excellent technical assistance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
-
Funding Supported by grants from the Interdisciplinary Centre for Clinical Research at the University of Muenster (project Foe2/005/06 and Ro2/004/10), the Deutsche Forschungsgemeinschaft (DFG project FO 354/2-2), the Innovative Medizinische Forschung (IMF project WI 120733), the Bundesministerium für Bildung und Forschung (AID-NET, project 01GM08100), FP7 programme (Pharmachild; GA-No 260353), SPARKS-UK (08ICH09) and the Big Lottery Fund UK (RG/1/010135231). The development and maintenance of the ABC Register has been unconditionally supported by the Dutch Board of Health Insurances (from 2003 to 2006), Pfizer (formerly Wyeth International, since 2007), and Abbott (since 2010).
-
Competing interests None.
-
Ethics approval Ethics committee, University of Muenster, Germany and Institute of Child Health / Great Ormond Street Hospital , London, UK..
-
Provenance and peer review Not commissioned; externally peer reviewed.